Clinical Presentation
A 68-year-old Asian woman had radiation therapy for early-stage cervical cancer about 40 years ago in Asia and remained cancer free for a long time but unfortunately developed recurrent cervical cancer. She was offered an anterior pelvic exenteration by the gynecological oncology service and an ileal conduit by the urology service. The plastic surgery service was asked to perform a vaginal reconstruction after anterior pelvic exenteration and ileal conduit. She was prepared for multiple surgical procedures in the same setting by three surgical services, each performing a specialty procedure for an optimal outcome ( Fig. 37.1 ).

Operative Plan and Special Considerations
A vertical rectus abdominis myocutaneous (VRAM) flap is a classic option for vaginal reconstruction and soft tissue filling of the dead space within the pelvic cavity. With an appropriate design, the flap can carry a sizable skin paddle for the vaginal reconstruction but only sacrifice a small amount of the anterior rectus sheath if perforators can be identified and incorporated within the skin paddle. The flap can be completely elevated and tunneled through the pelvis to fill the dead space within the pelvic cavity and a reconstructed vagina, formed by folding the skin paddle of the flap into a tube, can be brought out for closure of the perineal wound at the same time. If a smaller amount of the anterior rectus sheath is harvested with the flap, the actual fascial defect can be closed and no mesh is needed for the abdominal donor site closure.
Operative Procedures
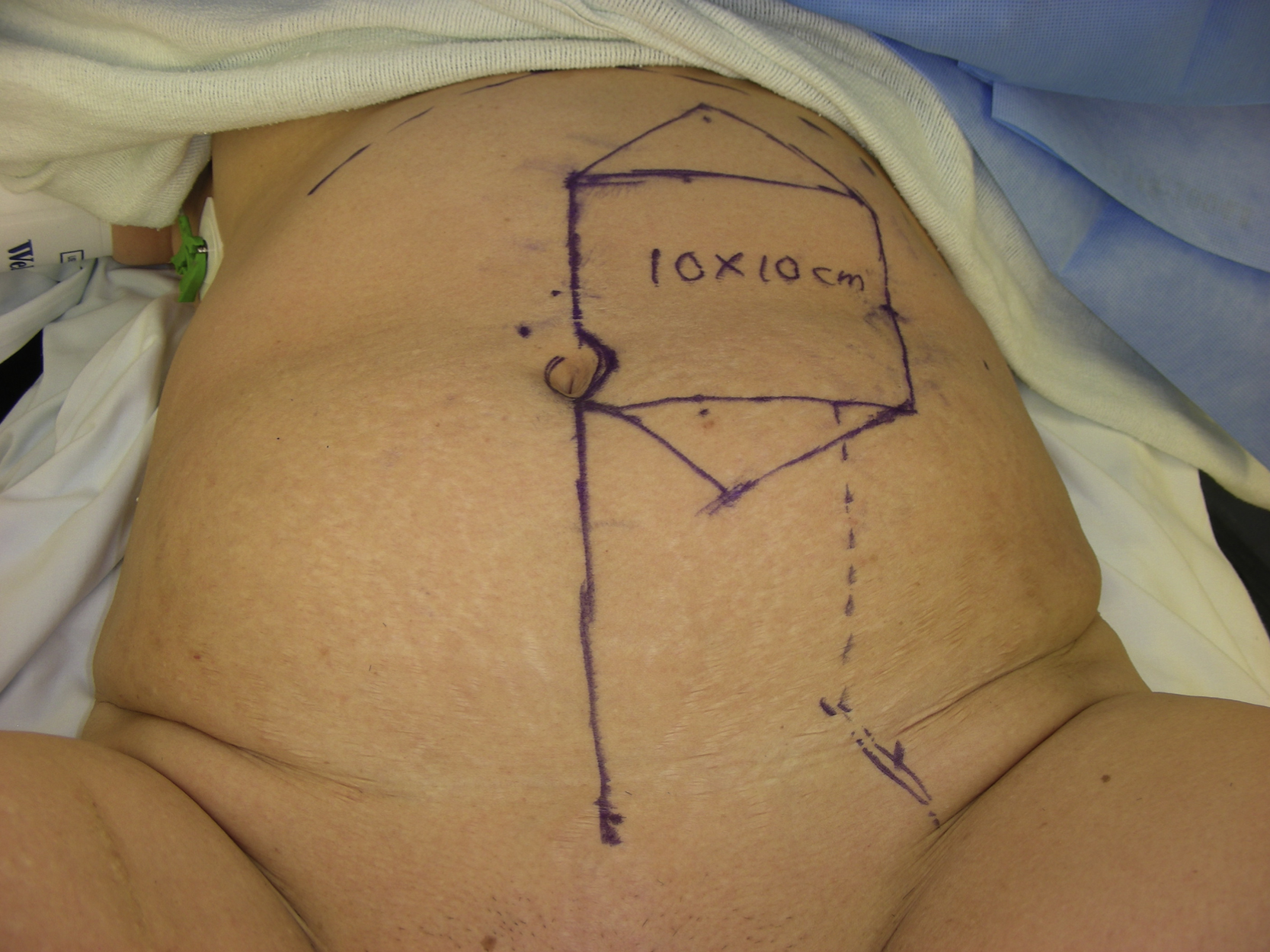
Under general anesthesia with the patient in the lithotomy position, anterior pelvic exenteration was completed by the gynecological oncology service through a midline laparotomy. After careful assessment of the left abdominal wall including the left inferior epigastric vessels, a left VRAM flap was performed as planned. Two perforators were identified with a hand-held Doppler and marked and incorporated within the skin paddle design of the flap. A 10 × 10 cm skin paddle was designed from the midline based on the pinch test and potential excess skin for the closure of the abdomenal skin defect was incorporated with the skin paddle design ( Fig. 37.2 ). The skin paddle was incised down to the anterior rectus sheath. The suprafascial dissection was performed to identify the perforators. In this way, only a small portion of the anterior rectus sheath was sacrificed during the flap elevation.
