Surgical Scar Revision
Matthias B. Donelan
Benjamin Levi
Curtis Gaball
KEY POINTS
All injuries to the skin that significantly damage the papillary dermis result in scars.
Scars are not inherently bad, they are an essential part of life.
Scar revision improves scars by favorably altering their characteristics, not necessarily by excising them.
Scar revision has been greatly improved by a more thorough understanding of scar maturation and novel technologies.
Scar revision requires analysis, diagnosis, treatment selection, surgical technique, and total patient care. That makes it an infinitely challenging and rewarding part of plastic surgery.
A long-term view of how scars have been managed over the course of medical history is informative and gives perspective (see Chapter 1). The management of scars can be divided into five different eras:
Prior to the development of anesthesia there was primarily acceptance and disguise, except for totally life-altering deformities (e.g., nasal reconstruction for punitive amputation).
After the emergence of anesthesia (both general and local) in the late 19th century, there was a burgeoning interest, and an extensive literature, in scar revision techniques. Among these the Z-plasty is most notable.
After World War I, scar excision and resurfacing gained popularity following Sir Harold Gillies’ monumental work on soldiers using flaps to restore facial appearance.
During the mid- to late 20th century, scar excision and ever more complex replacement with the patient’s other undamaged body parts has dominated thinking, particularly for large scars.
In the 21st century, scar rehabilitation—preserving original tissue—and regeneration have the potential to revolutionize how we “revise” scars.
Without scars there would be no wound healing, so scars are an essential part of life. The goal of this chapter on surgical scar revision is to demonstrate how understanding scar etiology and pathogenesis enables us to enhance normal wound healing during surgical scar revision therapy. We have now reached a point where scar excision is often not the best option for improving scars; there is nothing like original equipment in its original location. Understanding how and why scars heal well or unsatisfactorily is a fascinating and evolving process. Careful analysis of an individual scar’s qualities is the most essential part of planning a successful scar revision procedure.
The term “scar” originates from the Greek word “eskara,” meaning the scab (eschar), or wound caused by burning. It has come to mean any visible mark remaining after the healing of a wound or other pathological process. “Scar” is therefore a term applied to a wide range of visible skin abnormalities that can be composed of very different kinds of pathologic tissue, with or without pigmentary abnormalities. These include such varied presentations as linear surgical scars, hypertrophic burn scars, atrophic scars (such as those that follow severe acne), and skin grafts placed during reconstruction; each presents different clinical problems.
All scars are unique, but from a strategic thinking standpoint they can be roughly divided into four fundamentally different categories.
Category I: Linear scars from an incision or laceration through the full thickness of the dermis without “significant” associated tissue loss. Their most important attribute is their relationship to relaxed skin tension lines (RSTLs)1,2 (Figs. 12-1 and 12-2).
Category II: Scars following injury to the mid- to deep dermis from burns or trauma that have not completely transected the dermis, but are conspicuous and have associated hypertrophy and contractures (Fig. 12-3).
Category III: Scars associated with full-thickness loss of the integument and deeper tissues from trauma, surgical resection, or extensive third-degree burn injury (Fig. 12-4).
Category IV: Keloid scars, a benign proliferative disease process that behaves differently from other physiologic scarring processes (Fig. 12-5).
Appreciating the environment within which an individual scar lives is an essential factor in planning scar revision, particularly the presence of tension and an awareness of absolute tissue loss (see Chapter 7). Each of the above four categories presents different challenges and opportunities
for surgical scar revision. It is of critical importance to understand these differences in order to determine the most appropriate treatment plan. Scar orientation is of profound importance and plays a role in all categories except IV.1 RSTLs differ from Langer’s lines and most closely follow natural wrinkle lines, particularly in the head and neck (Fig. 12-1A). These lines are usually perpendicular to the orientation of the muscles beneath (Fig. 12-1B). They also can be identified by gentle compression of the skin.1,3 Elective incisions should be made as much as possible along these lines in order to obtain the best healing (Fig. 12-6A, B).
for surgical scar revision. It is of critical importance to understand these differences in order to determine the most appropriate treatment plan. Scar orientation is of profound importance and plays a role in all categories except IV.1 RSTLs differ from Langer’s lines and most closely follow natural wrinkle lines, particularly in the head and neck (Fig. 12-1A). These lines are usually perpendicular to the orientation of the muscles beneath (Fig. 12-1B). They also can be identified by gentle compression of the skin.1,3 Elective incisions should be made as much as possible along these lines in order to obtain the best healing (Fig. 12-6A, B).
