Scar management in patients with skin of color requires a varying set of considerations compared to patients without substantial constitutive pigmentation. Hyperpigmentation and hypopigmentation may both be more prominent at initial presentation, pathologic scars are more common, and the tendency toward hyperpigmentation following various treatment interventions must be more thoroughly accounted for.
Scar appearance can be improved with repeated sessions of minimally invasive modalities such as the vasculature-targeting pulsed dye laser and fractional resurfacing technology to induce collagen remodeling.
Intralesional corticosteroid combined with 5-fluorouracil remains a mainstay in the treatment of hypertrophic scars and keloids in skin of color.
Early intervention with fractional laser devices appears to improve the appearance and function of atrophic and hypertrophic scars. A lower density of microscopic treatment zones is preferred for skin of color to minimize the risk of postinflammatory hyperpigmentation.
Different subtypes of scars require varying combinations of treatment modalities, preferably at an early stage of scar formation. Darker skin tones require lower treatment densities and greater attention to epidermal cooling for optimal laser efficacy and safety.
Scars are a common reason for consultation in clinicians’ offices. They develop during the normal wound-healing response when connective tissue replaces lost tissue in the dermis or deeper planes because of injury or various inflammatory conditions. Frequent causes of scars include surgery, burns and other trauma, acne, body piercing, tattoos, and infections. Scars frequently lead to unfavorable cosmetic outcomes with associated symptoms such as pruritus and contractures that may impair limb function. “Skin of color,” also referred to as ethnic skin, describes individuals with greater constitutive pigmentation, including those of African, Asian, Hispanic, Native American, Middle Eastern, and Pacific Island backgrounds with Fitzpatrick skin types III to VI based on the assessment of the burning and tanning histories of each individual (Table 18-1). The current system may have limitations as little data have been reported on skin responses for populations with dark skin color. Skin of color carries a higher risk of keloid and hypertrophic scar formation, and postinflammatory hyperpigmentation (PIH) of atrophic scars also poses a significant potential cosmetic impact.
There are a multitude of treatment modalities described for scar management, but standard treatment protocols are lacking because of a paucity of controlled therapeutic studies, especially in skin of color. The importance of ultraviolet protection (including sun avoidance and sunscreen use in the early period after wounding) to prevent scar hyperpigmentation and postlaser PIH cannot be overemphasized. PIH is most prominent in the skin of color and can be observed in scars and after laser treatment. Inflammation induced by sun exposure or injury is often accompanied by pigmentary alteration in darker skin types.
Apart from the cross-talk between keratinocytes and melanocytes in the control of melanocyte function, increasing evidence has highlighted the critical role played by the interactions between mesenchymal and epithelial cells mediated through the release of fibroblast-derived growth factors. In particular, keratinocyte growth factor (KGF), in combination with interleukin (IL)-1α, induces melanin deposition in vitro and hyperpigmented lesions in vivo. Furthermore, a moderate increase of KGF and induction of its receptor have been shown in sun-damaged lesions, suggesting the involvement of this growth factor in the onset of the hyperpigmentation.1 The risk of PIH appears to be related to the degree of disruption of the dermoepidermal junction (DEJ) during laser resurfacing, and the subsequent inflammation at the DEJ with pigmentary incontinence (analogous to the interface dermatitis in lichen planus).
Currently available therapies include topical medications and intralesional injections, silicone-based sheets, compression therapy, cryotherapy, radiation, surgical revision, and laser therapy (see Chapter 10).2 A variety of lasers can be applied based on different scar subtypes in darker skin provided that appropriate treatment parameters and cooling methods are used3 (see Chapter 13). Most treatments carry a higher risk of adverse effects in this population, such as the propensity to develop pathologic scars and pigmentary alteration, owing to higher melanin content in the epidermis. In general, darker skin tones require lower fluences, greater attention to epidermal cooling when using pulsed dye laser (PDL), and lower treatment densities when using fractional lasers for optimal efficacy and safety (Table 18-2).
Table 18-1 Fitzpatrick’s Classification of Skin Phototypes
Phototype
Basic Skin Color
Response to Sun Exposure
I
Pale white
Burns easily; does not tan
II
White
Burns easily; tans with difficulty
III
White
May burn initially but tans easily
IV
Light brown/olive
Hardly burns; tans easily
V
Brown
Usually does not burn; tans easily
VI
Black
Does not burn; becomes darker
From Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Arch Dermatol. 1988;124:869-871.
Table 18-2 Minimizing the Risk of PIH Associated with Laser Treatment in Skin of Color
Ensure adequate sun protection in the pre- and postoperative periods
Pretreatment with topical bleaching agents is not effective
When using fractional lasers, decrease treatment density and the number of passes in each session, and increase the number of sessions and interval between treatments (at least 4-6 wk)
Ensure adequate epidermal cooling; when using a pulsed dye laser, settings of 40 ms dynamic cooling spray and 20 ms delay are recommended
Topical corticosteroid use is recommended if significant and persistent erythema is observed after laser treatment
FIGURE 18-1 Left: Icepick scars with a sharp, demarcated V-shaped configuration reaching to the deep dermis. Right: Rolling scars with broad ill-defined superficial depressions of the skin.
