Radioulnar Synostosis Derotation Osteotomy
Peter M. Waters
Operative Indications
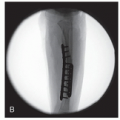
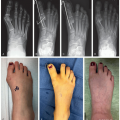
Complete radioulnar congenital synostosis (Figure 13.1)
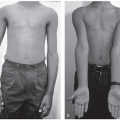
Pronation contracture >60° to >90°, especially if bilateral (Figure 13.2)
Functional limitations in activities of daily living
Alternative Treatments
Natural history adaptations
Adaptable shoulder internal rotation to supinate by back-handing (Figure 13.3)
Palm to ceiling to hold objects
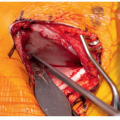
Compensatory increased rotation through radiocarpal joint (Figure 13.4)
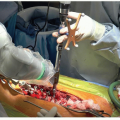
Surgical synostosis excision
Synostosis takedown and interposition arthroplasty (silastic, fat, aconeus, vascularized fascia)
High rate of recurrent synostosis
Even with successful takedown, without recurrence, true forearm rotation only mildly improved
Equipment
Fluoroscopy
Radiolucent arm and hand table
Tourniquet
Power drill
Power saw
Osteotomes
Smooth K-wires
Smooth C-wires
Standard dissecting kit
Casting materials and cast saw
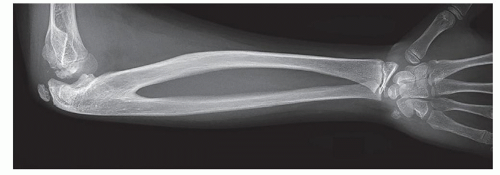 Figure 13-1 ▪ Lateral x-ray showing complete radioulnar synostosis with embedded radial head. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
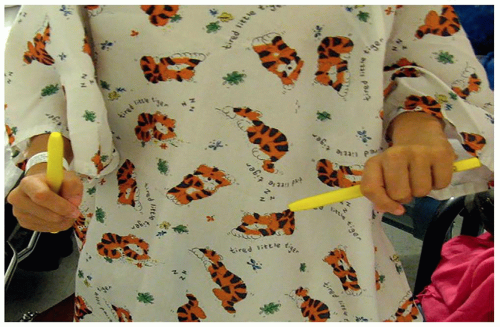 Figure 13-2 ▪ Photograph showing unilateral left radiolunar synostosis in >90° forearm hyperpronation and opposite side in neutral as indicated by surgical marking pen positioning in both hands. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
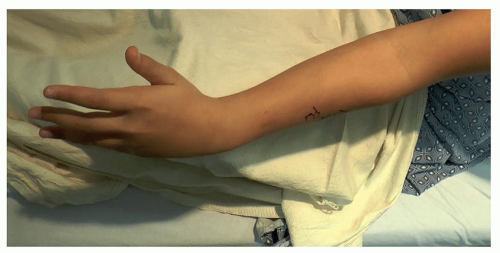 Figure 13-3 ▪ Photograph of increased shoulder external rotation in an attempt to supinate to put objects in palm of hand. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
Positioning
Supine with operative arm on radiolucent table
Surgical Approach
Use lateral fluoroscopy to identify the synostosis, proximal and distal extent of radioulnar synostosis (RUS), ulnotrochlear joint
Mark skin to aid percutaneous technique
Use fluoroscopy to identify medullary canal ulna
Choose wire diameter that will fill 50%-75% of the ulna medullary canal
Identify entry site olecranon apophysis (Figure 13.6)
Medullary canal usually thinner than expected
Choose smaller diameter smooth wire to fit full-length ulna
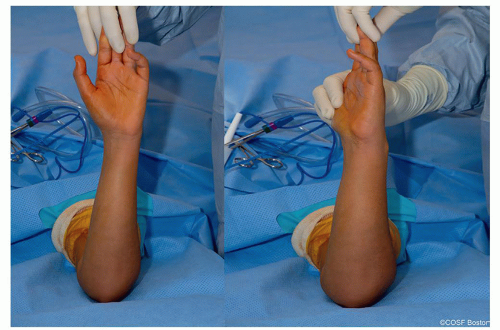
Figure 13-4 ▪ Pictures in operating room of wrist rotation with complete radioulnar synostosis in 80° pronation. Left image is natural state and right image is passive supination through radiocarpal joint. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
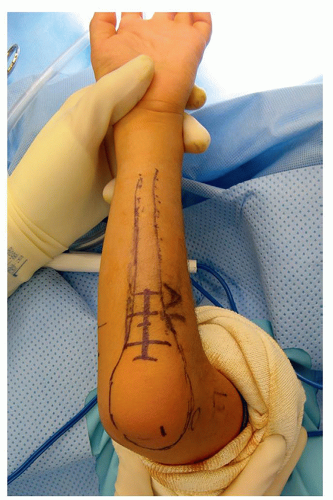
Figure 13-5 ▪ Photograph of surgical exposure to ulnar border as outlined by incision marking with cross hatching marks the length of the incision. The contour outline of ulna marked from olecranon distally. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
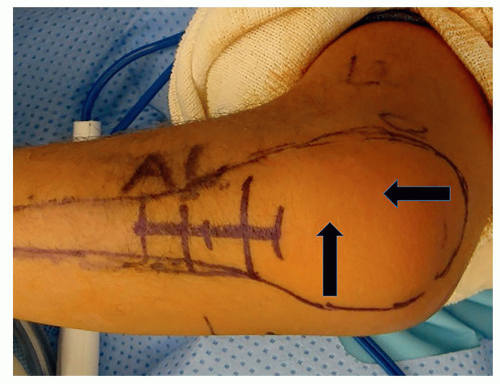
Figure 13-6 ▪ Photograph of skin markings for proximal, distal, and midportion of radiolunar synostosis for surgical exposure. Horizontal arrow indicates apophysis entry that corresponds to proximal ulna medullary canal. Vertical arrow indicates ulnotrochlear joint. (Courtesy of Children’s Orthopaedic Surgery Foundation.)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access