Atrophic scars are caused by a variety of inflammatory, infectious, traumatic, and individual genetic risk factors, in addition to mechanical skin stretching.
Acne is a common disorder with a high prevalence among adolescents, and it often results in atrophic scars.
The disfigurement from acne scarring is associated with considerable psychological distress including poor self-esteem, embarrassment, depression, anxiety, and anger. These issues may place limitations on social interactions, daily activities, and employment.
Levels of psychosocial distress may not be accurately predicted by one’s degree of disfigurement.
Multimodal treatment regimens that combine medical, injectable, surgical, and device-based therapies are most advantageous in the treatment of atrophic acne scarring.
Although striae distensae do not pose a health risk and are not associated with as severe psychosocial dysfunction as acne scars, they can burn, itch, and cause emotional stress.
Multiple treatment modalities for striae distensae have been published, yet no first-line ideal therapy has emerged.
The efficacy of multimodal regimens (“mega-combinations”) is gaining popularity and is likely the future of treating atrophic scars.
in recent years. Striae can be considered a form of atrophic scarring, resulting from various mechanisms of skin stretching. Millions of people are affected and bothered by this common condition and may seek evaluation and a discussion of treatment options.
have a substantial negative impact on the overall social and functional well-being of affected individuals. In their study, an overwhelming 85.4% of subjects revealed they were unhappy looking at themselves in the mirror, with 84.4% feeling less attractive owing to their acne scars.
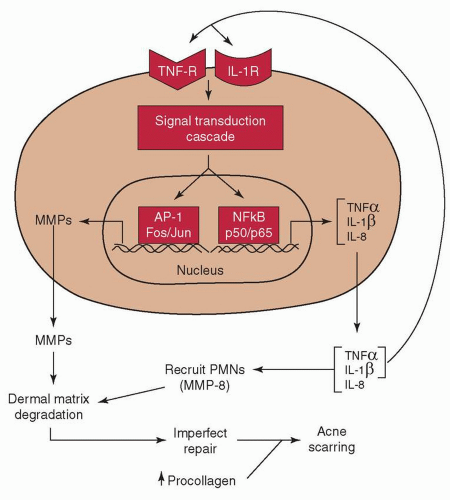 FIGURE 17-1 Hypothetical model of the pathophysiology of inflammatory acne and dermal damage. In inflammatory acne lesions, NF-κB signaling is activated. As a consequence, NF-κB-driven inflammatory cytokine genes (e.g., TNF-α and IL-1β) are induced. These primary cytokines will propagate the inflammatory response by acting on endothelial cells to elaborate adhesion molecules (eg, ICAM-1) to facilitate recruitment of inflammatory cells into the skin. TNF-α and IL-1β will also stimulate the production of secondary cytokines, such as IL-8, which can aid in chemotaxis of inflammatory cells. By working through their cell surface receptors, TNF-α and IL-1β not only amplify the NF-κB signaling cascade, but also activate MAP kinases to stimulate AP-1-mediated gene transcription. As a consequence of AP-1 activation (cJun induction), AP-1-driven MMPs are elaborated by resident skin cells. Along with MMP-8 and neutrophil elastase brought in by PMNs, they degrade the matrix. This is followed by matrix synthesis and repair, which is imperfect. Most of the imperfections would leave clinically undetectable deficits in the organization or composition, or both, of the extracellular matrix. However, when they occur to a significant extent throughout time, accompanied by sustained procollagen synthesis, acne scarring becomes clinically visible. (Used with permission from Kang S, Cho S, Chung JH, et al. Inflammation and extracellular matrix degradation mediated by activated transcription factors nuclear factor-kappaB and activator protein-1 in inflammatory acne lesions in vivo. Am J Pathol. 2005;166:1691-1699.) |
In other words, treatment of acne scars must be individually directed for each patient depending on the size, type, and severity of scars present.23 The anatomic location of the scar and the patient’s skin type may also be important considerations. Clinicians may encounter scars with more than one physical characteristic, such as pigmentation or erythema, in addition to being atrophic or hypertrophic. These may be termed “hybrid” scars.4 Various modalities, single or combined, have been used to treat acne scars. Limited efficacy and problematic side effects have made the gold standard or “home-run” treatments challenging to determine.
