In the United States, Current Procedural Terminology (CPT) codes are used to identify medical procedures, including those that may be appropriate for scar treatment. If an appropriate code is available, such as for an injection, laser, excision, or repair, this should be used.
Often, no specific code exists for a particular scar procedure. In this case, an unlisted procedure code may have to be used in combination with appropriate documentation to support the medical necessity of a procedure, whether before the procedure is performed (preapproval) or after the fact. Code updates are indicated to parallel advances in scar management techniques, such as ablative fractional laser treatment for traumatic scars and contractures with functional and symptomatic sequelae.
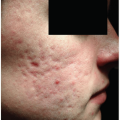
Treatment of some scars may not be considered medically necessary. For instance, atrophic acne scars may be construed as cosmetic in nature by insurers and require out-of-pocket payment by patients seeking treatment.
Apart from acquiring technical skills and honing the clinical decision making required to treat a scar, a physician interested in scar treatment must learn to incorporate scar treatment into his or her practice in a feasible and cost-effective manner. Important pragmatic considerations include: (1) how to defray the costs of scar treatment; (2) how to promote the availability of scar treatment services; and (3) how to ensure efficient throughput of scar patients that reduces utilization of staff, space, equipment, and time.
for completion of the procedure in question. Thereafter, the Centers for Medicare and Medicaid Services (CMS) usually accepts RUC recommendations and uses these to assign a dollar value to the code. The constituents of code value include physician work effort (i.e., the sum of preservice, intraservice, and postservice time, adjusted by the intensity of the effort), practice expense (i.e., the cost of disposable supplies, nonphysician staff time, a small fraction of the cost of durable equipment required, and other space and utilities costs), malpractice expense (i.e., a minute amount that reflects the malpractice risk per procedure), and any additional adjustments that CMS may deem appropriate. The final code values are published by the CMS each year in the Physician Fee Schedule. Private insurers usually use CMS-designated relative values, which they can adjust as they deem appropriate. For instance, a third-party insurer may price most procedures at 80% of Medicare or 120% of Medicare.
Table 25-1 Current CPT and HCPCS Codes That May Be Appropriately or Inappropriately Used for Scar Treatment | ||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
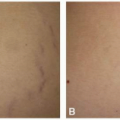
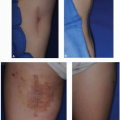
determination of the Medicare contractor operating in a given region may provide additional guidance as to which ICD-10 diagnosis codes may be used with the code group 17106-17018. In general, atrophic scars, like some acne scars, would not meet the proliferation criterion, and treatment of these could not be described by these codes. Treatment of redness in a scar associated with prior surgery or previous laser treatment to treat a congenital malformation would be covered since the underlying disease process is covered.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


