Abstract
- 1.
Transconjunctival blepharoplasty (TCB) is now a mainstream part of aesthetic eyelid rejuvenation.
- 2.
It is a more complex and intricate procedure than its transcutaneous counterpart.
- 3.
Surgery is performed from inside the eyelid and with limited exposure, so a detailed knowledge of eyelid anatomy and surgery is critical to success.
- 4.
Surgery can be performed in a preseptal or postseptal plane.
- 5.
Fat can be excised in a graded fashion or repositioned to adjacent periorbital depressions.
- 6.
Take care with standalone fast excision so as to avoid postoperative volume depletion.
- 7.
Fat repositioning allows recreation of the smooth and youthful transition of the lower eyelid to the cheek.
- 8.
Fat can be repositioned into a supra- or subperiosteal plane with similar aesthetic outcomes.
- 9.
When transposing fat pedicles special care and attention must be given to avoiding injury to the inferior oblique muscle.
- 10.
Skin excess, lax orbicularis muscle, and true eyelid laxity can be addressed with the addition of surgical adjuncts.
Keywords
Blepharoplasty, Lower blepharoplasty, Transconjunctival blepharoplasty, Fat repositioning, Lower eyelid retraction
Introduction
Lower blepharoplasty has evolved significantly since its early descriptions . Traditional surgery involved an open transcutaneous approach that allowed the excision of skin, muscle, and fat sequentially through the same subciliary incision . Although still a common approach to lower blepharoplasty today, the transcutaneous route can be associated with an increased incidence of lower eyelid malposition and rounding of the canthal angle . The addition of various canthal suspension techniques has reduced the development of these complications , but they can still occur at an unacceptably high rate . It has long been thought that unaddressed eyelid laxity, a “middle lamellar (orbital septal) scar,” and anterior lamellar shortage associated with the transcutaneous approach predisposed to these complications . More recently it has been shown that orbicularis weakness and negative vector eyelid configuration may be even more significant in the development of these issues . Whatever the primary instigators of these problems may be, the one common variable is the propensity for occurrence after open transcutaneous approach surgery . A recent report evaluating the physical findings present on patients with post-blepharoplasty lower eyelid retraction (PBLER) showed that all patients (100%) presenting with this problem had primary transcutaneous surgery . For this reason the transconjunctival approach to cosmetic lower eyelid rejuvenation has become a standard alternative for the aesthetic eyelid surgeon.
Transconjunctival blepharoplasty (TCB) has its origins in the French literature in the 1920s . It is a more complex technique than traditional open approach surgery, with limited surgical exposure, and it does not directly address lower lid skin excess. The procedure generally fell into disfavor for 50 years until 1973, when Tessier reported on its use for various reconstructive and cosmetic applications. Soon after, with the desire of reducing the incidence of lower eyelid retraction and ectropion after standard transcutaneous surgery, TCB was elaborated on by a number of authors. First, Tomlinson and Hovey described the preseptal transconjunctival approach, and then Baylis et al. the postseptal technique. The difference between these conjunctival routes of dissection was that the preseptal plane mandated septal division to access fat, whereas the postseptal route preserved this delicate tissue structure. It was thought that septal preservation was integral to preventing lower lid malposition after surgery . It has now been shown that when approaching fat transconjunctivally, septal manipulation does not play a role in postoperative eyelid malposition . Although septal scarring most assuredly is involved in PBLER, it is the combined skin/muscle/septal incision that predisposes to this complication and not an isolated septal manipulation (as is seen in preseptal TCB) .
Until the latter part of the 20th century lower blepharoplasty was primarily a fat-subtractive procedure . Postoperative volume depletion with a hollow, gaunt, and skeletonized appearance was not uncommon. With the more contemporary understanding that volume loss is a critical component of facial/eyelid aging , surgeons have come to understand that excisional-based surgery can be a form of iatrogenic aging rather than a recreation of youth . Today aesthetic lower blepharoplasty focuses on volume preservation and augmentation to maintain the fullness, curves, and contours of the youthful face and eyelids . In addition it is now clear that successful blepharoplasty involves more than surgery on the lower eyelid alone, but rather on the eyelid and its transition to the midface, as these two structures are considered one aesthetic unit . These observations fueled the development of fat transposition lower blepharoplasty variations, in which native eyelid/orbital fat is redistributed from areas of relative excess “lower eyelid bags,” to areas of relative deficit “underlying depressions,” with the goal of reducing lid prominence, effacing adjacent hollows, and smoothing the transition of the lower lid to the cheek.
Lower blepharoplasty with fat repositioning (LBFR) was first described by Loeb in 1981 , and has been elaborated on by many since . It can be performed through a transcutaneous or transconjunctival approach , and the fashioned fat pedicles can be placed in either the sub- or supraperiosteal planes . Although the techniques of sub- versus supraperiosteal fat transposition differ, a recent study showed that there is no difference in final aesthetic outcome between the two approaches . In this chapter the authors detail and outline the critical aspects of transconjunctival lower blepharoplasty with and without fat repositioning. An overview of lower eyelid anatomy and aging changes will be also be outlined.
