Surgical Management of Crouched Gait
Colyn J. Watkins
Anterior Screw Hemiepiphysiodesis With Medial Hamstring Release
Operative Indications
Crouch get with knee flexion contracture (>10°) in a child with older than 2 years of growth remaining and no evidence of knee pain (Gross Motor Function Classification System [GMFCS] I-III)
Knee flexion contracture greater than 20° in minimally ambulant children (GMFCS IV/V) who wish to maintain a standing program and prevent progressive knee flexion contracture
Be cautious in children who are overweight or have a large thigh as access to the medial screw can be challenging due to the presence of the contralateral leg
Preoperative Evaluation
Bone age is often helpful as dysmorphic bones in neuromuscular conditions can make amount of growth remaining somewhat difficult to interpret
Prone evaluation critical to assess for knee flexion contracture versus hamstring tightness
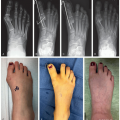
Obtain lateral radiograph in maximal extension
Consider concomitant hamstring lengthening and hip flexor lengthening
Equipment
4.5 mm cannulated screws fully threaded
Large bump or small radiolucent triangle
C-arm with lateral c-arm drape
Usual small instrument kit
NO tourniquet
Bilateral extremity drape and impervious stockinettes
Foot extension if patient is small enough
Positioning
Supine positioning on radiolucent table with arms across chest (so that arms do not get in the way with trajectory of the screws)
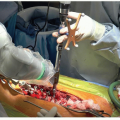
Hamstring Release
Generally done first before screw application only if hamstrings are tight
4 to 5 cm medial longitudinal incision over the palpable medial semitendinosus and gracilis tendons
These 2 tendons are almost immediately palpable in the incision. Semitendinosus is more lateral and larger. Gracilis can be identified with abduction and extension of the leg. The semimembranosus is a broader muscle which is found 1 layer deeper between the 2 tendons
Semitendinosus and gracilis can be isolated in their sheaths with electrocautery in line with tendon. They are then isolated and tenotomized with cautery
The semimembranosus is then palpated deep to these tendons and its aponeurosis identified. This is then released, leaving the muscle beneath intact
Hamstring Pearls and Pitfalls
If doing this operation with a novice, consider asking the scrub nurse to manage the leg in smaller patients. This allows the surgeon and trainee to go to the contralateral side of the table and both see into the wound. It can be difficult to see into the wound as the person holding the leg up for the operating surgeon
Remember medial to semitendinosus/semimembranosus is a generally safe dissection plane; the bundle is found lateral to these structures
In some situations can consider semitendinosus transfer around the adductor tubercle distally to maintain pelvic position and prevent excessive anterior pelvic tilt (see SEMLS chapter 36)
Screw Hemiepiphysiodesis
The C-arm can come in from whichever side of the room has more space
Generally starting with the lateral screw is the easiest and safest as there are no NV structures at risk on that side
A 20G spinal needle is advanced down to the bone, just proximal to the flare of the condyle, and image is taken to ensure an appropriate trajectory
Typically, this is just less three fingerbreadths above the superior pole of the patella (Figure 38.1)
The skin is then incised 1 cm in length just anterior or posterior to this needle (Figure 38.2)
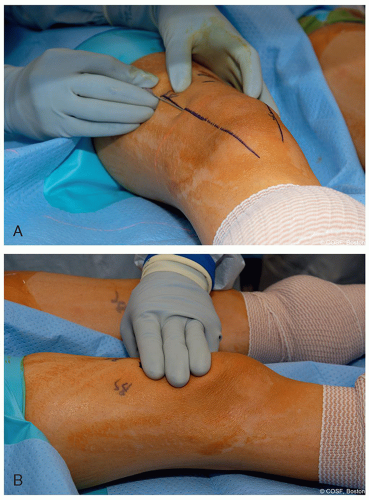
Figure 38-1 ▪ A spinal needle can be used to template your start point for the 4.5 mm guidewire note about 2 to 3 fingerbreadth above the top of the patella. (Courtesy of Children’s Orthopaedic Surgery Foundation.)

