Tarsal Coalition Bar Resection
Susan T. Mahan
Operative Indications
Presence of a tarsal coalition, most commonly either a talocalcaneal coalition (TC) or calcaneonavicular (CN) coalition in a child with foot or ankle pain with activity that has been recalcitrant to conservative treatments.
Talocalcaneal Coalition
Equipment: High-speed burr, retractors, small rongeurs and curettes, small and medium lamina spreaders, bone wax (in addition to preoperative computed tomography [CT] scan of the foot!)
Positioning: Supine with the foot externally rotated—put a bump under the contralateral hip if natural positioning of the leg does not leave the foot externally rotated
Surgical approach: Medial aspect of the hindfoot, coming directly down on the middle facet of the subtalar joint
Techniques in Steps ( Video)
Video)
Video)
Make an incision from the medial aspect of the navicular, over the middle facet of the subtalar joint to just before the Achilles, with slightly curving proximally to be over the retrocalcaneal fat pad in the posterior aspect of the incision
Dissect down and open the sheath of the flexor digitorum longus (FDL), extending the sheath incision under direct visualization distally and proximally (Figure 24.1)
Retract the FDL plantarly
Find and protect the neurovascular bundle—this can be done by incising the floor of the FDL and then elevating the plantar aspect of the FDL sheath and the bundle so a blunt retractor (such as an
“S”-retractor) can be placed around the FDL and the bundle to keep them safe for the remainder of the procedure (Figure 24.2)
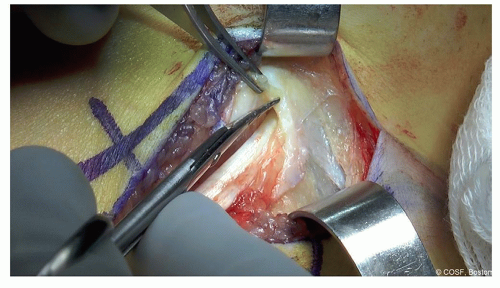
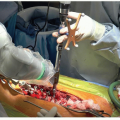
Figure 24-1 ▪ Find the flexor digitorum longus tendon, and then dissect proximally and distally in line with the tendon to facilitate exposure and retraction. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
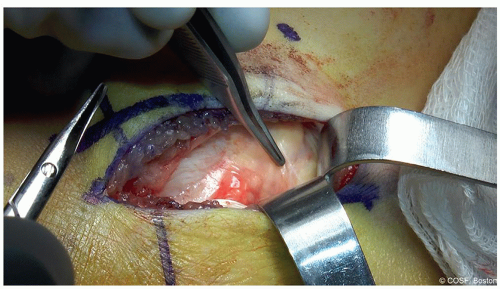
Figure 24-2 ▪ With the flexor digitorum longus retracted plantarly, identify where the neurovascular bundle is (it is pointed out in this photo) so it can be dissected and protected. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
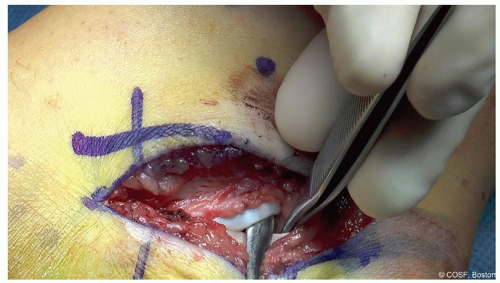
Figure 24-3 ▪ With the flexor digitorum longus and bundle now retracted plantarly, identify the flexor hallucis longus tendon which is under the calcaneal sustentaculum (at the tip of the Freer). (Courtesy of Children’s Orthopaedic Surgery Foundation.)