Relevant Anatomy
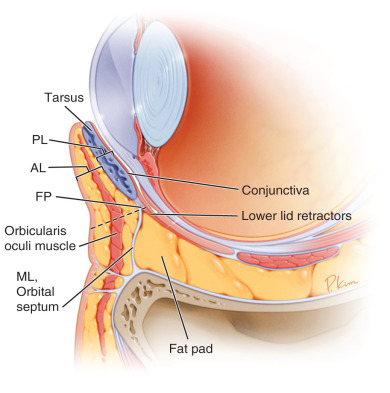
The lower lid is a complex structure composed of an anterior and posterior lamella ( Fig. 12.1 ). The anterior lamella, which is composed of skin and orbicularis oculi muscle, is consistent the full height of the eyelid from the eyelid margin to the orbital rim. The composition of the posterior lamella changes depending on its location within the eyelid. Just below the lashes the posterior lamella includes the tarsus and fused conjunctiva. Five millimeters below the lashes (at the base of the tarsus) the tarsus is replaced by a confluence of the orbital septum and lower lid retractors. This also continues for approximately 5 mm. Below this point (fusion point of lower lid retractors and orbital septum) the posterior lamella consists of lower lid retractors and conjunctiva. The orbital septum continues as the middle lamella until its origin at the orbital rim. There are three fat pads in the lower lid: nasal (medial), central, and lateral. These fat pads are sandwiched between the orbital septum and lower lid retractors. In the horizontal plane, the inferior oblique muscle lies between the nasal and central pad, and the arcuate ligament (an extension of Lockwoods’s ligament) separates the central and lateral fat pad ( Fig. 12.2 ).
At the orbital rim the orbital septum fuses with the periosteum of the orbit and face of the maxilla. This dense fusion point is called the arcus marginalis. Below this point the eyelid transitions to the midface. The midface consists (anterior to posterior) of the skin, malar fat pad, muscle layer (orbicularis oculi throughout and the zygomaticus muscles laterally and the levator labii and its adjacent alaeque nasi medially), suborbicularis oculi fat (SOOF) pad, and periosteum. The orbitomalar ligament (OML) is an anterior-posterior osseocutaneous connective tissue structure originating from just below the orbital rim and inserting onto the orbicularis muscle and dermis of the upper midface. The OML underlies the location of the periorbital hollows, which are filled with lower blepharoplasty fat-repostioning surgery ( Fig. 12.3 ).
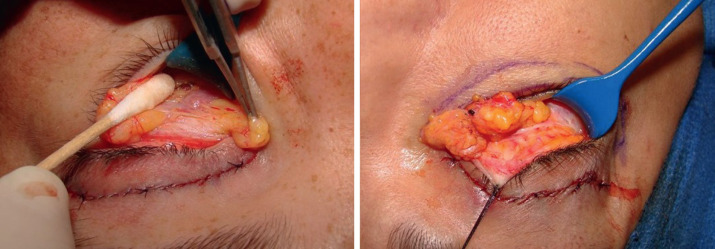
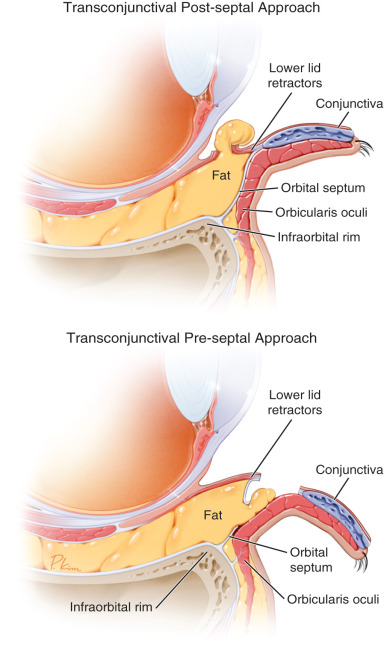
There are some critical anatomic features relevant to transconjunctival surgery. First, transconjunctival entry can be at the base of the tarsus through the fused conjunctiva/retractor/septum layer. In this plane dissection proceeds preseptally, posterior to the orbicularis muscle and anterior to the septum. Alternatively, entry can be more than 5 mm below the base of the tarsus, through the conjunctiva and retractors only ( Fig. 12.4 ) to access orbital fat post(retro)septally. The authors prefer the latter (postseptal) dissection, although both approaches lead to excellent results with infrequent complications. Second, as mentioned, the inferior oblique muscle separates the nasal and central fat pads. In cases of fat-transposition surgery, these are the fat pads that are fashioned into pedicles for translocation. It is important to assure that there are no attachments of the fat pedicles to the oblique muscle before fat transposition, to prevent potential postoperative ocular motility issues. This is achieved by lysing any obvious connective tissue bands from the muscle. The authors employ a maneuver that assures this step, which they have called the “inverse shoe shine sign” (refer to surgical section later) ( Fig. 12.5 ) . Third, by definition, the arcus marginalis is released when fat is transposed subperiosteally (arcus marginalis release is needed to create a subperiosteal pocket). Conversely, when supraperiosteal surgery is performed, the periosteum and arcus are left attached, but the OML is released. Some believe that release of the OML improves lid/cheek interface depression effacement better than when the OML is left intact . This has yet to be studied in an evidence-based manner. In either instance, fat is placed where the age-related depressions (eyelid/cheek junction) are present.
