Case 1
Clinical Presentation
A 51-year-old White male had a basal cell cancer over his left medial cheek and nasal sidewall. Mohs surgery was performed by our dermatological surgeon and the skin resection margins were all negative. The patient had a 6 × 2.5 cm skin defect involving the medial cheek and nasal sidewall near the medial canthus ( Fig. 3.1 ). The plastic surgery service was asked to close this complex skin defect after a definitive cancer resection. The patient was also a heavy smoker and was unable to stop smoking prior to surgery.

Operative Plan and Special Considerations
Based on an analysis of the defect involving the medial cheek and nasal sidewall, the medial cheek advancement could be designed to cover the cheek defect and a portion of the nasal sidewall defect and a full thickness skin graft could also be used to cover the rest of the defect in the nasal sidewall.
Operative Procedures
The medial cheek advancement flap was designed superiorly parallel to the lower eyelid and medial to the nasolabial fold ( Fig. 3.2 ). The flap area was infiltrated with 1% lidocaine with 1:100,000 epinephrine.

The flap was elevated under direct vision at the subcutaneous tissue plane and the area of the skin flap elevation measured 15 × 10 cm ( Fig. 3.3 ). With a scissor dissection, the medial cheek skin flap was elevated and advanced to cover the entire medial cheek defect along with some of the inferior portion of the nasal sidewall ( Fig. 3.4 ). Several tacking sutures were used