Identify the flexor hallucis longus (FHL) under the sustentaculum, and this can be retracted along with the bundle and the FDL for protection or left under the sustentaculum as needed (Figure 24.3)
Once the neurovascular bundle and the FHL and FDL have been identified, work to increase the exposure distally to the navicular (and anterior facet of the talocalcaneal joint) and posteriorly to the posterior facet of the talocalcaneal joint. Depending on the location of the individual patient’s coalition (as determined by preoperative CT), more or less exposure proximally or distally should be obtained (Figure 24.4)
Utilizing a small thin osteotome (such as a 4 mm osteotome), take a small sliver of bone and periosteum from the area of the middle facet in the floor of the FDL. Depending on the extent of fibrous versus bony aspect of the individual coalition, this may reveal the narrow white line of the fibrous coalition. In a patient with a solid bony coalition at this level (which can typically be determined by preoperative CT), this white fibrous line may not be encountered (Figure 24.5)
If a thin white fibrous line of the coalition is found, then while the neurovascular bundle is carefully protected, the high-speed burr can be used (with 2 hands always!) to develop a trough along the coalition, following that thin white line (Figures 24.6 and 24.7)
If no thin white line is found or expected, then first find both the anterior facet and posterior facet and work from those known facets distally and/or proximally to develop the trough that connects to the known joint. When the middle facet coalition is entirely bony, it can be challenging to find the appropriate location for the excision
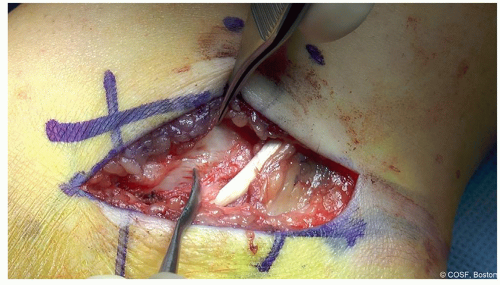
Figure 24-4 ▪ Identify the floor of the flexor digitorum longus which will be the location of the coalition (at the tip of the Freer). (Courtesy of Children’s Orthopaedic Surgery Foundation.)
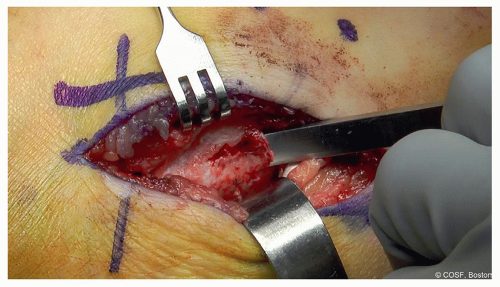
Figure 24-5 ▪ With S-retractor carefully protecting the flexor digitorum longus, flexor hallucis longus, and neurovascular bundle, take a small osteotome and peel off the top few millimeters of bone over the coalition. This will generally reveal the white line of cartilage within the bone that identifies the coalition. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
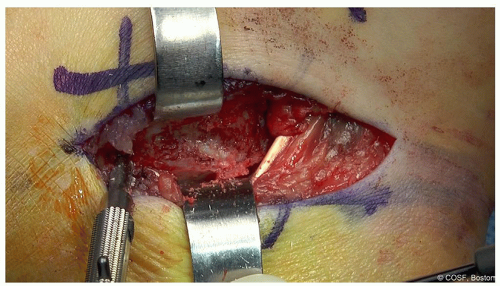
Figure 24-6 ▪ Here with the S-retractor still in place protecting the vital structures, and the Freer elevator in the posterior facet, the burr is used to follow the white line of cartilage and create a trough. Be careful to leave the sustentaculum intact. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
