Forearm Malunions: Corrective Osteotomies
Carley Vuillermin
Operative Indications
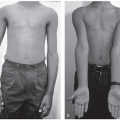
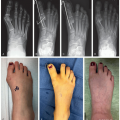
Symptomatic malunion without the potential to remodel (Figure 16.1)
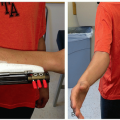
Restricted range of motion
Pain—particularly functional pain not responsive to therapy
Pain at rest should prompt investigation as it is not common in an isolated malunion
Instability
Distal radioulnar joint (DRUJ) in diaphyseal malunions
Midcarpal joint in distal radial malunions
Nerve compression
Musculotendinous contracture or impingement
Combination of the above
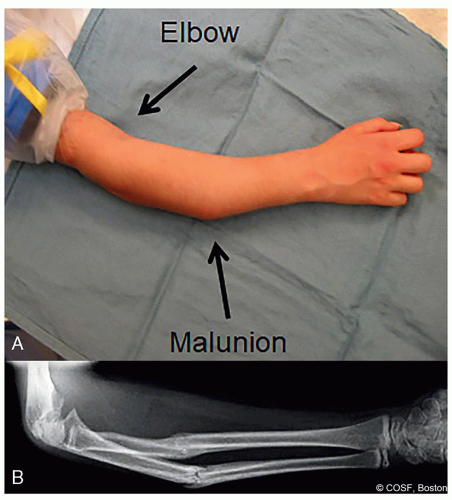 Figure 16-1 ▪ A, Photograph and (B) radiograph of marked malunion with symptomatic block to motion, dysfunction, and pain. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
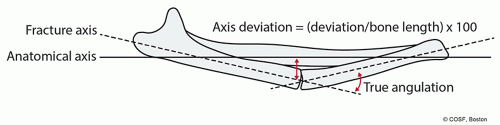 Figure 16-2 ▪ Axis deviation defines the difference between anatomic alignment (solid line) and fracture alignment (dotted lines) with true angulation. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
Alternative Treatments
Natural history
Younger children with sufficient growth remaining may remodel marked deformities
Especially if distal, close to physis, and in plane of motion of joint
Diaphyseal and especially proximal forearm malunions are less likely to remodel
Rotational malunion will not remodel (Figure 16.2)
Mild degrees of deformity may be tolerated, so correction rarely performed in the absence of symptoms, restricted motion, instability, or activity-associated pain
Corrective Osteotomy (Figure 16.3)
Equipment
Fluoroscopy
Radiolucent arm and hand table
Tourniquet
Power drill
Power saw
Osteotomes
Laminar spreaders (small and medium)
Smooth C-wires
Standard dissecting kit
AO small fragment set (or appropriate sized implant for case)
Bone graft—structural allograft, cancellous chips, or iliac crest autograft may be required
Casting materials and cast saw
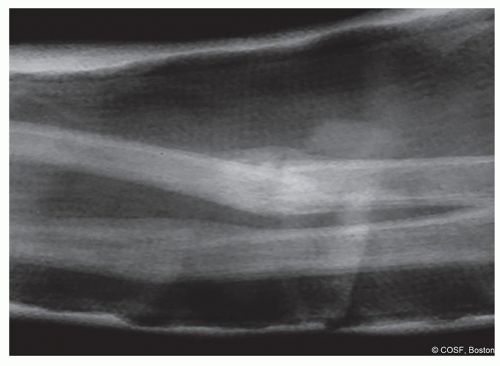 Figure 16-3 ▪ Failure of cast treatment to maintain acceptable alignment radius and ulna diaphyseal fracture. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
Positioning
Supine with radiolucent arm and hand table
Surgical Approach
Extensile exposures—most commonly a subcutaneous approach for the ulna and volar Henry approach to the radius.
Occasionally, a posterior approach to the radius may be indicated, however, not commonly
Preoperative Planning
This is essential
The more time spent here, the better the case will go and the more likely surgery will improve the patient’s problem
Determine the deformity, especially the apex and axis of deformity
Do plain radiographs adequately display the deformity?