with 4-0 nylon suture to hold the skin flap and facilitate closure of the defect. On the nasal side wall, the skin flap was also approximated to the nasal sidewall skin with 4-0 nylon sutures in half-buried horizontal mattress fashion. Some excess skin was excised for better donor site closure. The medial inferior portion of the flap was sutured to the nasal labial fold skin with 4-0 nylon sutures in simple interrupted fashion. The lower eyelid incision closure was done in the deeper dermal layer with 5-0 Monocryl sutures in a simple interrupted fashion, followed by the 5-0 nylon sutures for skin closure in a simple running fashion.


The excess portion of the distal flap was excised. This portion of the skin, which measured 2 × 1 cm, was defatted and placed over the left nasal side wall defect and secured with multiple 5-0 chromic sutures ( Fig. 3.5 ). The skin graft was sutured to the wound bed and then secured with a tie-over dressing for skin graft immobilization.

Follow-Up Results
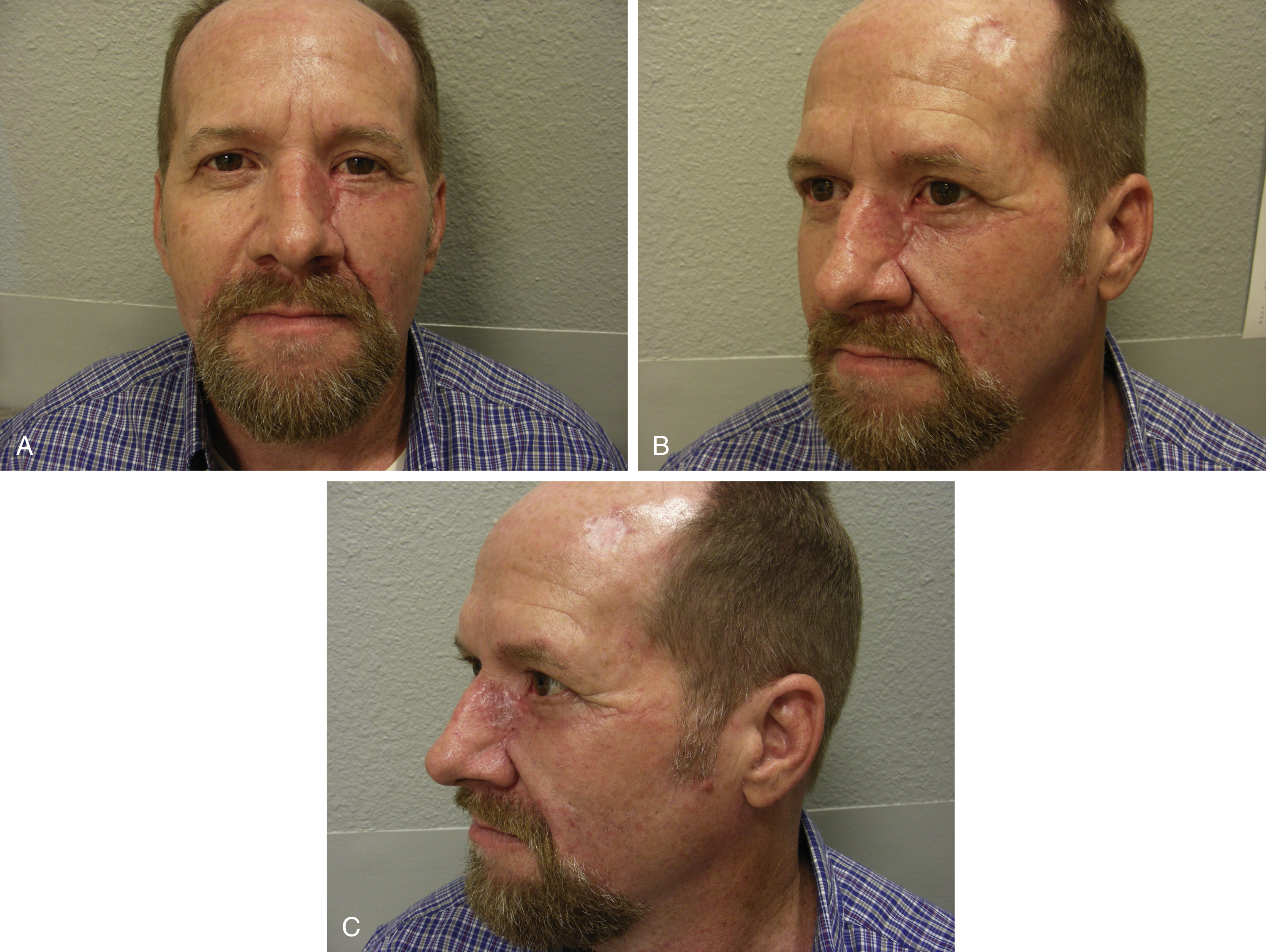
The patient did well postoperatively without any complications related to the medial cheek advancement flap. He was observed overnight in the hospital and discharged home the next day. His tie-over dressing was removed at postoperative day 5. The flap and skin graft sites both healed well. There was no entropion over his left lower eyelid ( Figs. 3.6A–C ).
Final Outcome
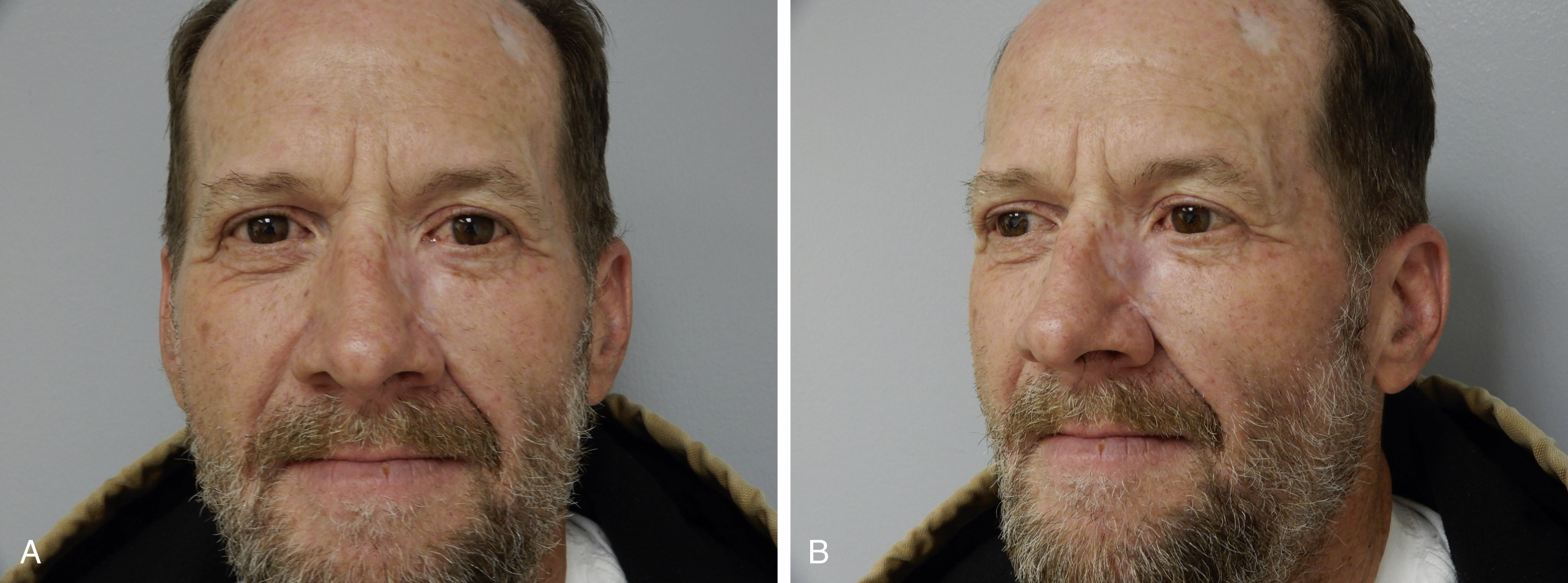
The medial cheek advancement flap to the medial cheek defect and full thickness skin graft to the nasal sidewall defect healed well without any issues. The patient has had a reasonably good cosmetic outcome and minimal scarring ( Fig. 3.7A and B ). He returned to normal life and has been followed by our demonologist for routine skin cancer follow-up.
Pearls for Success
The medial cheek advancement flap can be elevated to cover a medial cheek and even a portion of the nasal sidewall defects if the patient has some skin laxity in the cheek. The flap is elevated at the subcutaneous tissue plane above the fascia of the superficial musculoaponeurotic system. Superiorly it is parallel to the lower eyelid and medially it follows the nasolabial fold. Attention should be paid not to traumatize the orbicularis oculi muscle. Preoperative evaluation of the lower eyelid position may be helpful to predict whether the patient would need a lateral canthopexy. In a smoker, the distal portion of the flap may not be reliable. For this case, it was converted to a full thickness skin graft. With proper immobilization postoperatively, the full thickness skin graft can heal well and provide even better contour of the nasal sidewall for reconstruction.
Case 2
Clinical Presentation
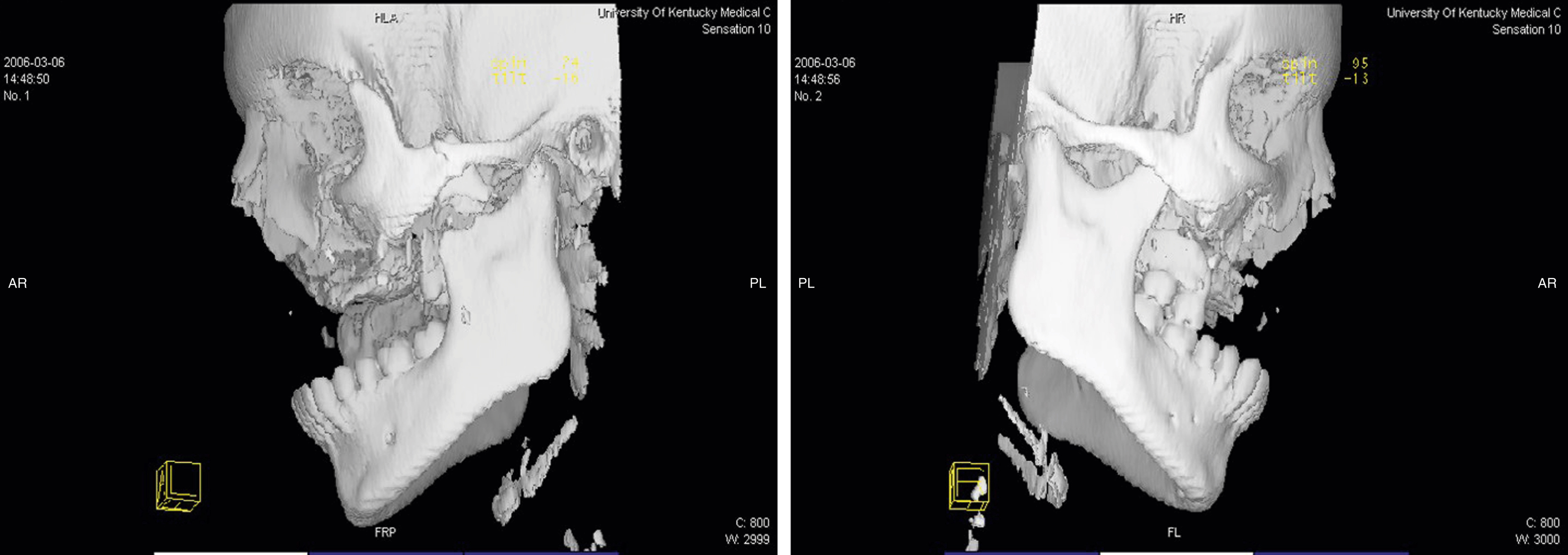
A 19-year-old White female sustained comminuted fractures of her maxilla secondary to a motor vehicle accident. She was managed by an outside hospital initially for the soft tissue injury and acute trauma conditions and was transferred to our plastic surgery service for definite reconstruction of her middle facial bony defect. On examination, she had a significant midfacial collapse ( Fig. 3.8 ). Intraoral examination showed poor quality and scarred gum tissue over the old fracture site. Her facial bone CT scan showed a significant bony defect in the central portion of the maxilla and a missing small bony portion of the nasal dorsum ( Fig. 3.9 ).

Operative Plan and Special Considerations
This patient was also evaluated by our oral surgery service. A dental model was made for her and it showed the exact 8-cm bony defect of the maxilla and the amount of vascularized bone graft needed for such a reconstruction ( Figs. 3.10 and 3.11 ). Because of the need for maxillary bony reconstruction and the poor quality of her intraoral soft tissue, a free fibula osteocutaneous flap reconstruction was offered to this patient. Because the dental model had been made, the bony reconstruction could be performed simultaneously for potentially improved occlusion and future osteointegrated dental implants. A preoperative angiogram was performed to confirm a normal vascular structure of both legs.


Operative Procedures
The procedure was started by two teams simultaneously. Her old maxillary fracture site was explored by the oral surgery service. Her scarred gum tissue was removed and the residual maxillary fracture sites were explored. All of the mini bony fragments were removed. Her maxilla bony defect was confirmed as 8 cm after a direct measurement.