Lower Eyelid Aging Changes
Patients presenting with “eyelid bags” typically have age-related structural alterations to the eyelid and its adjacent middle face. Lower eyelid/midface aging is a multifactorial process involving degenerative changes in the skin and muscle, loss of soft tissue volume, bone remodeling, and tissue descent . The aged lower eyelid/midface demonstrates true or relative fat herniation, septal attenuation, volume loss over the infraorbital rim, and midface descent/deflation ( Fig. 12.6 ) .These changes convert the topography of the eyelid/cheek transition from the concavity/convexity of youth to the double convexity of age . In between these convexities are depressions or periorbital hollows, which require surgical effacement to attain appropriate cosmetic surgical outcomes (see Fig. 12.3 ). Traditional fat-excision lower blepharoplasty often leads to postoperative volume depletion (eyelid hollows) and exacerbation of the unmasked orbital rim (periorbital hollows) . Fat repositioning is added to lower blepharoplasty to camouflage these adjacent eyelid/cheek interface depressions . The technique allows preservation of eyelid volume, filling of periorbital hollows, and recreation of the youthful transition of the lower lid to the midface .

Indications
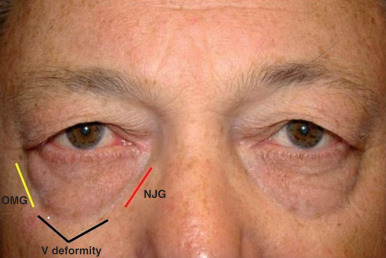
LBFR is indicated in patients demonstrating lower lid fat prominence with adjacent periorbital hollows. In the lower lid/midface transition these hollows have been named according to their anatomic location. The nasojugal groove (tear trough) is most nasal, the V-deformity central, and the orbito (palpebro) malar groove most lateral (see Fig. 12.3 ) . Typically the nasal and central lower lid fat pads are transposed to the tear trough and central lid hollow. There are two critical factors that must be present for effective performance of the procedure: (1) adequate fat to transpose; and (2) a noticeable depression to efface. In cases when primarily fat protrusion is present without an associated depression, standalone subtractive lower blepharoplasty is adequate. When the primary deficit is an eyelid/cheek depression without appropriate fat to reposition, fat grafting or soft tissue fillers are better options. LBFR, in itself, does not address skin excess, reduced orbicularis tone, or eyelid laxity. However, when indications are present, skin excision, muscle placation, and canthal suspension can be added to enhance surgical results.
Surgical Technique
All procedures are performed under conscious sedation or general anesthesia depending on patient preference and associated procedures. If fat transposition is planned, the tear trough (nasojugal fold) and central lid depression are marked in the preoperative area, with the patient in the sitting position, for reference during surgery ( Fig. 12.7 ). It is often helpful to have the patient look up when assessing the fat pads. This maneuver tends to better delineate the degree of relative fat prominence, and allows a visualized separation of the central from lateral fat pad, as in upgaze this delineation by the arcuate expansion (which is anterior in the orbit) is more obvious. Conversely the nasal and central pads appear continuous as their dividing anatomic structure, the inferior oblique muscle, is more posteriorly located in the orbit and the anterior extent of the fat pads overrides the muscle ( Fig. 12.8 ) . Once the patient is prepped and draped, the eyelid is infiltrated transconjunctivally with 2 mL of lidocaine (Xylocaine) 1% with 1 : 100,000 epinephrine. If fat repositioning is planned, an injection is also given transcutaneously over the nasojugal groove to the periosteum. If a preseptal plane of dissection is preferred, an incision is made below the tarsal border but above the fusion point of the orbital septum and lower eyelid retractors. A Desmarres retractor is used to displace the eyelid inferiorly for initiating an incision 5 mm or less below the tarsus ( Fig. 12.9 ) . The dissection then proceeds in a plane between the orbicularis anteriorly and septum posteriorly until reaching the arcus marginalis at the orbital rim ( Fig. 12.10 ). In this instance the orbital septum will be in direct view and will need to be incised to enter the fat compartment. For the purposes of this chapter the authors will describe the retroseptal approach to fat, as this is their preferred approach. The steps after fat access are the same for both approaches.