Table 17-1 Classification of Acne Scars | ||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||
Table 17-2 Most Common Treatment Modalities Based on Scar Type | ||||||
|---|---|---|---|---|---|---|
| ||||||
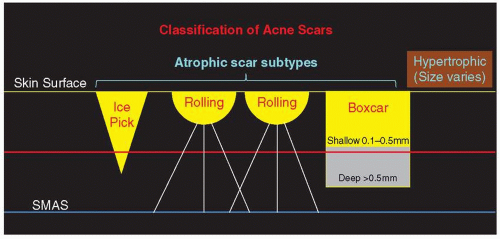 FIGURE 17-2 Classification of acne scars. Yellow line represents skin surface. Yellow/gray-shaded areas within scar subtypes represent loss of tissue. Brown-shaded area represents gain of tissue. Red line roughly denotes depth of ablation and resurfacing capability of the CO2 laser. Blue line represents SMAS to which fibrous bands (white lines) adhere, creating rolling scars. (Adapted by Dr. Joanna G. Bolton from Jacob CI, Dover JS, Kaminer MS. Acne scarring: a classification system and review of treatment options. J Am Acad Dermatol. 2001;45:109-117.) |
Table 17-3 Main Causes and Risk Factors for Developing Atrophic Scars | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||
shallow (0.1 to 0.5 mm) or deep (>0.5 mm). Shallow boxcar scars are within reach of most resurfacing treatments, but deeper boxcar scars and the tip of the infundibulum of ice pick scars are resistant to improvement in the absence of full-thickness treatment of the scar.
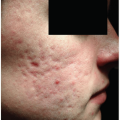
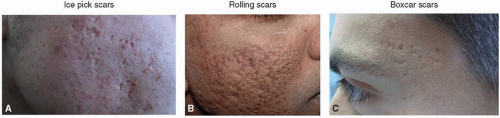 FIGURE 17-3 Atrophic acne scars. A: Ice pick, B: rolling and boxcar, C: boxcar. All three subcategories can be deep and coexist, making a singular clinical identification difficult. (Photo permission granted for (B) by Dr. Mitchel P. Goldman, MD; (A, C) Copyright © 2010 Gabriella Fabbrocini et al.) |
Table 17-4 Goodman and Baron Qualitative Grading Scale of Postacne Scarring | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||
different grades to identify the level of postacne scarring. In those affected with mild acne, the pattern and grading is often easy to assess. However, in severe cases, different patterns are simultaneously present and may be difficult to differentiate. Their quantitative global postacne scarring assessment tool30 is a more complex grading pattern that assigns scores on the basis of the type of scar and the number of scars present.
Table 17-5 Pros and Cons of the Most Common Treatment Modalities for Atrophic Scars | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||
Stressing postprocedure aftercare regimens, expected healing times, unpredictability with any intervention, and emphasizing the need for multiple treatment sessions spaced over many months to achieve desired appearance is essential. “Under promise, over deliver” results is a good rule of thumb.
Table 17-6 Hierarchy of Therapy for Atrophic Acne Scars, in Descending Order of Efficacy | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
mandatory. Additionally, superficial peeling agents include Jessner solution and low-concentration (10% to 30%) TCA. Similar to light glycolic peels, they affect only the epidermis when applied correctly and are best utilized to treat only the most superficial acne scars and PIH.