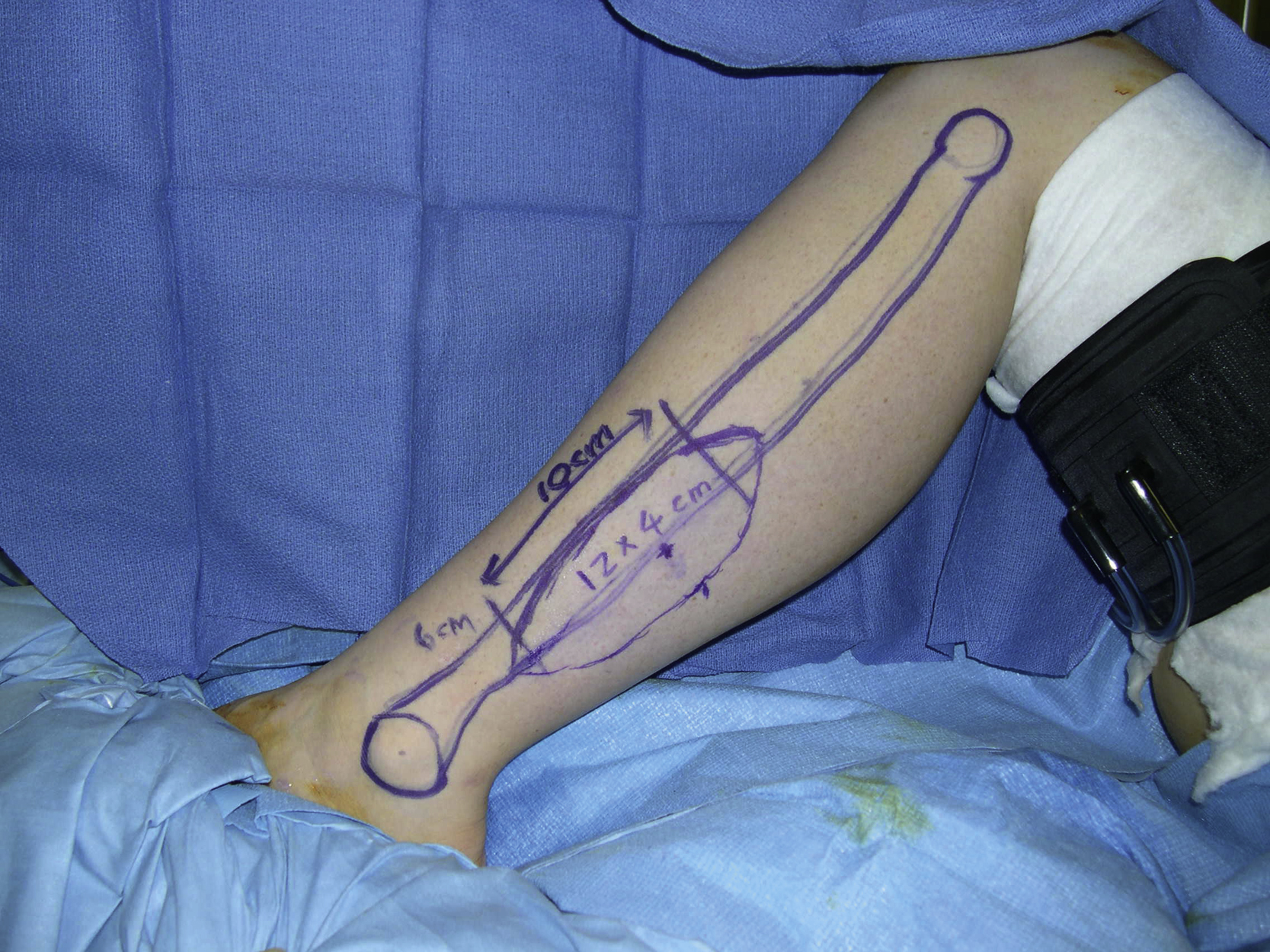
The left free fibula osteocutaneous flap was harvested by the plastic surgery service. A 12 × 4 cm of the skin paddle was designed ( Fig. 3.12 ). Under tourniquet control, the skin paddle was incised through the fascia. The subfascial dissection was performed toward the posterior intermuscular septum ( Fig. 3.13 ). Two septocutaneous perforators were identified in the septum. Attention was made to avoid direct or indirect injury to those perforators. The dissection was made to release the muscle attachment to the fibula from the soleus muscle. Once the peroneal vessels close to the fibula were identified, the distal osteotomy was performed at a level of about 6 cm proximal to the lateral malleolus. By further dissection of the hallucis longus muscle’s attachment, the peroneal vessels and the fibula were dissected free. The proximal osteotomy was then performed and a 10-cm segment of the fibula was obtained. A longitudinal skin incision was extended further toward the fibular head. Following more dissection around the pedicle, the peroneal vessels were dissected free toward its bifurcation with the posterior tibial vessels. Once the bifurcation was visualized, the pedicle was divided and the flap’s dissection was completed ( Fig. 3.14 ). With the guide of the dental model, two osteotomies were performed on the nonperiosteum attachment side ( Fig. 3.15 ).