Case 1
Clinical Presentation
A 40-year-old White male had a very complicated injury to his right hip and lateral thigh regions with a pelvic fracture and extensive muscle necrosis over his right hip region as a result of a motor vehicle accident. He unfortunately developed heterotopic ossification requiring resection of the head of the right femur. A definitive treatment plan, proposed by the orthopedic trauma service, was to perform right total hip replacement as soon as possible after additional bony debridement. However, because of lack of good soft tissue and the poor skin quality secondary to the heterotopic ossification and the frequent surgeries in the area ( Fig. 40.1 ), the primary service felt that it would be critical to obtain better soft tissue coverage to the area immediately after the total hip replacement. The plastic surgery service was consulted to provide reliable soft tissue coverage for the potential right hip prosthesis. Because there was no reliable local option available, a free tissue transfer would be required for this kind of soft tissue coverage. However, the lack of recipient vessels for free tissue transfer presented a real challenge because all potential recipient arteries were occluded during initial embolization to control bleeding.
Operative Plan and Special Considerations
Because there was no reliable local option after total hip replacement, a free latissimus dorsi muscle flap could be selected to provide a good and reliable soft tissue coverage for potentially exposed hip prosthesis. The flap has a long pedicle and can provide large but well-vascularized soft tissue to obliterate the deep space for reliable soft tissue coverage. Because of the previous arterial embolization to the pelvic vessels to control bleeding, no suitable recipient vessel could