Does the clinical examination match the radiographic findings?
Is there a soft-tissue component to the deformity that will not be seen on radiographs?
Long bone radiographs of entire forearm are better for diaphyseal and complex multiplanar deformity planning
Additional joint radiographs can more accurately quantify periarticular deformities
Is this a simple deformity or complex?
The deformity may be more complex when there are
multiple deformities/fractures
joint malalignment
incomplete remodeling
secondary growth arrest
Complex deformities benefit from 3D planning
Standard radiology 3D scans and proprietary options exist
Create an “on paper” template plan using either plain films and/or 3D reconstructions
Determine the location and magnitude of correction
Consider the effect of your correction on the DRUJ and ulna variance
Plan the appropriate fixation
Many metaphyseal deformities in the pediatric and adolescent population can be fixed with K-wires
2.4- and 2.7-mm plates and screws can be good alternatives to 3.5-mm implants in the shaft in the younger patient
Anatomic specific implants commonly will not be suitable
Technique in Steps
Exposure
Through planned ulna and/or radial approaches
Each osteotomy should be performed via a separate incision to minimize the risk of cross union
Longitudinally incise the periosteum for the length of the fixation if using a plate and screws; intramedullary or percutaneous wire fixation requires only subperiosteal elevation at osteotomy site
Only at the osteotomy site does the periosteum need to be elevated circumferentially
Additional subperiosteal elevation may be required to aid fragment mobility
Ensure the periosteum is kept intact—so a biologic envelop surrounds the osteotomy on closure
The intact periosteum also protects the adjacent tendons and neurovascular structures
Planning the Osteotomy in Operating Room After Surgical Exposure
Using your preoperative template, mark the osteotomy
Most commonly with K-wires and fluoroscopy
Keep Control of the Osteotomy at All Times
Periarticular osteotomies should have the articular fragment fixation with plate and distal screws or temporary fixation set prior to making the osteotomy
Fixation should be preset taking into account the corrected position of the distal fragment, so that the wires or plate will intersect the proximal fragment properly in corrected position
This requires biplanar thinking and planning
Diaphyseal osteotomies: As it can be hard to judge rotation after the osteotomy is performed, a longitudinal mark across the planned osteotomy site should be made
This is best with a true indentation in the bone rather than ink alone
Either an osteotome or careful use of a saw
Consider the placement of fixation and direction of any rotatory deformity correction so that these marks can be visualized after correction achieved
If a plate is to be used, commonly this mark can be along either the front or back edge of the plate
Place a line of surgical marker into the groove to help maintain visualization of the mark
Alternate methods of marking include a monopolar diathermy line or ink marker; however, these are more prone to be wiped away during the procedure
When possible, place one side of the fixation prior to performing the osteotomy
Screws partially inserted through the plate and removed make later fixation after manipulation of fragments into corrected position easier
Remember, never lose control of your osteotomy
Most commonly, initial fixation in the proximal shaft for diaphyseal osteotomies is used as it is easier to secondarily manipulate the distal fragment and
Distal fixation in wrist periarticular and distal metaphyseal osteotomies
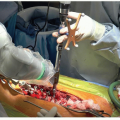
Perform the Osteotomy
Determine if a complete or incomplete osteotomy is required
Most commonly, a complete osteotomy is required in distal radius and forearm diaphyseal corrections
Oscillating saw
Irrigate while sawing, stop frequently to cool the blade, and clean the teeth
Preservation of biology and avoiding necrosis is essential regardless of the method chosen
At times, the only safe way to complete the osteotomy is with an osteotome
Drilling sequential holes and then using osteotome is an alternate lower energy technique
Most common for distal radial metaphyseal 3D deformity (Madelung deformity)
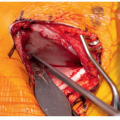
Complete the Correction and Fixation
Based on correction of joint angle for distal radius malunions
Or restoring diaphyseal bony alignment and reducing corresponding proximal and/or distal joint subluxation in diaphyseal malunions
Restore anatomic alignment
Achieve stable internal fixation (Figure 16.4)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree