Clinical Presentation
A 30-year-old White female sustained severe neck contracture from a previous burn injury about 5 years ago. She had excision of the deep burn wound and skin grafting in a local hospital but unfortunately developed severe anterior neck scar contracture ( Fig. 11.1 ). She reported severe limitation of the range of motion (ROM) in her neck especially neck extension and requested a surgical release of the scar contracture so that her neck ROM could be improved ( Fig. 11.2 ).


Operative Plan and Special Considerations
A complete surgical release of the neck scar contracture should be done first. This would create a sizable skin defect that could be reconstructed with several options. Integra wound closure would be the simplest option, but its success may not always be reliable based on this author’s experience. Tissue expansion could be a viable option for some patients but unfortunately this patient had burn and skin graft on her adjacent upper chest. A free anterolateral thigh (ALT) perforator flap can be a good option if the flap could be transferred successfully to the neck after microvascular anastomoses. In this case, neck recipient artery and vein should be dissected first before an ALT flap dissection is started.
Operative Procedures
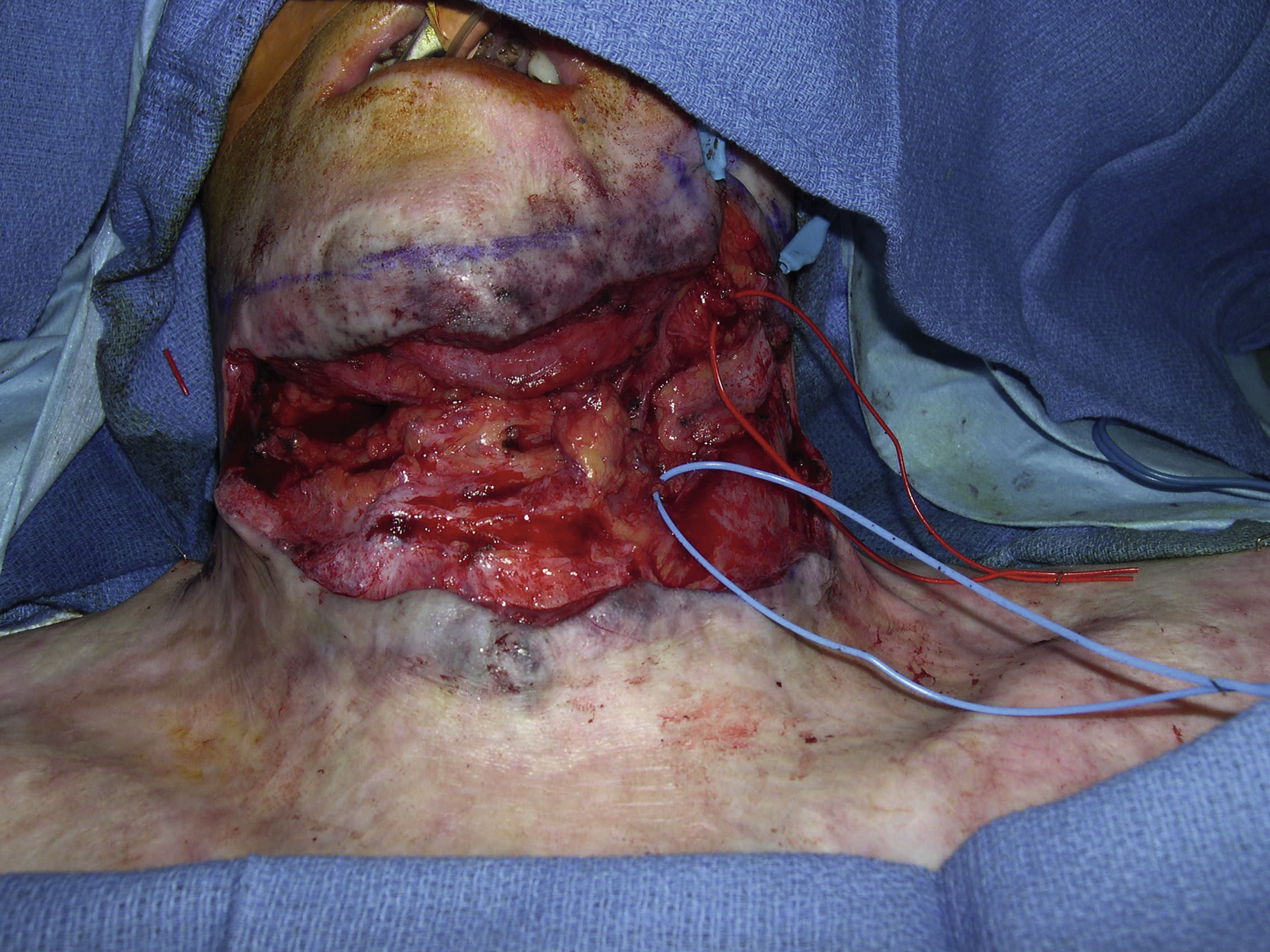
Under general anesthesia, the patient was taken to the operating room for release of the neck scar contracture and a planned free ALT perforator flap. The scar contracture was completely released once the incision was made at the base of the neck scar. After an extensive surgical dissection, the size of the neck soft tissue defect was measured as 16 × 9 cm ( Figs. 11.3 and 11.4 ). The left facial artery and superior thyroid vein were dissected as recipient vessels for microvascular anastomoses.

A standard right ALT perforator flap was marked and two perforators were identified by a handheld Doppler ( Fig. 11.5 ). Unfortunately, after the skin paddle of the flap was elevated, the previously identified perforators were not found. During further flap dissection, a large perforator near the proximal side of the flap was identified ( Fig. 11.6 ). The perforator appeared to be of adequate size (approximately 3 mm). There was a strong signal based on the handheld Doppler. Based on the principles of free-style free flap, the intraoperative decision was made to convert the free ALT flap to a free-style free flap ( Fig. 11.7 ). A lengthy and challenging intramuscular dissection was performed until the length of the pedicle was determined to be adequate and the diameter of the pedicle was big enough for microvascular anastomoses ( Fig. 11.8 ). The pedicle was divided and the free-style free flap dissection, based on the same donor site, was completed ( Fig. 11.9 ).