be identified on preoperative angiogram to be used for free tissue transfer. The descending branch of the lateral circumflex femoral vessels in the thigh is well known because of increased experience by surgeons in harvesting an anterolateral thigh perforator flap. After a straightforward dissection between the rectus femoris and vastus lateralis muscles, the descending branch of the lateral circumflex femoral vessels in the thigh, when dissected with adequate length, can be placed in the lateral thigh to serve as an excellent recipient vessel for free tissue transfer to the thigh or hip.
Operative Procedures
Under general anesthesia, the patient was placed in the left lateral decubitus position. Prior to the procedure, the descending branch of the lateral circumflex femoral vessels was identified by duplex scan and marked ( Fig. 40.2 ).

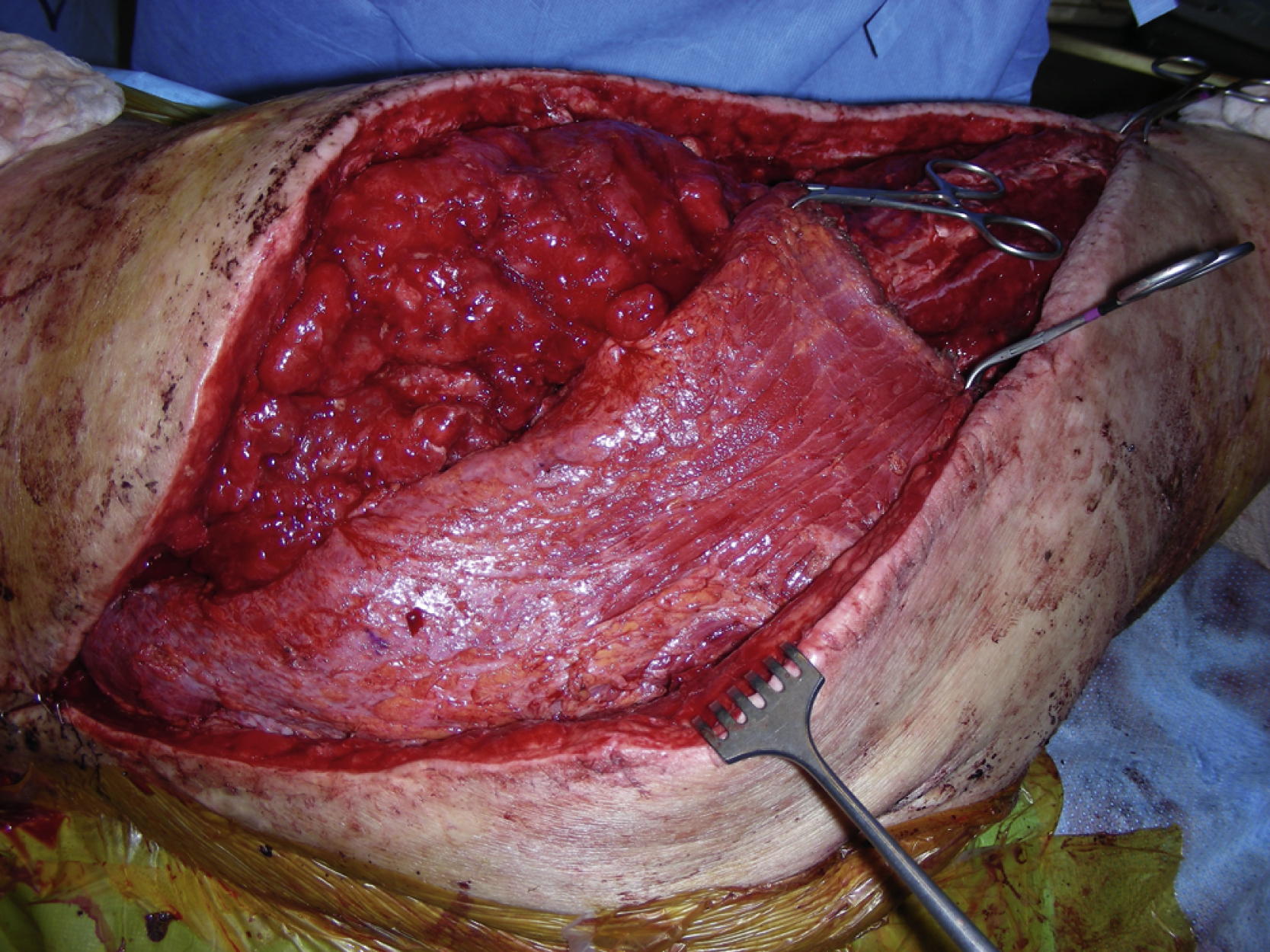