Types of Scars
Proper recognition and classification of scars is essential for selecting the optimal treatment modalities (see Chapter 5). Scars present with various morphologies and are generally classified into hypertrophic and atrophic subtypes. Keloids and hypertrophic scars result from excessive fibrotic tissue formation, and occur less frequently than atrophic scars on the face. Atrophic acne scars are further classified into ice-pick, rolling, shallow, and deep boxcar scars, and are the result of compromised collagen production and increased degradation during the natural wound-healing process following inflammation or injury, which leads to surface undulations4 (see Chapter 17) (Fig. 18-1).
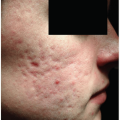
Pathologic scars (hypertrophic scars and keloids) result from an aberrant wound-healing response and are seen in ethnic skin at rates ranging from 3- to 18-fold higher than in Caucasians. The incidence of keloids is 4.5% to 16% in skin of color, including African and Hispanic populations, especially in the second and third decades of life.3 Predisposing factors include location (particularly on jaw line, upper chest, sternal area, shoulder, upper back, and earlobe), race, family history, and past history of tendency to scar. Differences in scar characteristics between skin of color and Caucasian skin include an increased risk of hypertrophic scars and keloids with PIH. In addition, prolonged erythema, pigmentary alteration, hypertrophic scarring, and longer recovery period are more likely to occur in darker skin types (Fig. 18-2).
Hypertrophic scars differ from keloids in a number of ways. Hypertrophic scars are pink scars that are confined within the borders of the original wound, and they tend to improve over time. Keloids often form nodules and plaques of deep red color that extend beyond the original wound border with claw-like projections. The lesions may occur months or even years following injury, and they tend to enlarge and recur over time despite treatment. The lesions are disfiguring and are frequently associated with pain and pruritus. Histopathologically, keloids are composed of thick, disorganized collagen fibers with abundant mucoid matrix, whereas hypertrophic scars are comprised of more organized parallel collagen fibers within scanty mucoid matrix5 (see Chapter 5).
FIGURE 18-2 Postinflammatory hyperpigmentation on right temporal and malar areas associated with active inflammatory acne in a Chinese man.
Atrophic facial scarring is a common long-term complication of moderate to severe acne, and patients with inflammatory acne should be counseled early that they have a significant risk of scar development. Every effort should be made to treat the inflammatory lesions and prevent this long-lasting complication. Acne scars can have substantial cosmetic and psychological effects, particularly in adolescence and young adulthood. Concerns about PIH and scarring are one of the main motivational factors that lead patients to seek treatment for acne.6 The precise prevalence of acne scarring is unknown. One community-based study reported the presence of acne scars in 14% of women and 11% of men aged 25 to 58 years.7 Most patients presented with macular atrophic or ice-pick scars. Other studies reported that between 30% and 95% of patients with acne developed some form of associated scarring, and a higher incidence of scarring on the trunk was observed in men.8
Pathophysiology of Scarring
The exact mechanism of scar formation has not been fully elucidated (see Chapter 6). Inflammatory acne lesions often lead to atrophic scarring, and the formation of acne scars of various morphologies depends on the degree, depth, and duration of inflammation and on the extent of tissue damage.9 Acne scars are the result of a suboptimal wound-healing process that involves inflammation, granulation tissue formation with fibroplasia and new vessel formation during the proliferative phase, and wound contracture and tissue remodeling.10
Wound healing involves a stepwise process consisting of multiple overlapping phases including inflammation, proliferation, and remodeling. Tumor necrosis factor β and IL-6 appear to play a role in the scarring process.2 Under normal circumstances, the immature scar passes into the final maturation phase, with degradation of the extracellular matrix and transformation of the immature type III collagen of early wound into mature type I collagen. The delicate balance of synthesis and degradation of different scar components is tightly regulated by a number of molecules, particularly epidermal growth factor, TGF-β, matrix metalloproteinases (MMPs), and basic fibroblast growth factor. The delay in regression of angiogenesis also contributes to persistent erythema in incipient pathologic scars.11 Deep scars are more liable to occur when the destruction of subcutaneous fat is involved in the inflammatory process, because the enzymatic activity and inflammatory mediators also destroy the deeper tissue.