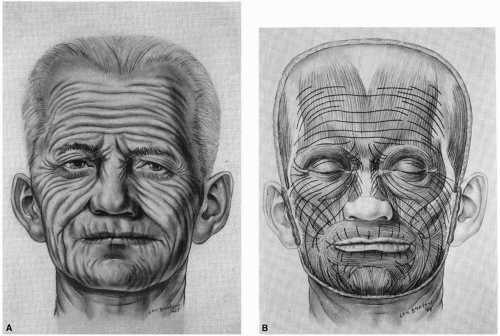 FIGURE 12-1 A: Relaxed skin tension lines (RSTLs) differ from Langer’s lines and most closely follow the natural wrinkle lines, as demonstrated in this facial schematic. B: RSTLs are usually perpendicular to the orientation of the muscles beneath. (Kraisel CJ. The selection of appropriate lines for elective surgical incisions. Plast Reconstr Surg. 1951;8:1-28.) |
 FIGURE 12-2 Traumatic lacerations which do not follow relaxed skin tension lines, particularly if they are perpendicular to them as in this example, heal unfavorably. (From Krakowski AC, Totri CR, Donelan MB, Shumaker PR. Scar management in the pediatric and adolescent populations. Pediatrics. 2016;137(2):e20142065.) |
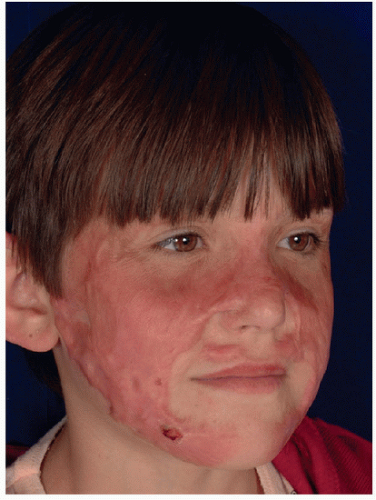 FIGURE 12-3 A 11-year-old girl who sustained mixed second- and third-degree facial burns. One year after the injury they have healed with contraction, hypertrophy, and ulceration. |
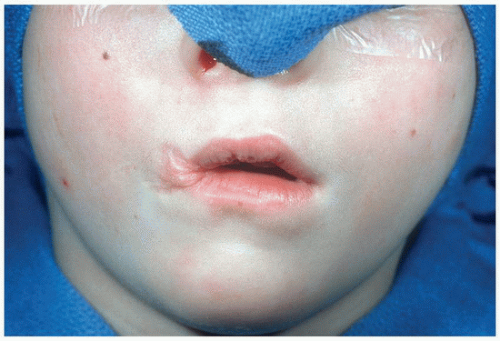 FIGURE 12-4 A 5-year-old child who sustained an electrical burn injury to the right oral commissure with full-thickness loss of vermilion, muscle, mucosa, and skin. His deformity has extensive contractures with displacement of the philtrum and the midpoint of the lower lip. |
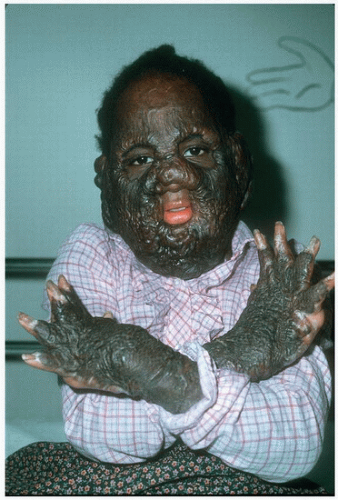 FIGURE 12-5 A 10-year-old girl following a second- and third-degree burn injury with massive keloid scar formation in all areas, including donor sites. |
 FIGURE 12-6 A: A 20-year-old woman who had always been reluctant to have her congenital nevus excised because of concerns about a scar. B: Scars parallel to RSTLs result in the best possible healing for both elective incisions and traumatic lacerations. Fusiform scar revision should always adhere as much as possible to this principle. |
The decision of whether to treat or not to treat an “unsatisfactory” scar is extremely important (see Chapter 4). Some scars are unsatisfactory because they restrict range of motion or distort facial features; others, despite being very subtle, are objectionable because they evoke unpleasant memories. The perspectives of the patient and the evaluating surgeon are often very different. The patient frequently desires that the scar be “removed,” as
in eliminated completely. This is clearly not possible. The surgeon must determine which scars are possible to improve and whether the improvement will be adequate to make an individual patient pleased with the outcome. Arriving at a satisfactory meeting of the minds is an essential first step in creating reasonable patient expectations. Creating that joint understanding is a subtle but important learned skill that is an integral part of successful scar revision surgery. In some cases the decision is easy to make. For example, a linear scar on the face that is unfavorably oriented to RSTLs, and has an unsatisfactory appearance because of either hypertrophy or widening with atrophy, almost always can be improved by a correctly performed surgical scar revision (Fig. 12-7).