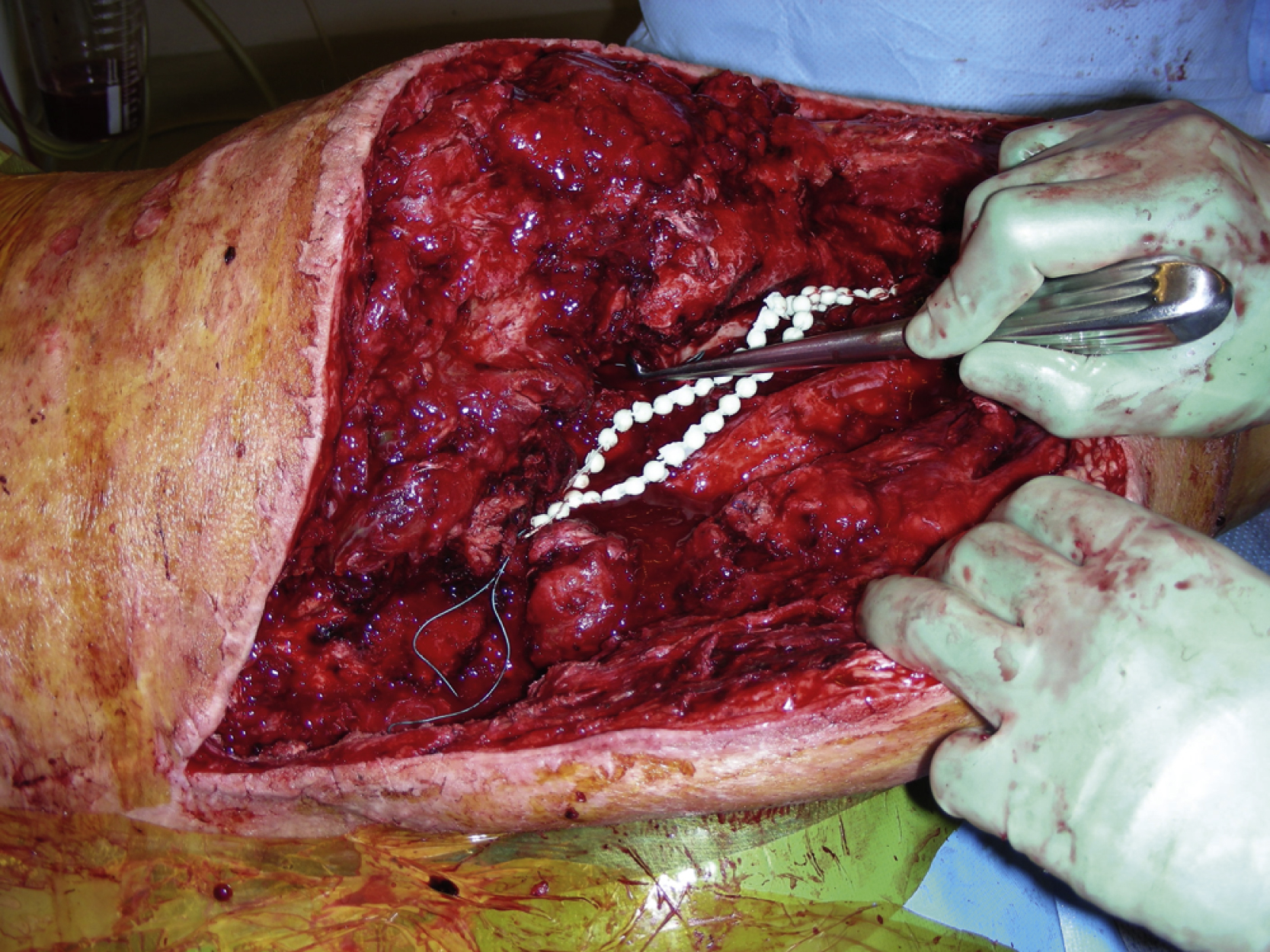
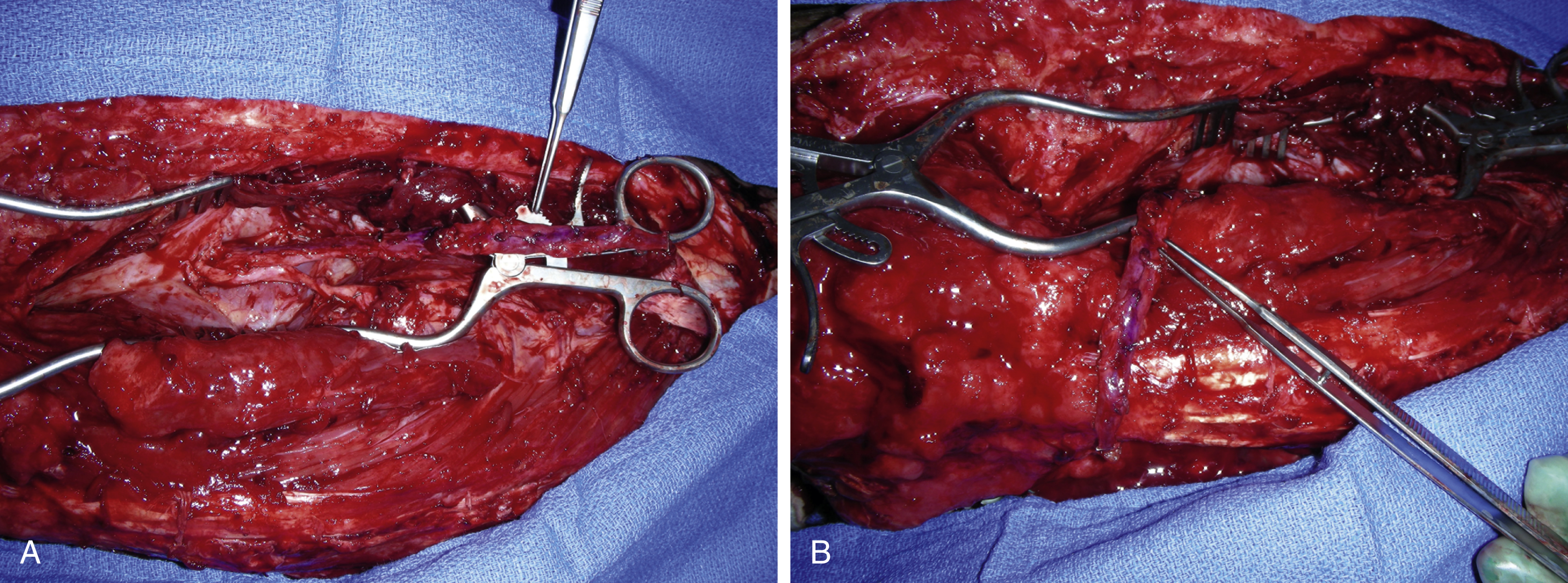
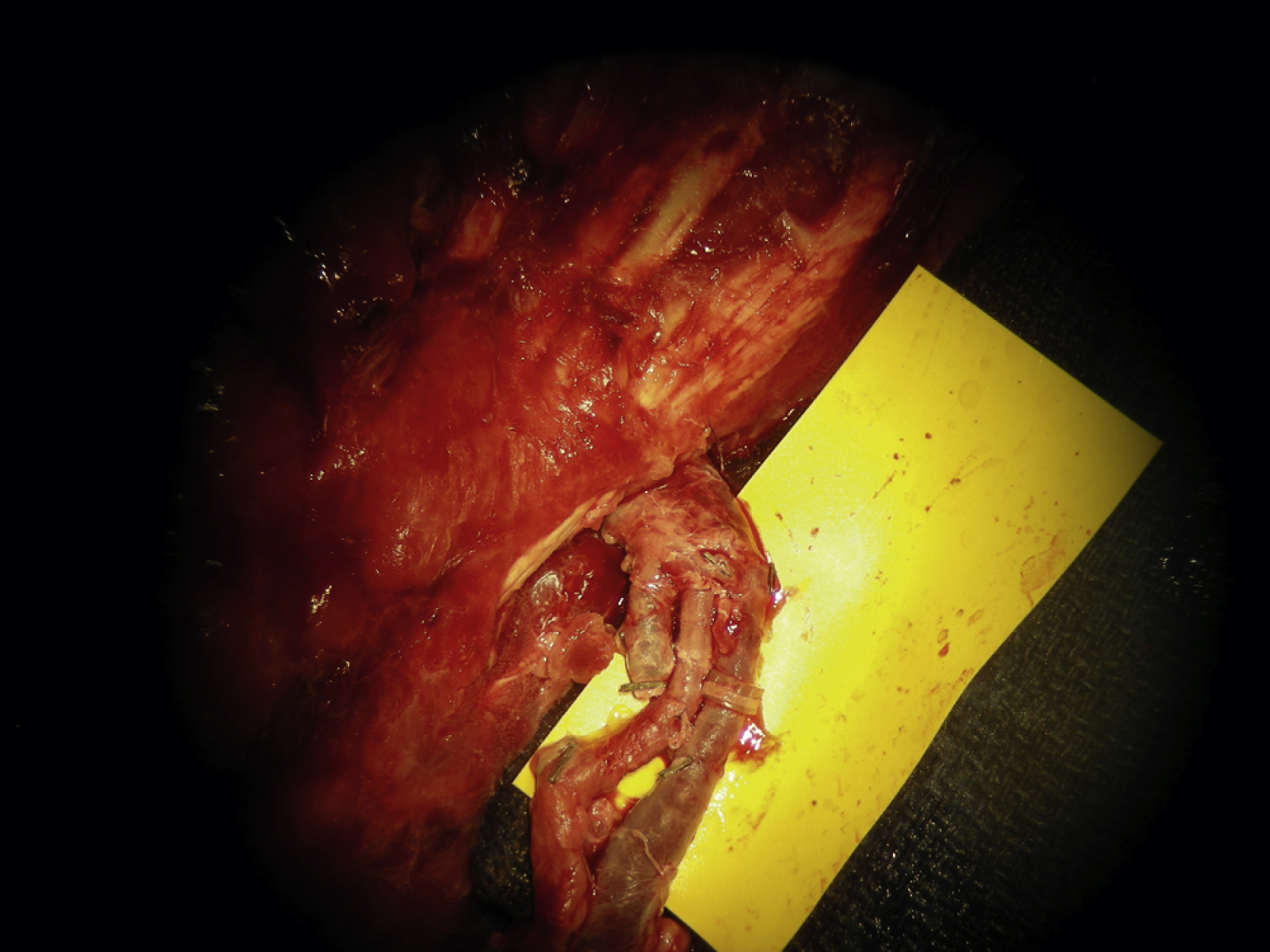
The previous right hip incision was reopened. There was a fair amount of blood clots as well as seroma. All were removed and the open wound was then irrigated. The entire potential wound measured 30 × 11 cm. Based on the duplex finding, the right lateral thigh incision was extended more medially and inferiorly and the space between the rectus femoris and the vastus lateralis was opened. The descending branch of the lateral circumflex vessels was identified and the vessel was divided with hemoclips at the most distal level near the knee. Retrograde dissection was then performed along the entire length and the many small branches from it were divided with microclips ( Fig. 40.3A ). The motor nerve was spared during dissection. The dissection again followed a retrograde fashion in the space