Figure 38-2 ▪ A small 1 cm incision is made either anterior or posterior to your spinal needle, and on the lateral side, the knife is incised through the iliotibial band. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
A 1.6 mm guidewire is then taken by hand and advanced to the cortex of the bone and malleted such that the tip is just into the bone in the correct trajectory, both in the sagittal and coronal plane
The wire is then advanced up to the physis, palpating and aiming for the anterior-most portion of the femoral condyle
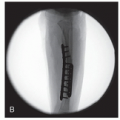
A lateral image to check wire position—goal is to cross the physis in the anterior 1/3 on the sagittal plane (Figure 38.3)
The same procedure is then completed on the medial side
Both wires can be placed and then standard cannulated screw technique to place the screws. Be aware as bone is soft and only need to drill to lateral cortex and not past the physis
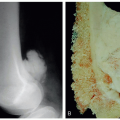
Note the trajectory for the wires is such that your wire ends up against the quadriceps proximally (Figure 38.4)
Three threads across the physis—this should be assessed on the lateral image
Ensuring that you are out of the patellofemoral and femor-tibial joint is critical
Leave screws proud if considering removal in the future
Screw Epiphysiodesis Pearls and Pitfalls
A perfect lateral image of the distal femur must be obtained before finishing. The screw tips must be within the intercondylar line on the lateral
Screw must be anterior to the distal tip of the intercondylar line of the femur
Do not use a tourniquet
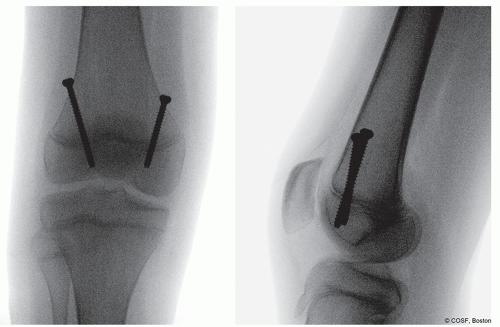 Figure 38-3 ▪ The position of the guidewire on the anteroposterior (AP) and lateral plane, on the AP view, the wire should split the distance between the medial and lateral half of the distal femur, and on the lateral view, the wire should cross the physis in the anterior 1/3 of the epiphysis with at least 3 threads across the physis. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
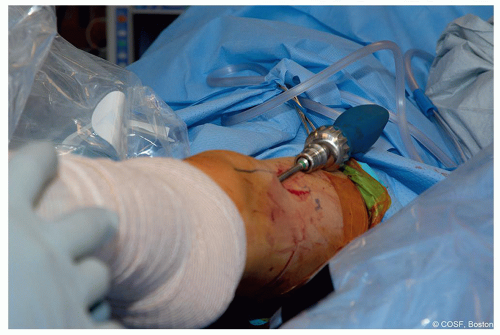 Figure 38-4 ▪ Note that the screw trajectory is such that the wires run very close to the quadriceps both medially and laterally. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
Postoperative Care
Knee immobilizers immediately postop for 3 weeks to help with weight-bearing and support
At 3 weeks, check incisions and switch immobilizers to night-time only
WBAT right after surgery
Start ROM and therapy about 1 week after surgery as tolerated
Complications
Iatrogenic nerve stretch
Avoid intraoperative knee popliteal angle testing
Over-lengthening and anterior pelvic tilt
Lateral hamstring release generally unnecessary and can lead to excessive anterior pelvic tilt
Incomplete correction/asymmetric correction
Maintain close follow-up and ensure that medial and lateral screws are across the physis
Distal Femoral Extension Osteotomy With Cannulated Blade Plate and Soft Tissue Patellar Tendon Advancement
Operative Indications
Crouch gait with knee flexion contracture (>10°) in a skeletally mature adolescent or greater than 20° in a growing child who is symptomatic and guided growth is not an option
Knee flexion contracture greater than 20° in minimally ambulant patients who wish to maintain use of stander and transfers
Obesity and inability to participate in postoperative rehab protocols are relative contraindicationsRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree