Clinical Presentation
A 40-year-old White male had previously sustained a gunshot wound to his mandible and left mandibular bony reconstruction was unsuccessful. He had a significant deformity of his left lower face and desired a “good” mandibular reconstruction, not only to improve his lower face contour and deformity but also to have possible future reconstruction for osteointegrated dental implants ( Figs. 5.1 and 5.2 ). A preoperative CT scan of his mandible was performed.


Operative Plan and Special Considerations
This patient was also evaluated by our oral surgery service. After a careful preoperative evaluation of the mandible including a dental model, a large, approximately 10-cm mandibular bony gap of the mandible was identified ( Fig. 5.3 ). Because of the need for mandibular bony reconstruction, the future need for osteointegrated dental implant reconstructions and anticipated need for a skin coverage of the newly reconstructed mandible, a free fibula osteocutaneous flap reconstruction was offered to this patient. Because the dental model had already been made, a prebent 2.4-mm reconstruction plate was made preoperatively for secure occlusion and time saving in the operating room for plating the vascularized fibular bone graft. A preoperative angiogram was also performed to confirm a normal vascular anatomy of the left lower extremity.

Operative Procedures
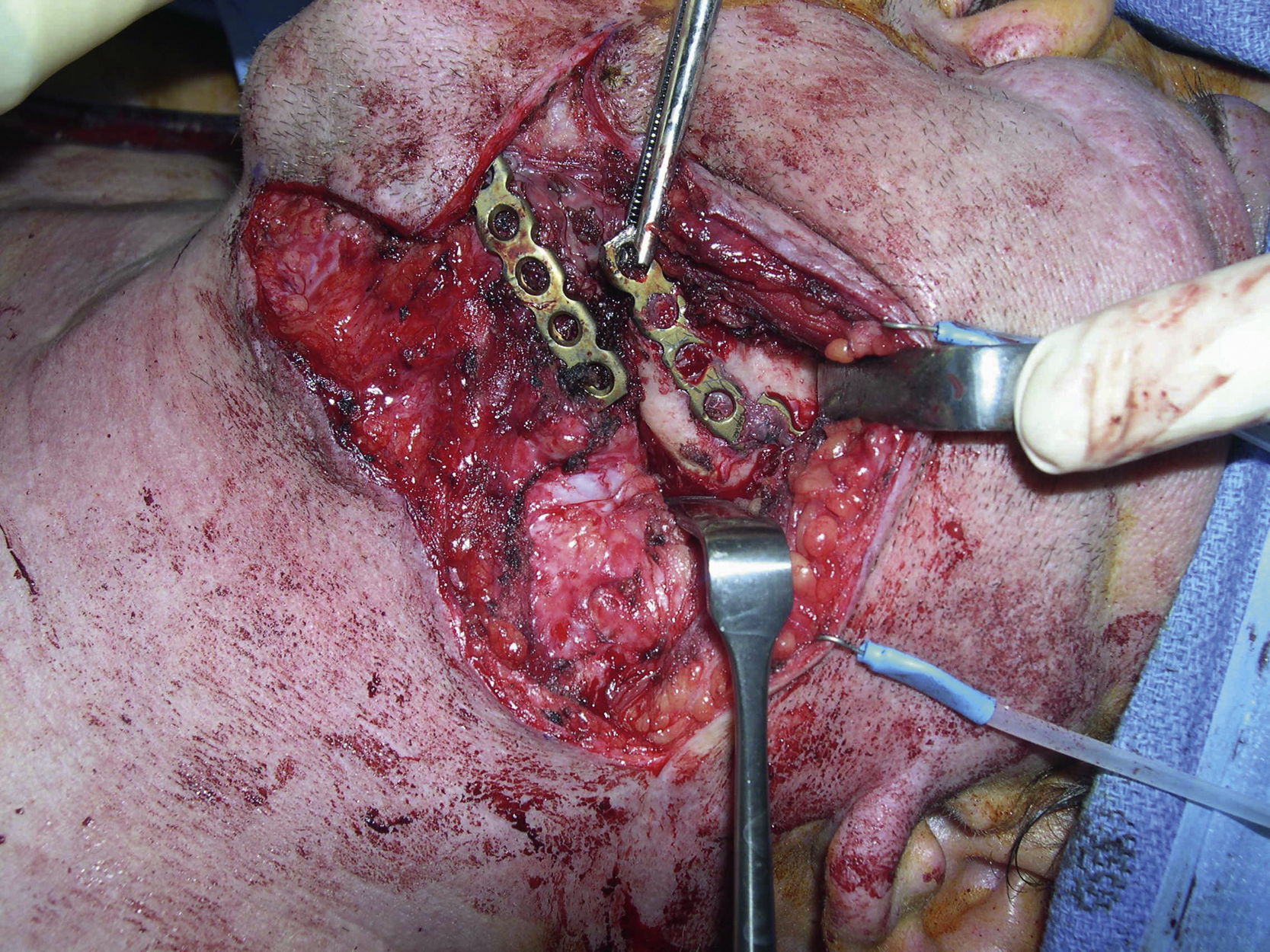
The procedure was started by two teams simultaneously. His old mandibular fracture site was explored. All scarred soft tissue was removed and both mandibular fracture sites were dissected free ( Fig. 5.4 ). Measurement of the left mandibular bony defect confirmed it to be 10 cm long. The previous submandibular incisions were reopened for a wide exposure.