between the rectus femoris and vastus lateralis toward the profunda. At least 12 cm of the pedicle was dissected free ( Fig. 40.3B ) and then tunneled under the vastus lateralis and brought out superficially to serve as extended recipient vessels with a good arterial flow ( Fig. 40.4 ). Care was taken to ensure that the entire pedicle was not kinked or compressed.

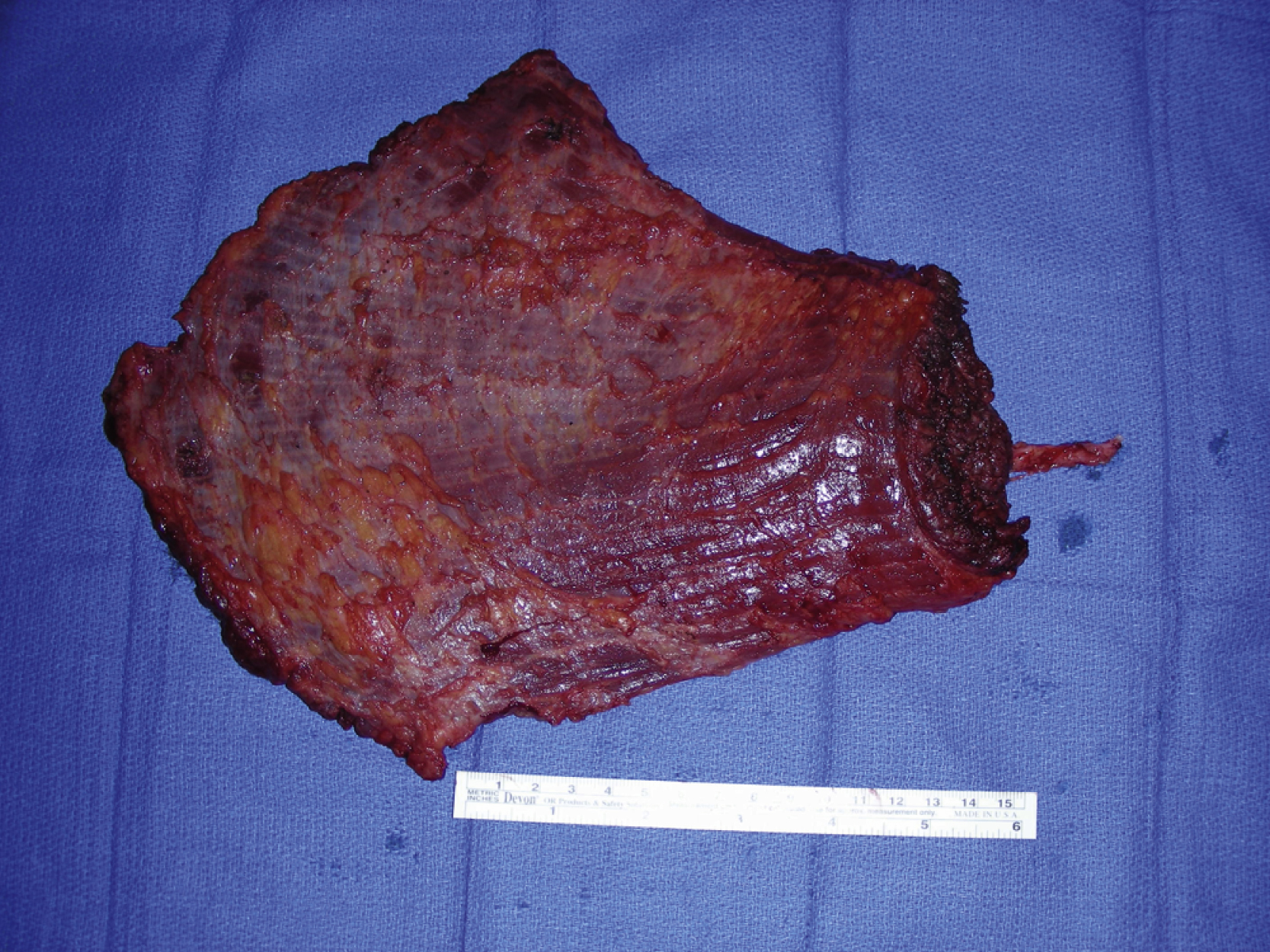
The right latissimus dorsi muscle was harvested next. An oblique incision was made down to the latissimus dorsi muscle fascia. Once both medial and lateral borders of the latissimus muscle were identified, the muscle was divided with electrocautery medially, inferiorly, and laterally. Under direct vision, the latissimus dorsi muscle was elevated from the chest wall, but the serratus muscle was left intact. After division of the serratus branch of the artery, the latissimus dorsi muscle attachment to the humerus was divided with electrocautery. The pedicle dissection was performed under direct vision with proper retraction. The thoracodorsal nerve was divided first and both thoracodorsal artery and vein were then divided after further pedicle dissection ( Fig. 40.5 ).
The muscle flap was prepared on a separate table. The pedicle artery and vein were irrigated with heparinized saline solution. The muscle flap was temporarily placed into the right hip wound. Under a microscope, an end-to-end arterial microanastomosis was performed with an interrupted 8-0 nylon suture. A 3.0-mm coupler device was used for an end-to-end venous microanastomosis ( Fig. 40.6 ). After all the clamps had been removed, the flap was instantly perfused with good Doppler signals throughout. The flap was placed over the hip region for 1 hour and it appeared to be stable with good arterial and venous flow ( Fig. 40.7 ).
