Case 1
Clinical Presentation
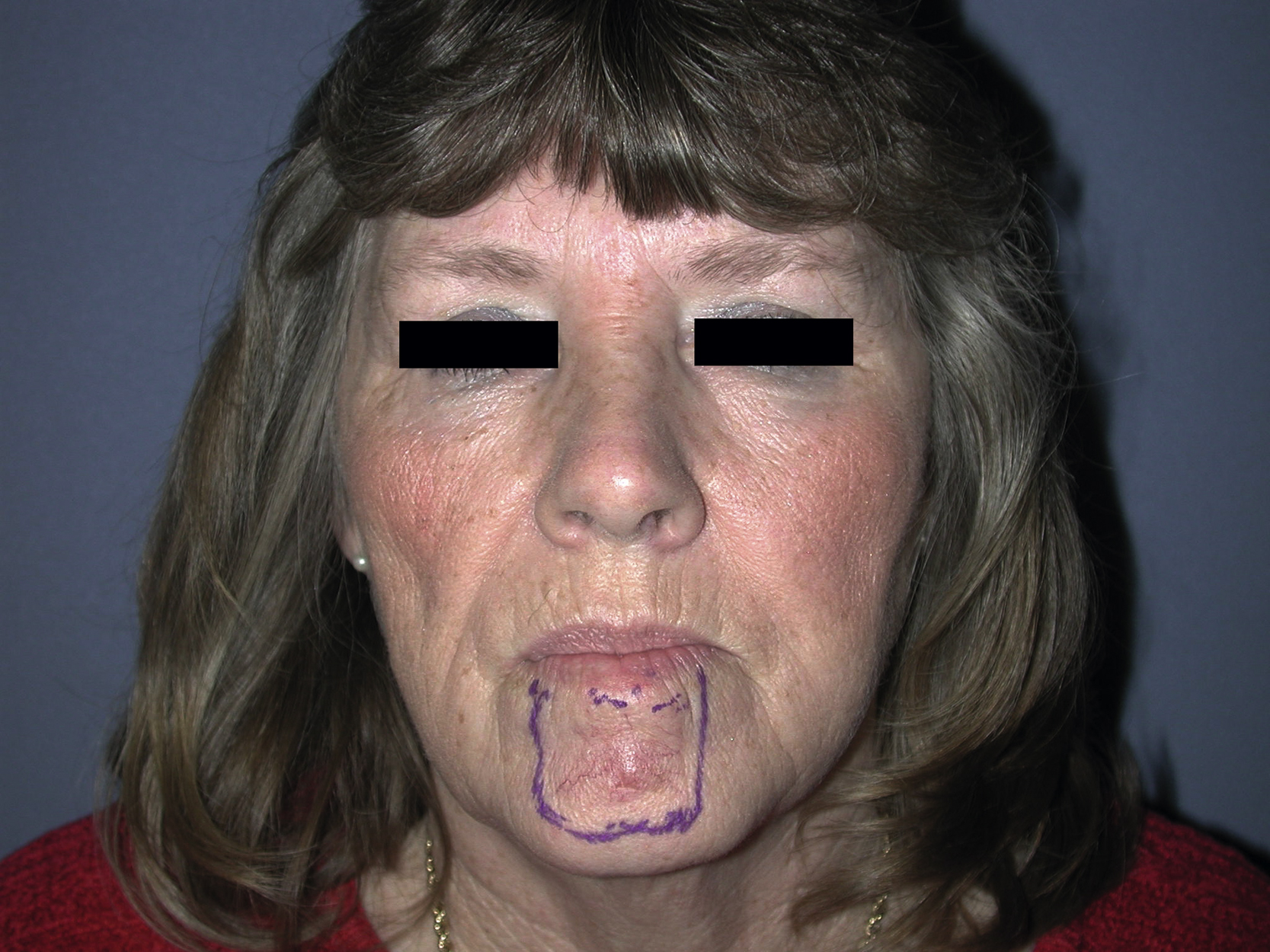
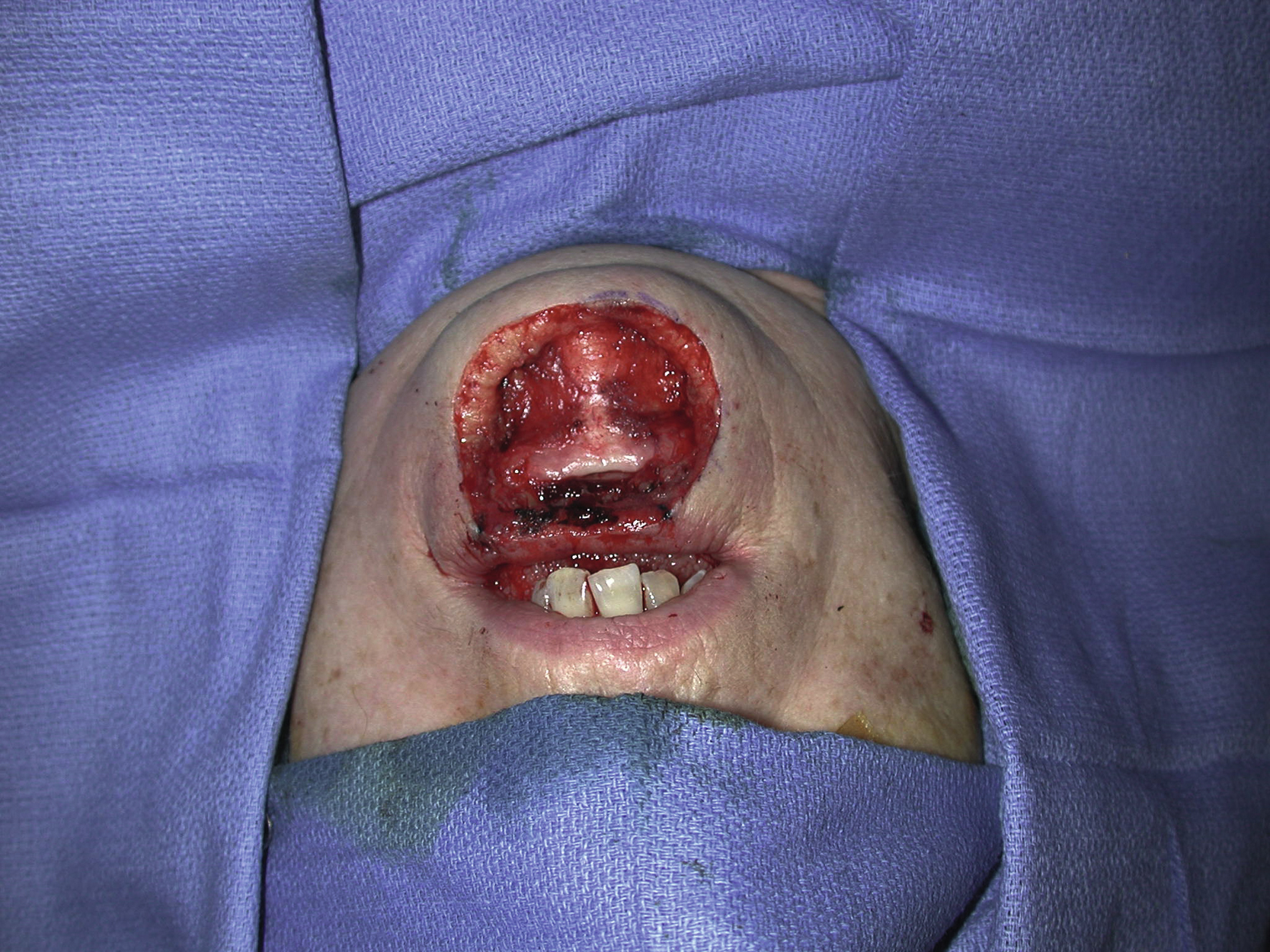
A 58-year-old White female had a 4 × 4 cm skin lesion of cancerous appearance above her central lower lip ( Fig. 9.1 ). She underwent a local excision of the lower lip lesion with a 5-mm margin by the plastic surgery service ( Fig. 9.2 ). All peripheral and deep margins were confirmed negative for basal cell carcinoma, a tissue diagnosis in the operating room, by intraoperative frozen sections. The defect over her central lower lip extended to the muscle but in the most area it was a full-thickness through-and-through defect ( Fig. 9.3 ). A definitive lower lip reconstruction was planned for this patient by the same service.

Operative Plan and Special Considerations
Based on the location and size of the lower lip defect, which was about two-thirds of the entire lower lip, bilateral Karapandzic flaps were planned for this patient. The flap, performed bilaterally, would be ideal for the reconstruction of a large central lower lip defect. In this case, the excess lower face and cheek skin could be incorporated with each flap to facilitate both flaps’ approximation in the midline so that the defect could be closed primarily without much tension.