The right facial artery and vein were explored and both recipient vessels appeared to be a good size.
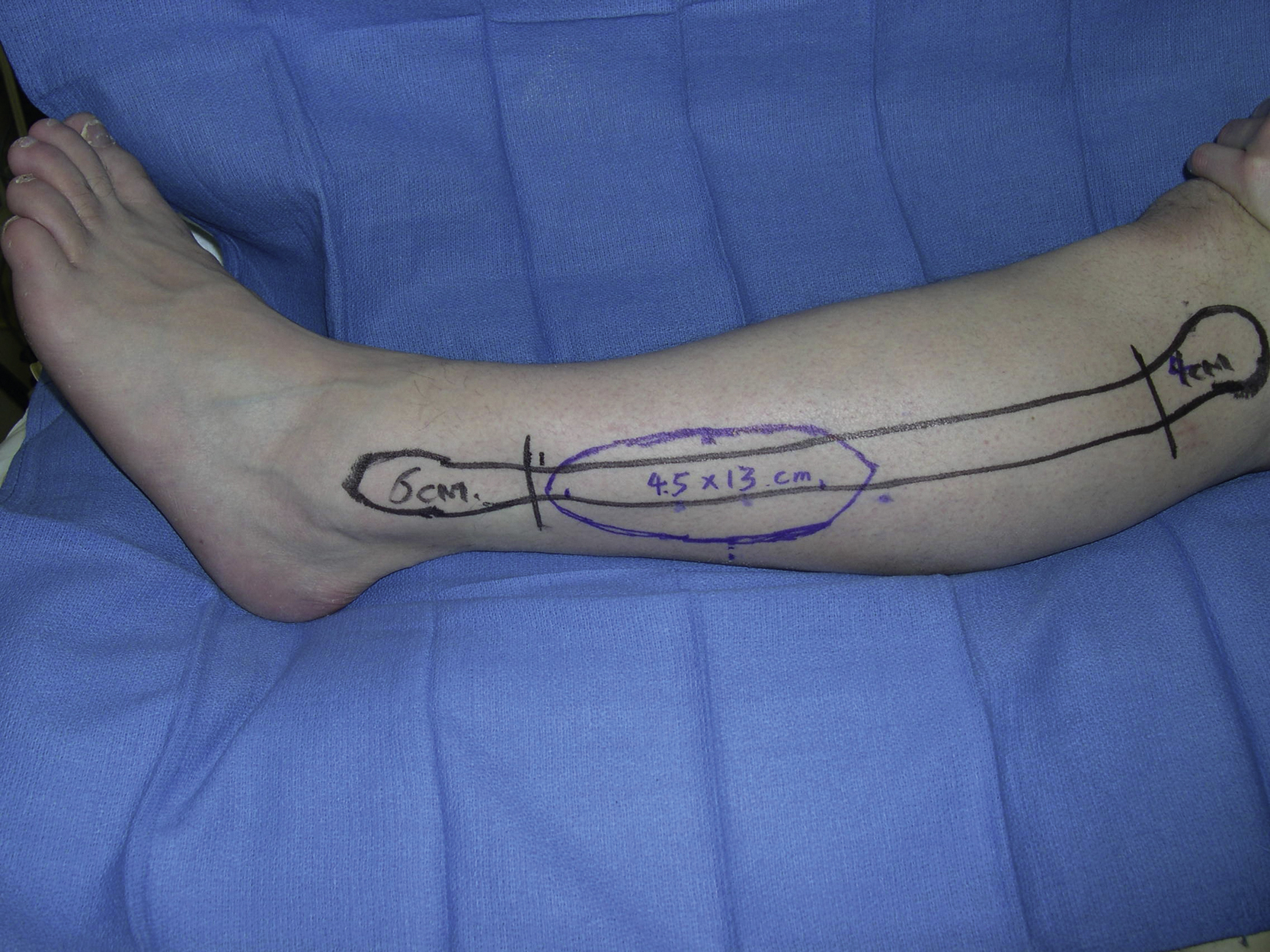
The left free fibula osteocutaneous flap was harvested and a 13 × 4.5 cm skin paddle was created ( Fig. 5.5 ). Under tourniquet control, the skin paddle was incised to the fascia. The subfascial dissection was performed toward the posterior intermuscular septum. Two septocutaneous perforators were identified within the septum and . Attention was given to avoid direct or indirect injury to them. The dissection was done to release the muscle attachment to the fibula from the soleus muscle. Once the peroneal vessels close to the fibula were identified, the distal osteotomy was performed at a level of about 6 cm proximal to the lateral malleolus. By further dissection of the hallucis longus muscle’s attachment, the peroneal vessels and the fibula were dissected free. The proximal osteotomy was then performed and a 10-cm segment of the fibula was obtained. A longitudinal skin incision was extended toward the fibular head. After more dissection around the pedicle, the peroneal vessels were dissected free toward its bifurcation. Once the bifurcation was visible, the pedicle was divided and the flap’s dissection was completed. With the guide of the dental model, only one osteotomy was performed on the nonperiosteum attachment side ( Fig. 5.6 ).