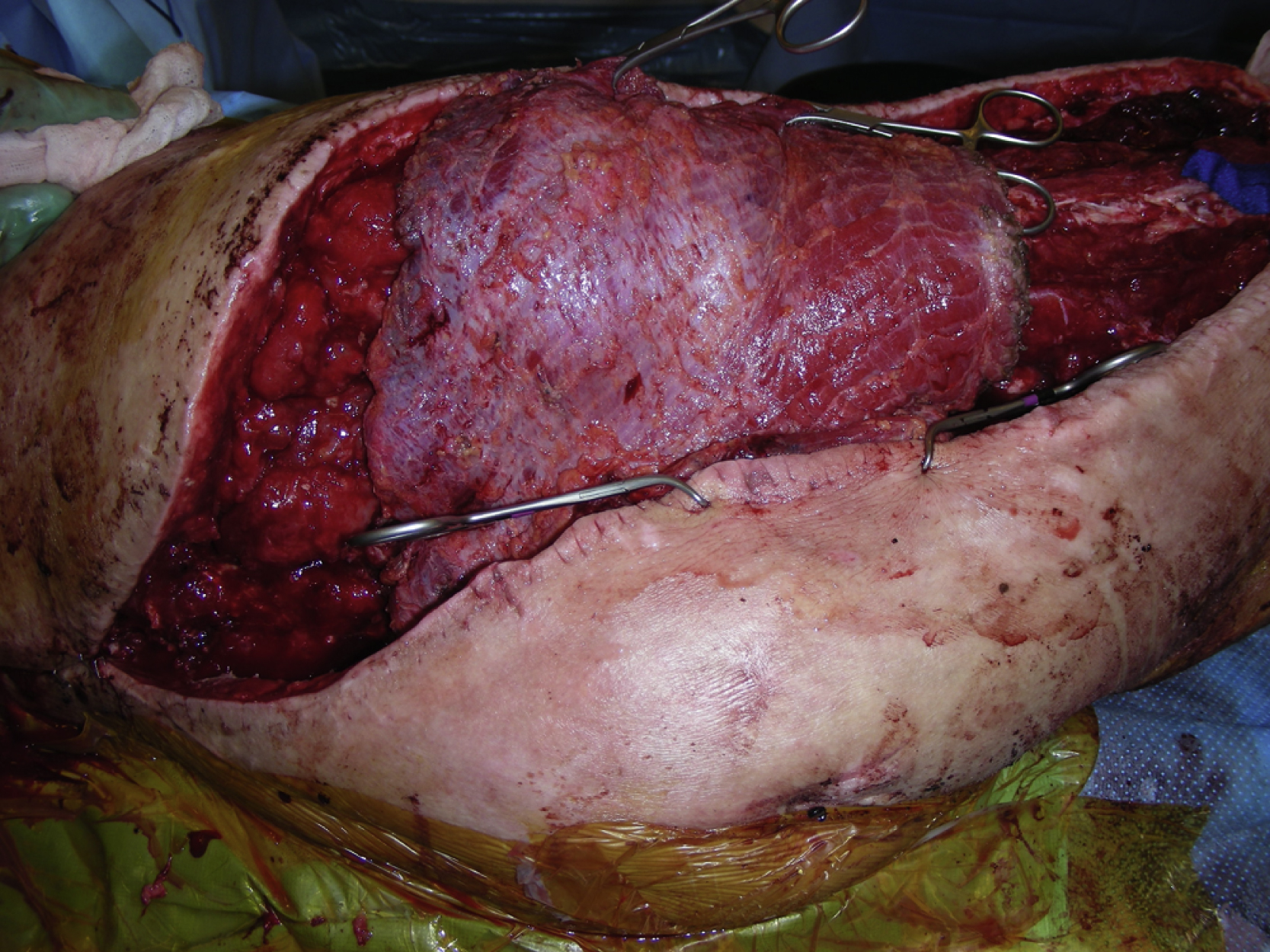
At this point, the orthopedic trauma service performed the right total hip replacement with prosthesis while the flap was temporarily placed near the area. The right total hip replacement was completed by the primary service. Because of the skin condition and the amount of swelling, it was initially impossible to close the right hip wound. Therefore, the intraoperative decision was made to place the muscle flap to cover the entire prosthesis and the hip wound ( Fig. 40.8 ). The muscle flap was inserted into the entire wound with 2-0 PDS sutures in a figure-of-eight. The most proximal part of the hip wound and the distal part of the thigh wound were approximated temporarily with towel clips. The skin edge was sutured to the surface of the muscle flap ( Fig. 40.9 ). The split-thickness skin graft was harvested from the right lateral thigh. The skin graft was meshed to 1:1.5 ratio and placed over almost the entire muscle flap and secured with skin staples. The muscle flap appeared to be well perfused and viable at the end of the procedure ( Fig. 40.10 ). The rest of the skin incision was closed in two layers. The deep dermal layer was approximated with several interrupted 2-0 PDS sutures. The skin was closed with either skin staples or 3-0 nylon in a mattress fashion. A large vacuum-assisted closure sponge dressing was placed over the skin graft site and connected with a machine.