Scars and Scar Management: Ethical Considerations
Baddr A. Shakhsheer
Puneet Singh
Lawrence J. Gottlieb
Peter Angelos
Mark Siegler
KEY POINTS
The patient perspective directs the management of scars.
Expectations of patient and surgeon need to be concordant before any intervention to improve a scar is initiated.
Decisions about scar management require a shared decision-making approach in which the physician provides judgment, technical guidance, and expertise and patients express their values and preferences.
A broad array of scars and deformities exist, congenital and acquired, with a spectrum of perception of severity. Ethical issues relating to the treatment of scars may be specific to the circumstances of the scar.
In Nathaniel Hawthorne’s story The Birthmark, an esteemed philosopher and scientist marries a beautiful woman who is aesthetically perfect save for a small red birthmark on her cheek.1 He becomes progressively obsessed with this imperfection and seeks to develop a potion to rid his wife of the “frightful object.” The potion succeeds in removing the birthmark but she dies as a side effect of the treatment. Renowned ethicist Leon Kass used this vignette to open the 2002 President’s Council on Bioethics as a prelude to discussing the effects and consequences of biomedical innovations and intervention.2 Hawthorne’s story raises many issues that are relevant to the topic of deformities, one principal issue of which is the benefit-risk ratio of treating such deformities, either congenital ones as in The Birthmark or acquired ones, such as scars after a surgical procedure.
Scars exert far greater effect than simply their physiologic consequences. One need not venture past the popular literature to find examples of this sentiment. Nora Ephron writes in her book I Feel Bad About My Neck: “If you learn nothing else from reading this essay, dear reader, learn this: Never have an operation on any part of your body without asking a plastic surgeon to come stand by in the operating room and keep an eye out. Because even if you are being operated on for something serious or potentially serious, even if you honestly believe that your health is more important than vanity, even if you wake up in the hospital room thrilled beyond imagining that it wasn’t cancer, even if you feel elated, grateful to be alive, full of blinding insight about what’s important and what’s not, even if you vow to be eternally joyful about being on the planet Earth and promise never to complain about anything ever again, I promise you that one day soon, sooner than you can imagine, you will look in the mirror and think, I hate this scar.”3
Ethics underlies all medical practice and plays a fundamental role in decision-making in health care. Without ethics, medicine would be a “disembodied” discipline, one that would not consider the importance of the patient, his or her goals, and the broader meaning of the interventions that are performed.4 This chapter will discuss ethical principles and tenets related to the management of scars, including congenital and iatrogenically acquired scars, with the goal of providing a framework for pertinent decision-making in the field of scar management.
Medicine and Ethics
Clinical Medical Ethics
The ethics of medicine and the interaction between physicians and patients has been of interest since the Hippocratic Oath in the 5th century bc. The “first do no harm” ethos is found in the Hippocratic writing Epidemics, Book I, and forms the historical impetus for contemporary medical ethics, based on the four principles of beneficence, nonmaleficence, respect for autonomy, and justice.5 Beneficence means that practitioners should always work in the best interest of the patient. Nonmaleficence is a modern statement of the “first do no harm” principle. Respect for autonomy mandates that the patient has the right to choose or refuse treatment and holds primary responsibility in decision-making for
medical treatment. In other words, autonomy recognizes the patient’s right to self-determination. The principle of justice concerns itself with fairness and equality and the elimination of disparity in health care and health.
medical treatment. In other words, autonomy recognizes the patient’s right to self-determination. The principle of justice concerns itself with fairness and equality and the elimination of disparity in health care and health.
A well-regarded contemporary approach to assessing clinical ethical issues is Jonsen, Siegler, and Winslade’s use of four different categories to analyze the issues: medical indications, patient preferences, quality of life, and contextual features.6,7 Medical indications refer to the clinical facts of the medical situation and the goals of treatment. Patient preferences relate to the principle of respect for autonomy: has the patient been informed about the appropriate risks and benefits and have any choices or predilections been expressed? Quality of life explores the probable future of a patient, with or without treatment. Under this heading, the risks, benefits, and potential side effects are weighed in order to ascertain potential medical outcome. The contextual features category examines issues of justice, fairness, and disparities, for instance, whether there are entities outside of the physician and the patient that may be affected, including family members, the health care organization, or society at large (Fig. 4-1).
Surgical Ethics
Surgical ethics represents a subset of medical ethics specific to surgeons and other proceduralists.8 One of the original goals of the American College of Surgeons upon its founding in 1913 was to eliminate unethical practices in surgery, particularly fee-splitting, itinerant surgical procedures, and the practice of performing surgery at a distance from one’s local hospital and practice, which left the postoperative care to local physicians.
The practice of surgery and of other invasive procedures poses a direct challenge to the ancient doctrine of “do no harm” (i.e., nonmaleficence). Modern commentators have agreed that the “do no harm” rule is not an absolute prohibition. Rather, “do no harm” is a caution for physicians to balance the benefits of their interventions with the likelihood of bad effects or harms. The development of iatrogenic scars after surgical procedures is a prime example for the need for this benefit-harm balancing test.