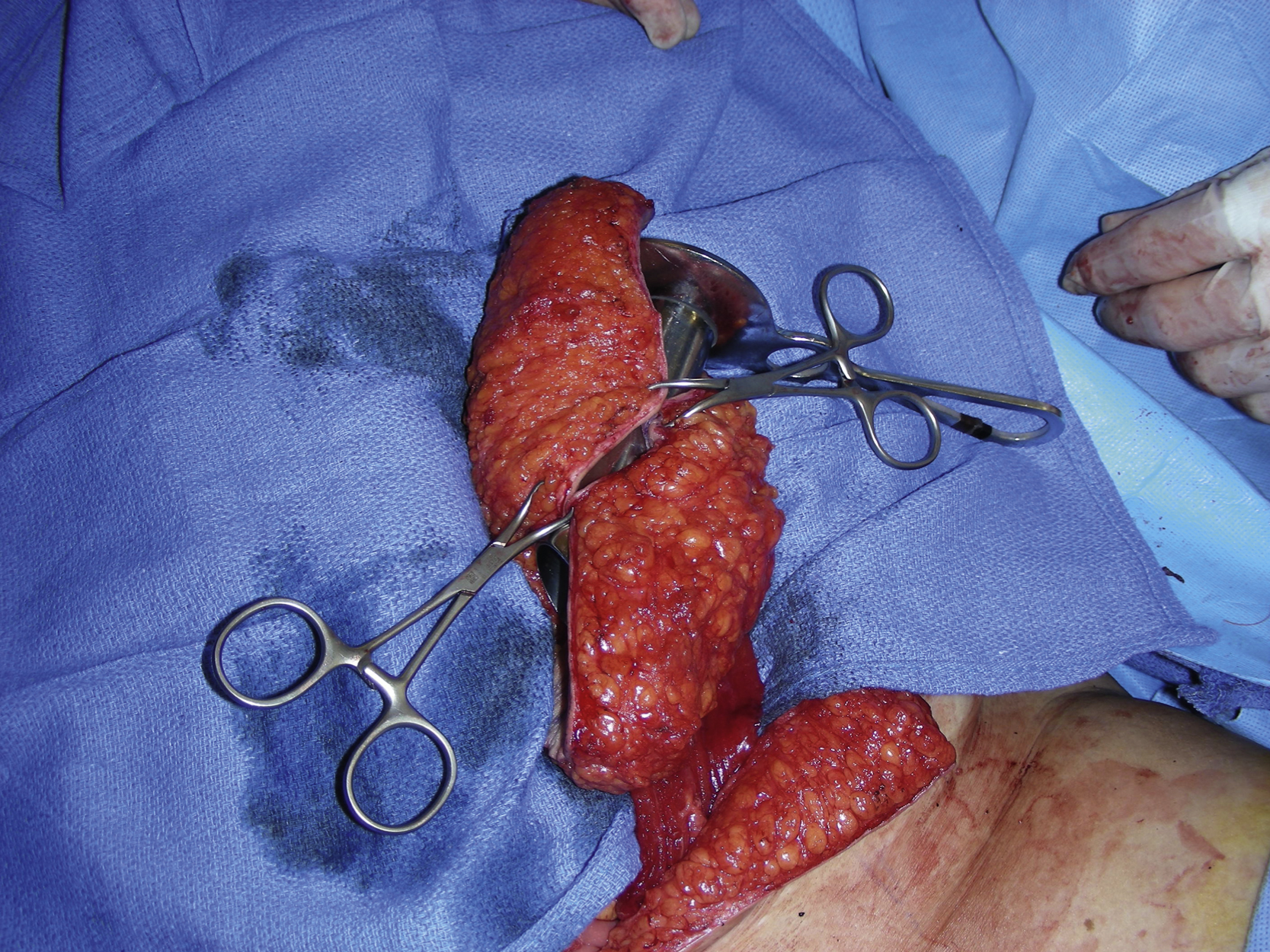
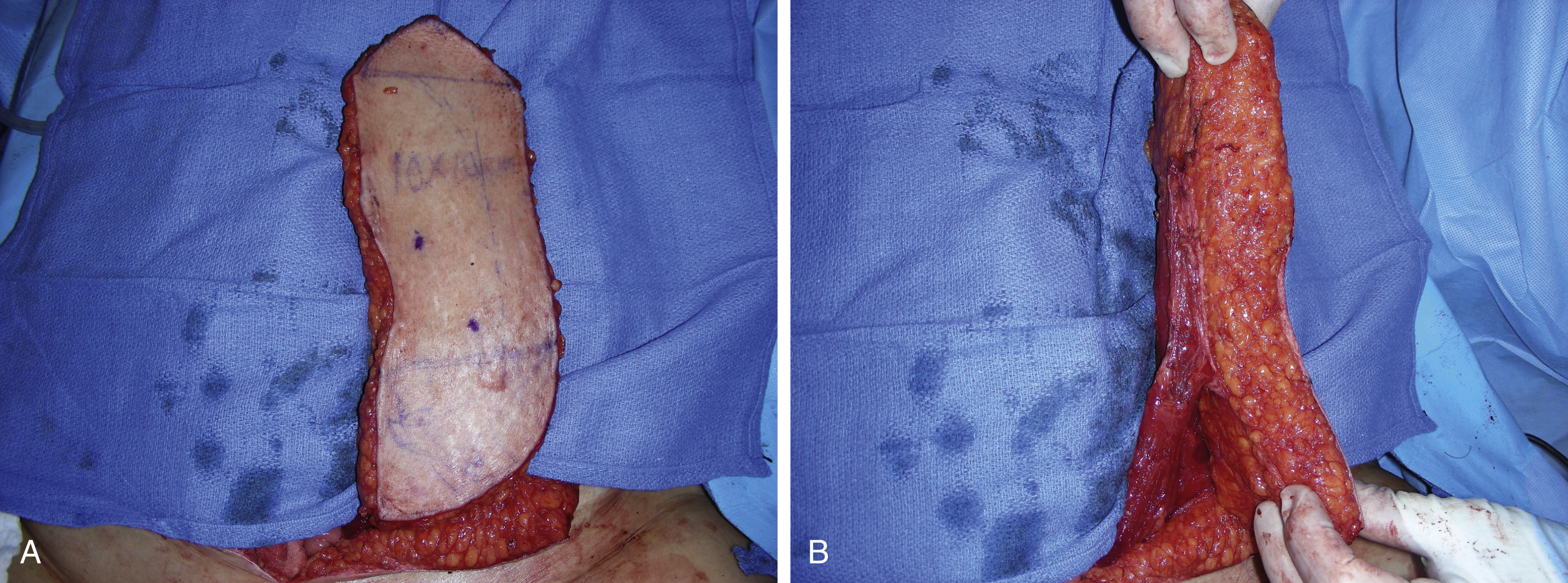
Further dissection was performed to free the muscle more proximally and the superior rectus abdominis muscle was divided with electrocautery. The muscle flap was elevated from the posterior rectus sheath. During dissection, several intercostal nerves were identified and divided with hemoclips. Inferiorly, the muscle was dissected free toward its insertion. The muscle flap was then completely elevated based on the inferior epigastric vessels ( Fig. 37.3 A ). The anterior rectus sheath was tacked to the subcutaneous tissue with 3-0 Vicryl sutures to prevent shear force ( Fig. 37.3 B). The pedicle dissection was performed within the pelvis under direct vision. The entire flap was easily turned over and tunneled through the pelvic cavity and brought out in the perineal opening without any tension.
The new vagina was then created using the skin paddle of the flap. With a 3-cm diameter stand, a spiral type of closure was performed to form a new vaginal canal ( Fig. 37.4 ). This was done in two layers. The deep tissue layer was approximated with several interrupted 2-0 Vicryl sutures in figure-of-eight fashion and the skin was approximated with several interrupted 2-0 Vicryl sutures ( Fig. 37.5 ). The proximal end of the reconstructed vagina was approximated with 2-0 Vicryl sutures, once again in two layers ( Fig. 37.6 ). The entire flap was tunneled through the pelvis and brought out in the perineal opening ( Fig. 37.7 ). Two 15-Fr Blake drains were inserted in the pelvis and brought out in the buttock area. At this point, the urology service started the ileal conduit procedure through the right abdomen.