in eliminated completely. This is clearly not possible. The surgeon must determine which scars are possible to improve and whether the improvement will be adequate to make an individual patient pleased with the outcome. Arriving at a satisfactory meeting of the minds is an essential first step in creating reasonable patient expectations. Creating that joint understanding is a subtle but important learned skill that is an integral part of successful scar revision surgery. In some cases the decision is easy to make. For example, a linear scar on the face that is unfavorably oriented to RSTLs, and has an unsatisfactory appearance because of either hypertrophy or widening with atrophy, almost always can be improved by a correctly performed surgical scar revision (Fig. 12-7).
Goals of Scar Revision
The overriding goal is to unequivocally improve the appearance of the scar. Simply creating a new deformity to modify an old one is not a successful outcome. Surgery should only be undertaken when the surgeon feels confident that the scar will be made clearly better to both patient and surgeon. There should be minimal to no additional iatrogenic deformity caused by the scar revision procedure. When possible, favorably altering the environment in which the scar will heal is very beneficial. Decreasing or eliminating tension is of the utmost importance. Using lasers for drug delivery, to obscure scar margins, and to initiate scar remodeling/regeneration are new game-changing advances, discussed in detail in other chapters (see Chapters 13 and 14).
 FIGURE 12-7 A: Transverse facial laceration perpendicular to relaxed skin tension lines with widening and atrophy. B: The atrophic depressed scar was excised and the defect closed incorporating four Z-plasties with the lateral limbs oriented parallel to relaxed skin tension lines. C: The most posterior extent of the excision was not closed with Z-plasties. That area widened again and 2 years later it was revised with two Z-plasties similarly oriented to the original excision. D: Six years following the last scar revision the deformity is not noticeable. (From Krakowski AC, Totri CR, Donelan MB, Shumaker PR. Scar management in the pediatric and adolescent populations. Pediatrics. 2016;137(2):e20142065.) |
Category I: Scars parallel to RSTLs in general are favorable and usually cannot be improved by revisional surgery.2 Antitension line (ATL) scars, which are unfavorably oriented to RSTLs, frequently result in hypertrophy, atrophy, “trapdooring,” and widening and can frequently be improved by scar revision. With experience, and taking these simple factors into consideration, it is a rare unsatisfactory linear scar that cannot be improved.
Category II: Scars require an accurate diagnosis of what has caused their unsatisfactory characteristics, followed by a rehabilitative approach that eliminates tension and facilitates scar remodeling.
Category III: Scars require the provision of adequate tissue to enable the best possible restoration of satisfactory appearance.
Category IV: Keloid scars are unsolved clinical and surgical problems, often requiring multimodal therapies geared toward palliation and symptomatic improvement.
Surgical Technique
It goes without saying that scar revision surgery must be performed well. The plan must make sense, and the execution
must be meticulous. Basic surgical techniques are described in detail in many excellent texts,4,5,6 and only a few relevant caveats will be highlighted here. Incisions must be made exactly perpendicular to the skin’s surface unless specific local conditions, such as hair follicle angulation, dictate a different approach. When dealing with tissue that includes a combination of indurated scar and uninjured skin, scalpel control is extremely important. The different resistance of the tissues can easily result in inaccurate incisions. Preserving the minimally injured skin at the margin of a scar can be helpful in masking the transition from normal skin into the reconstructed area, and helps with camouflage. Surgical incisions made in normal skin always heal with the appearance of a surgical scar and this looks unnatural in most circumstances.
must be meticulous. Basic surgical techniques are described in detail in many excellent texts,4,5,6 and only a few relevant caveats will be highlighted here. Incisions must be made exactly perpendicular to the skin’s surface unless specific local conditions, such as hair follicle angulation, dictate a different approach. When dealing with tissue that includes a combination of indurated scar and uninjured skin, scalpel control is extremely important. The different resistance of the tissues can easily result in inaccurate incisions. Preserving the minimally injured skin at the margin of a scar can be helpful in masking the transition from normal skin into the reconstructed area, and helps with camouflage. Surgical incisions made in normal skin always heal with the appearance of a surgical scar and this looks unnatural in most circumstances.
Scar Analysis
Everyone can treat, but few can diagnose.