It is not clear why some wounds heal to become atrophic scars whereas others become hypertrophic. An abnormal healing response with persistent collagen production, unbalanced production of collagen type I relative to that of collagen type III, abnormal expression of a variety of growth factors, and dysregulation of the extracellular matrix have all been implicated in the formation of keloids, which tend to occur in families with a racial predisposition for dark skin. TGF-β is overproduced in keloids with a loss of feedback control during the production of collagen and the extracellular matrix.12 Hypertrophic scars are primarily composed of well-organized bundles of type III collagen, whereas keloids contain disorganized type I and III collagen bundles. Fibroblasts in keloids have a greater number of growth factor receptors and thus an increased sensitivity to growth factor stimulation, particularly platelet-derived growth factor and TGF-β.13 The use of topical agents such as retinoids to treat acne may help to modulate the course of wound healing and prevent acne scar formation.14
Prevention and Minimization of Pathologic Scars
For those patients with a family or personal history of pathologic scarring after surgery or injury, elective invasive procedures of the skin are best avoided. This is especially true over high-risk areas such as the chest, shoulders, beard area, and earlobes. The current trend is early intervention after surgery to modulate scar formation (Table 18-3) (see Chapters 8 and 9). Optimization of the wound-healing response with early interventions such as a vascular-specific 595-nm PDL and the use of occlusive dressings may help minimize the development of hypertrophic scars or keloids. A reduction of the pigmentation and vascularity of newly revised surgical scars has been demonstrated by the application of silicone gel sheeting daily for 3 months after surgery in Asian patients.15 Topical silicone gel has also been shown to minimize the formation of hypertrophic scars in the early postoperative period after sternotomy in Asian patients.16 Intervention with laser treatment within the first weeks of the scar remodeling process after suture removal has been shown to ultimately reduce the amount of scar tissue formed.17 Early postoperative intralesional injection of 2 mg per mL triamcinolone acetonide combined with PDL treatment using subpurpuric settings has also been shown to minimize the development of hypertrophic scars after thyroidectomy in Asian patients.18 In the experience of the authors, scars earlier in the remodeling process seem to respond better and required fewer treatment sessions than more mature scars, indicating that proactive laser intervention may better modulate the wound-healing response. To prevent keloid or hypertrophic scar formation, scars should always be reevaluated 4 to 8 weeks after surgery to determine if further scar therapeutic interventions are needed. Intralesional injection of corticosteroid plus 5-fluorouracil (5-FU) should be considered once scar thickness increases, indicating the development of pathologic scars.
Table 18-3 Prevention of Keloid and Hypertrophic Scars in Skin of Color
Avoid invasive procedures to high-risk areas, such as upper torso
Employ occlusive dressings or topical silicone-based material
Consider early postoperative use of potent topical corticosteroids, such as clobetasol propionate 0.05%, to scars on limbs and fusidic acid/betamethasone cream to areas prone to develop folliculitis
Modulate wound healing by early use of the pulsed dye laser 2 weeks after surgery, or when stitches are removed. Doses are usually subpurpuric: 595 nm, pulse width 450 µs, 4.75-5.25 J/cm2, spot size 12 mm, 10% overlap, 2-3 passes, DCD 40/20 ms
Early intralesional corticosteroid plus 5-FU injection if pathologic scars start to develop
Patients who have nodulocystic acne with intense visible inflammation are more liable to develop scarring, particularly when there is a delay in the effective treatment of the problem. In contrast, scarring may occur early regardless of the severity of the acne. Thus, the early treatment of acne is of paramount importance to reduce the risk of scarring. Retinoids have been shown to reduce the inflammation in acne by the inhibition of leukocyte migration in the skin, and oral isotretinoin reduces the expression of MMP-9 and MMP-13 in the sebum of acne patients. This may prevent acne scar formation by normalizing the balance of MMPs and tissue inhibitors.19 In the practice of the authors, intervention with lasers can be considered 6 months after completion of isotretinoin therapy for acne.
Treatment of Hypertrophic Scars and Keloids
Pathologic scars including hypertrophic scars and keloids are difficult to treat because of their persistent and recurrent nature. Hypertrophic scars are associated with a better prognosis and tend to improve somewhat with time. Treatments including intralesional corticosteroids and 5-FU, cryotherapy, pressure therapy, silicone gels or sheets, laser therapy, and radiotherapy have all been previously described in the literature12 (see Chapters 10 and 13). However, treatment results are not consistent and frequently disappointing. Furthermore, treatment-related complications such as atrophy and dyspigmentation are especially problematic in skin of color. Ultimately, the selected treatment course depends on a variety of factors such as patient expectations and needs, scar classification, constitutive skin pigmentation, procedural pain, treatment cost, number of visits, and potential downtime and adverse effects, particularly PIH risk in skin of color (Table 18-4). Scar location, functional disturbance resulting from scar contractures, and their overall psychosocial impact are important points to consider so that the treatment objective can match the patients’ expectations (see Chapter 18).
Table 18-4 Factors to be Considered in the Choice of Treatment Modalities
Patients’ expectations regarding treatment endpoints such as cosmetic outcome and symptomatic relief
Psychosocial impact and functional disturbance
Scar types, size, and location
Skin phototypes
Tolerance to procedural discomfort
Estimated number of treatment sessions and duration
Cost and downtime
Adverse effects (e.g., PIH and chance of recurrence)
The application of silicone-based gel sheeting up to 12 hours per day for 2 to 6 months’ duration is a well-established and well-tolerated choice for hypertrophic scars and is used widely in clinical practice for prophylaxis of pathologic scars.20 Although surgical intervention for keloids is tempting, particularly for the seemingly ubiquitous earlobe keloid, surgery should be approached with extreme caution and not without a management plan beginning immediately after surgery. This is due to an extremely high relapse rate of at least 50% after surgical excision and difficulty in predicting the treatment course. Additional management options for keloids, either alone or as adjuncts to surgical excision, include pressure therapy, intralesional corticosteroids and 5-FU, and radiotherapy. In general, multiple treatment sessions and many months, even years, may be required for significant improvements in pathologic scar appearance and symptoms. The treatment aims are cosmetic improvement, relief of symptoms such as pain and itch, and mitigation of scar contractures that limit limb movement. In the experience of the authors, it takes an average of 3 years to achieve treatment goals for pathologic scars on the face. Intralesional corticosteroid plus 5-FU injection every 4 to 6 weeks remains the mainstay of treatment in the early stage. The injection interval can be gradually spaced out to every 2 to 3 months depending on the response. It is more cost-effective to initiate PDL to improve telangiectasias and scar erythema at later stages of management, when the scars are almost flattened. The appearance and texture of scars can then be further improved by fractional laser resurfacing.
Lesional factors affecting the treatment response include the age of the scar, color (hyperpigmentation or hypopigmentation), location, and lesional stability (active growth). In general, younger scars respond better to treatment. Less invasive, safer, and simpler interventions with minimal side effects are generally preferred in ethnic skin. A palliative approach can be adopted with the aim of improving pliability, reducing scar volume, erythema, and dyspigmentation, and to relieve symptoms such as pain and itch. It is also imperative to communicate with the patient adequately to educate them on the course of treatment and the expected response and risk.
Scar origin does not seem to be as important as morphology when developing a treatment plan. The standard treatment for keloids and hypertrophic scars resulting from acne is similar to that of other excessive scarring that results from trauma and surgery. Intralesional corticosteroids decrease collagen synthesis and inhibit fibroblast proliferation.21 PDL therapy has been shown to downregulate the expression of TGF-β and upregulate MMP-13, which results in reduced fibroblast proliferation and collagen type III deposition.22 Laser therapy improves erythema and vascularity as well as scar texture and elevation. Radiotherapy is reserved for recalcitrant keloids; it penetrates into the dermis and inhibits fibroblast proliferation effectively. However, its usefulness is limited by its considerable adverse effects, which include mottled dyspigmentation, radiation dermatitis, and a low risk of carcinogenesis.14 A combination of the various treatment modalities is often adopted to achieve the optimal cosmetic results (see Chapter 16).
Intralesional Injection
Corticosteroids (such as triamcinolone acetonide suspension at doses of 10 to 40 mg per mL) and antitumor agents such as 5-FU and bleomycin can be injected directly into the pathologic scars, either alone or in combination. Hyperpigmentation is a major side effect of intralesional bleomycin in darker skin types, affecting 71.4% of patients in one study.23 Corticosteroids can inhibit TGF-β, can decrease fibroblast proliferation, and have vasoconstrictive effects. Common side effects associated with intralesional corticosteroids include injection site pain, local skin atrophy, telangiectasia, and hypopigmentation. Iatrogenic Cushing’s syndrome following repeated corticosteroid injections for keloids has been reported.24 5-FU, as a potent inhibitor of TGF-β/SMAD signaling, is capable of blocking TGF-β-induced, SMAD-driven upregulation of α2 type I collagen (COL1A2) gene expression in a c-Jun N-terminal kinase (JNK)-dependent manner.25 5-FU is contraindicated in pregnant and pediatric patients. Injections are performed with a 30-gauge needle every 4 to 8 weeks; injection site pain can be ameliorated with a cooling agent or the use of topical anesthesia. Clinical improvement of keloidal and hypertrophic sternotomy scars after treatment with intralesional corticosteroid alone or combined with 5-FU, 5-FU alone, and PDL appeared comparable, though intralesional corticosteroid with or without 5-FU achieved faster resolution and greater improvement of induration of scars than PDL in a randomized controlled study.26 In the experience of the authors, multimodal treatments combining intralesional corticosteroid with 5-FU and laser treatment sessions can reduce the number of treatments to reach treatment goals compared to either modality alone (Table 18-5).
Only gold members can continue reading. Log In or Register to continue