Table 17-7 Classification of Peeling Agents | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
 FIGURE 17-4 Patient after two coats of 30% trichloroacetic acid (TCA) with a dense white frost representing keratocoagulation. (Photo permission granted by Joseph Niamtu, DMD.) |
to 70% or more after three to six treatments at intervals of 2 to 4 weeks.51,52 Patient satisfaction was rated higher with 100% TCA versus a 65% concentration, at 94% satisfaction versus 82%, respectively, in the study by Lee et al.52 However, Fabbrocini et al.49 have shown that a lower TCA concentration (50%) has similar results with fewer adverse reactions. The CROSS technique has also been successful in the treatment of atrophic postvaricella (chickenpox) scarring, with over 80% of patients demonstrating moderate to marked improvement following six treatments with 70% TCA.53
 FIGURE 17-5 Acne scarring with PIH treated with a commercially available acid peel (before and after four Vi Peel treatments and a proprietary topical regimen including bleaching cream). (Photo permission granted by Melissa McGuire, Vi Aesthetics.) |
 FIGURE 17-6 CROSS technique (chemical reconstruction of skin scars), or dot peeling, using a high-strength TCA (65% to 100%) has been found to be a useful solo or adjunctive treatment for ice pick and small boxcar scars. (Photo permission granted by Joanna G. Bolton, MD.) |
hypertrophic scarring has been reported to be a potential risk, first noted in patients undergoing dermabrasion following a recent course of oral isotretinoin therapy. This complication originally prompted the recommendation to wait 6 to 12 months for scar revision following isotretinoin use.33,63 Despite this recommendation, there are reports of patients undergoing dermabrasion with concurrent or recent isotretinoin therapy without hypertrophic scar formation and research is ongoing.64
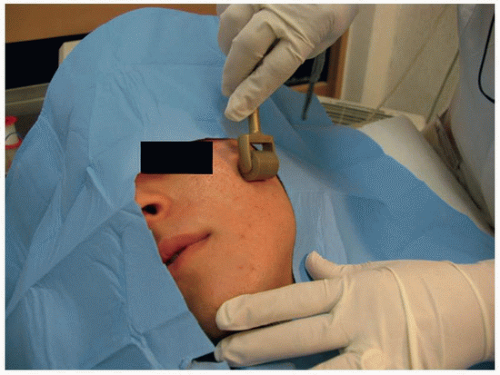 FIGURE 17-7 Needling procedure utilizing a sterile roller comprising hundreds of fine, sharp needles to puncture the skin 1.5 to 2 mm (level of mid-dermis). (Copyright © 2010 Gabriella Fabbrocini et al.) |
 FIGURE 17-8 A: Schematic depicting subcision. A regular lumen, 18G, 11/2-inch hypodermic needle or a triangular, solid-tipped Nokor Admix needle (inset photo; Becton Dickinson and Co, Franklin Lakes, NJ) may be used to undermine and separate fibrous bands (white bands). Nokor needle photo is for illustration only – the level of treatment should remain above the SMAS. (Adapted by Dr. Joanna G. Bolton from Jacob CI, Dover JS, Kaminer MS. Acne scarring: a classification system and review of treatment options. J Am Acad Dermatol. 2001;45:109-117.) B: Subcision technique with Nokor needle inserted intradermally and being used to undermine a bound-down scar. Scars identified for treatment are marked preprocedure with blue ink. Piston-like motion used to release the fibrous bands; the skin is elevated to improve traction, facilitate needle motion, and avoid underlying structures. The needle may be placed on a 3-mL syringe for easier gripping and better leverage. (Photo permission granted by Joanna G. Bolton, MD.) |
treated with the CROSS technique, punch techniques, and radiofrequency treatments. Shallow boxcar scars have been successfully treated with ablative and nonablative fractionated lasers in addition to subcision, dermal fillers, skin needling, radiofrequency, and/or other surgical corrections such as excision and closure, rhytidectomy, and punch-grafting techniques. Deeper boxcar scars are better treated with punch-grafting or excisional techniques and/or radiofrequency devices. Rolling acne scars have been treated with ablative and nonablative fractionated lasers in addition to dermal fillers, dermabrasion, subcision, skin needling, and/or radiofrequency devices. Hypertrophic and keloidal scars are better treated with the 585-to-595-nm PDL, 515-to-1,100-nm IPL, and ablative fractionated lasers with or without the addition of intralesional corticosteroids and/or 5% 5-fluorouracil because of the potential for a worsening of these lesions with other modalities.73 Table 17-8 summarizes various laser treatment modalities (see Chapter 13).
Table 17-8 Laser Treatment of Acne Scars | ||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