—Dr. Samuel Moschella
Many factors play a role in whether a scar has healed in a satisfactory or unsatisfactory fashion. It is mandatory to take a complete history to understand the etiology and pathogenesis of an individual scar. If previous attempts at revision have occurred, details of treatment should be obtained to avoid a repeat disappointment. Important physical findings to note include anatomical location, orientation to RSTLs, shape, hypertrophy or atrophy, presence of tension, pigmentation, step-off deformities, presence of extrinsic contractures, patient age, scar maturity, and the presence of foreign bodies.
Anatomic Region
Scars on the face tend to heal more favorably than scars in other areas of the body. Favorably oriented scars on the face can end up looking much like normal skin lines. Neck skin is notorious for poor healing, perhaps because it is thin and has fewer skin appendages. Linear scars in other areas, such as the deltoid region, the presternal area, and around the knee, frequently result in widening, hypertrophy, and an unsightly appearance. Scars on the trunk have much more of a propensity to widen than do scars in the region of the head and neck, even if they approximate RSTLs.
Orientation
As noted, this is probably the most important component for linear scars. “Practically speaking few tension lines (TL) scars are unaesthetic, but most, if not all, anti-tension lines (ATL) scars are unsatisfactory.”2
Hypertrophic Scars
Hypertrophic scars are a normal physiologic response of the skin to trauma, influenced by multiple factors which cause them to hypertrophy (see Chapter 6). Keloid scars, on the other hand, are a benign proliferative diathesis leading to hypertrophy that is not in response to normal physiologic stimuli (see Chapter 5). Hypertrophic scars can be improved by correct diagnosis and appropriate scar revision. Keloid scars are a completely separate entity and will be discussed separately in Category IV.
It is essential to diagnose the etiology of the hypertrophic scar. Is it hypertrophied because of an unfavorable orientation to RSTL? Is it hypertrophic because it was a partial-thickness burn injury which has contracted and is now under tension? Is it the result of tension and relaxation across a flexion joint, or because it bridges a concavity? Is it the result of healing complicated by infection or foreign bodies? Before embarking on the correction of a hypertrophic scar, the etiology must be diagnosed and there must be a plan to favorably alter the factors that resulted in the hypertrophy.
Depressed Scars
Depressed scars can result from unfavorable orientation, fat atrophy following a contusion or laceration, loss of tissue, or adhesions between the surface of the scar and the underlying deep structures such as fascia. Depressed scars are frequently seen as a result of overly aggressive steroid injection for hypertrophic scars (Fig. 12-8). When atrophy is present, regardless of etiology (with the frequent exception of steroid-induced atrophy), it is often necessary to remove all or part of the atrophic tissue (Fig. 12-7). Fat grafting can be helpful in selected cases (see Chapter 15). Because the transposed limbs of Z-plasties originate from the level surface of the normal skin on either side of a depression they can be very effective in elevating depressed scars.
Shape
Curvilinear scars create a trapdoor effect because of the tightening of the margin of the scar like a “purse string.” Lengthening the scar by multiple Z-plasties, with the limbs of the Z-plasties paralleling RSTLs as one moves along the curvilinear scar, is a uniformly successful technique in the authors’ experience.
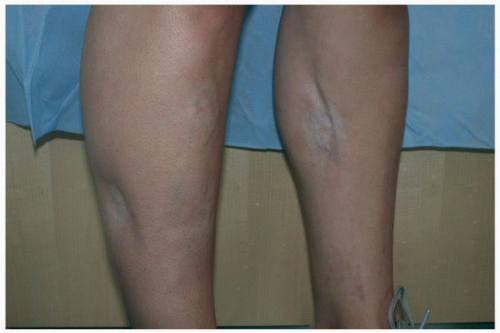 FIGURE 12-8 A 20-year-old woman athlete who underwent elective orthopedic fasciotomies for compartment syndrome. Following multiple steroid injections for hypertrophic scarring she developed severe atrophy of both the skin and subcutaneous fat. |
Step-off Deformities
These are usually the result of an inadequate, or absent, closure of a laceration. This type of deformity, once clearly diagnosed, requires reopening of the scar and then appropriate, meticulous, closure. If the scar is unfavorably oriented, such that unfavorable future healing is likely, appropriate revisional techniques should be considered at the same time. Otherwise, a careful simple closure is adequate.
Patient Age
The very young and the very old heal with the best scars. Adolescents are the healthiest patients and make the most exuberant scars.
Scar Maturity
As mentioned under hypertrophic scars, the timing of the scar analysis is pivotal as scars go through a normal maturation phase that lasts for years. A hypertrophic scar in a fair-skinned blue-eyed patient which is extremely erythematous, even though favorably oriented, is likely to mature well if given enough time. Experience is very important, as well as patient patience, in determining when and how to intervene after a scar has become unsatisfactory.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