Operative Procedures
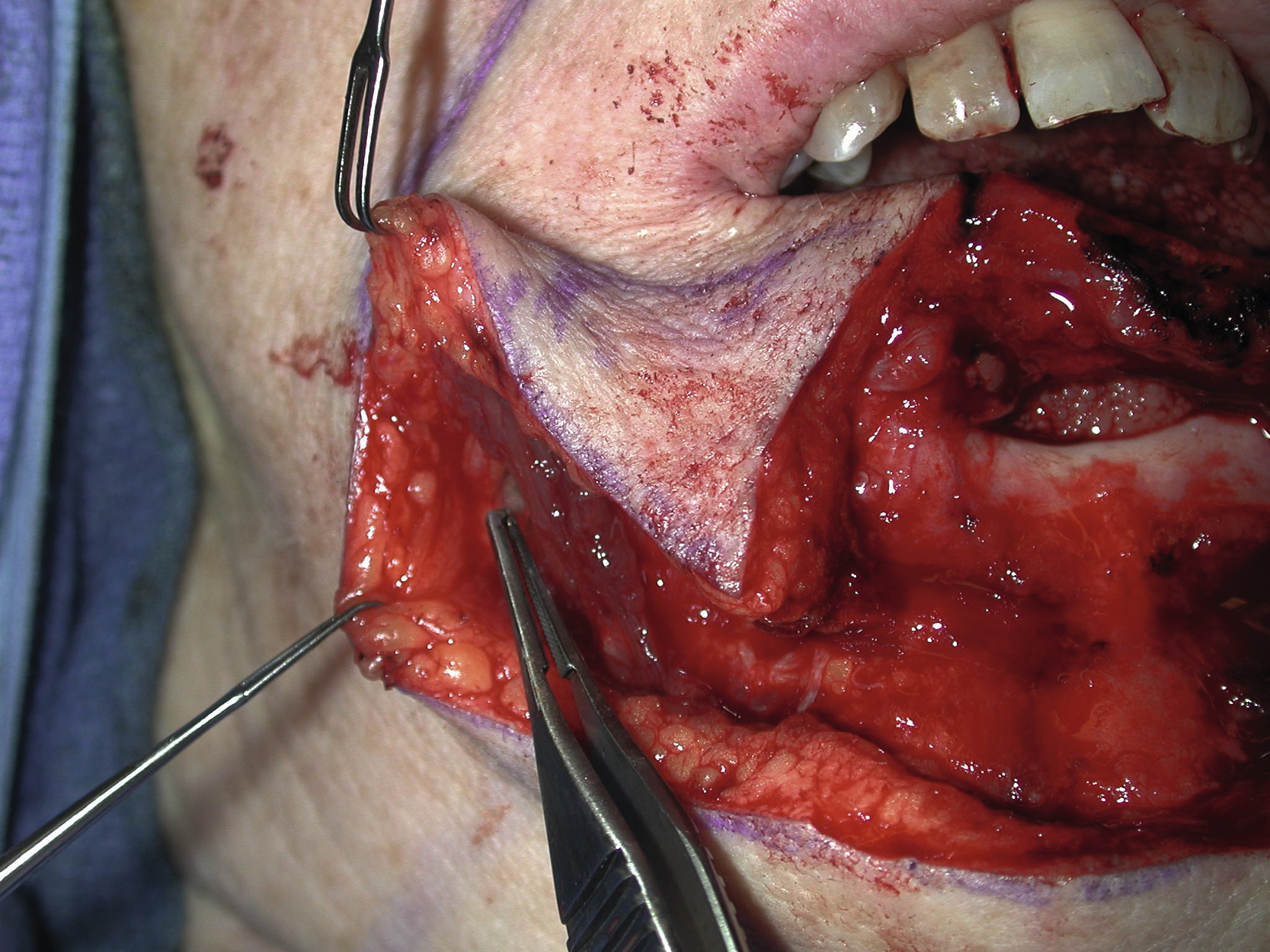
Bilateral Karapandzic flaps were designed based on the existing skin crease in each side of the lower face and extended to the nasolabial fold ( Fig. 9.4 ). All proposed skin incisions and dissection areas were infiltrated with 1% lidocaine with 1:100,000 epinephrine. The connected portion of the lower lip was excised, to facilitate the approximation of bilateral Karapandzic flap closure to the midline. Once the transverse skin incision had been made through the subcutaneous tissue to the orbicularis oris muscle, the muscle fibers were spread apart longitudinally to aid the flap’s rotation and advancement to the midline. Care was taken to preserve the neurovascular pedicle of the flap on each side ( Fig. 9.5 ). The skin incision was extended to the nasolabial fold and with additional muscle fiber spreading, both flaps could be approximated in the midline without tension. The midline closure was done in four layers from the mucosa, muscle, and subcutaneous tissue to the skin. The rest of the flap closure was done in two layers from the subcutaneous tissue to the skin. The back cut was extended to each side of the cheek to facilitate the flap’s rotation and advancement. All skin closure was performed with 5-0 nylon suture in either interrupted or running fashion. The actual closure of the mucosa in the lower lip was done with 5-0 chromic sutures in an interrupted fashion ( Fig. 9.6 ).

Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