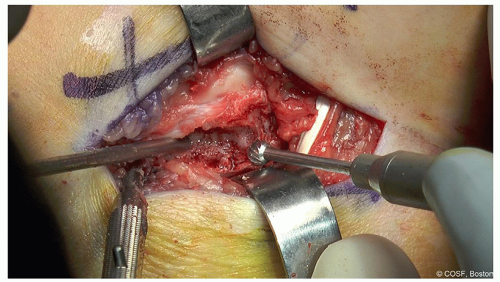
Figure 24-7 ▪ The trough is deepened using the burr. Irrigation and suction are critical. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
As the coalition is excised (using a combination of burr, curette, and rongeur), deep in the trough the normal posterior facet joint will be found (Figures 24.8 and 24.9). The lamina spreader can be used to gently open up the joint once exposed to take down any remaining spicules of bony connection. Be careful to preserve the sustentaculum and not to fracture it with the lamina spreader (Figure 24.10)
Be sure to remove all bony and fibrous connections in the coalition while leaving as much normal subtalar joint cartilage as possible (Figure 24.11). Hindfoot subtalar motion should now be seen (Figure 24.12)
Harvest some retrocalcaneal fat—about 1 to 2 cm2—while protecting the neurovascular bundle (retracting it anteriorly for this part of the procedure) (Figure 24.13)
Some surgeons utilize a separate buttock incision for harvesting fat graft instead of retrocalcaneal fat
Irrigate the coalition and incision copiously. Dry the cut bony surfaces well and apply bone wax (Figure 24.14). Place the harvested fat in the coalition (Figure 24.15). The FDL will return to the top of the excised coalition (Figure 24.16). Confirm satisfactory clinical subtalar motion
Close the skin
Place a dry sterile dressing and a bivalved short-leg cast
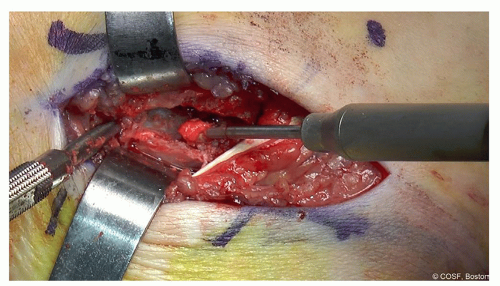 Figure 24-8 ▪ This is extended proximally and distally along the coalition until the white line becomes the joint. Here you can see some fat starting to be seen on the proximal end of the coalition. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
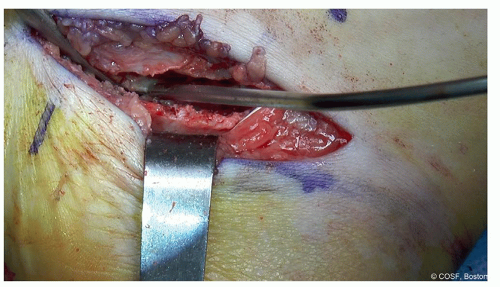 Figure 24-9 ▪ Here you can see, at the base of the trough, the black line of the joint between the 2 white lines indicating that the coalition has been resected to its base. Be sure to extend the resection proximally and distally enough. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
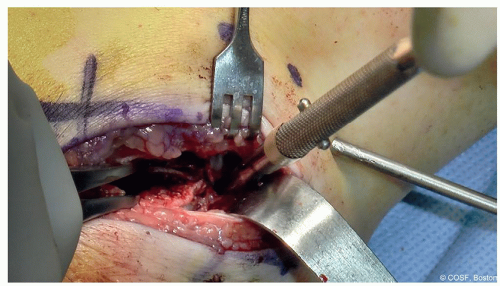 Figure 24-10 ▪ A small lamina spreader can be carefully placed in the excised coalition to determine if motion is complete and the coalition further excised; if not, then further work to release the remaining coalition needs to be done. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
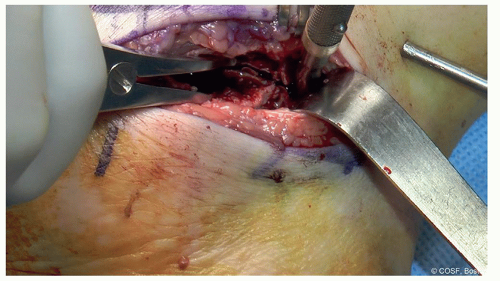 Figure 24-11 ▪ Here the Freer is in the posterior facet, and the lamina spreader is working to distract the joint so the remaining anterior coalition can be identified and excised. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|