On a daily basis, surgeons shoulder heavy responsibility. Because of the trust engendered in the surgeon-patient relationship, the surgeon feels a strong sense of personal responsibility for patient outcomes.9 Frequently, they perform invasive procedures with high levels of associated risk, adding further complexity to the practice of surgery and surgical ethics.10 In addition to invasive procedures, which may be performed when the patient is anesthetized and thus incapacitated, surgeons must adequately obtain informed consent, deliver bad news, and address end-of-life issues.11 In the case of emergency surgeries, this relationship must be established quickly and under pressure, as the proceduralist must ascertain the patient’s values in a brief time period and act upon those values while a patient is potentially incapacitated by anesthesia.
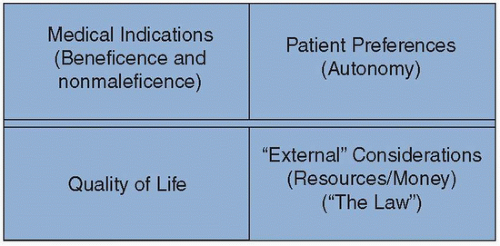 FIGURE 4-1 The four-box model, providing a structured approach to ethical and clinical decision-making. (Adapted from Jonsen AR, Siegler M, Winslade WJ. Clinical Ethics: A Practical Approach to Ethical Decisions in Clinical Medicine. 8th ed. New York, NY: McGraw Hill Medical; 2015.) |
Further, the everyday, frequent potential for surgical innovation at the operating table distinguishes surgical ethics from the general field of clinical medical ethics.12 For instance, in the early history of organ transplantation, patients were often harmed by the procedure. Laparoscopy and minimally invasive techniques in surgery were adopted widely in the absence of clinical trials because of patient demand after reports of decreased pain and shorter length of stay, even though early assessments on the novel techniques showed significantly increased complication rates.13 Thus surgical ethics is a unique subset of clinical medical ethics, set apart by a distinct set of questions and by situations that distinguish them from the larger field of clinical ethics.
Ethical Questions Specific to Scar Treatment
Medical Indications
What Is a Scar?
A scar generally forms as the body attempts to heal a wound. It is the natural endpoint of inflammation and subsequent fibrosis. Scars can result from trauma, infection, and certain diseases as well as from iatrogenic causes.
What Is Normal?
“As I contend that the desire for the normal is a powerful one, not easily swayed by a rational weighing of costs and benefits, I believe it is important to consider what means there are to satisfy that desire without necessarily acquiescing to the norm implied in the standard of normal.”14 It is also important to remember that the concept of “normalcy” is crucial to patients, especially ones with scars. This concept ought to be explicitly discussed and the possible outcomes explicitly conveyed. Thus we may consider that when a patient presents for consultation for improvement of an unsightly scar, the surgeon is generally thinking of how they may improve the scar or deformity. By contrast, the patient’s goals are frequently to erase the scar and return to the preinjury state, and so, it is imperative that the surgeon’s expectations be concordant with that of the patient’s. We must recognize that what is “normal” or “acceptable” is often determined by the perception of the patient, a concept that conforms to the ethical principle of autonomy. For example, a military patient may wear a scar as a badge of honor or a reminder of bodily sacrifice. However, a victim of domestic abuse will likely have very negative feelings associated with his or her scars. A patient
may consider any skin scarring “abnormal.” Even a scar that is not visible may cause itching or pain and thus be considered “abnormal” by the patient. These differences contribute to the difficulty in managing scars as well as the difficulty in justifying compensation for these procedures from outside parties such as insurance companies.
may consider any skin scarring “abnormal.” Even a scar that is not visible may cause itching or pain and thus be considered “abnormal” by the patient. These differences contribute to the difficulty in managing scars as well as the difficulty in justifying compensation for these procedures from outside parties such as insurance companies.
What is “normal” can vary not only from person to person but geographically and culturally as well. For instance, in Nigeria, pediatric umbilical hernias are nearly ubiquitous. Anecdotal reports exist of Nigerian mothers bringing their children to medical centers because they did not have an umbilical hernia.15 In some cultures, an umbilical hernia is seen as a sign of beauty.16 Certain tribal cultures of eastern Africa have embraced and indeed celebrated their tendency to heal with hypertrophic scars and keloids by purposeful injury and scarification to produce decorative scarring, which has not only become the social norm but imparts social status.
Further, the implications of deviation from normal can be different culturally and geographically. Take Nora Ephron’s example from this chapter’s opening: a scar after a thyroidectomy is in a cosmetically sensitive anatomic location in the United States. However, in places such as Korea and Japan, this neck scar holds an even greater impact with a severe social stigma.17 This has led Southeast Asian surgeons to develop innovative techniques for thyroidectomy, including using trans-axillary incisions to reach the neck. These techniques, however, are recognized to carry greater risk.
In describing the risk and benefits of altering the technique of a surgical procedure with the goal of a less noticeable scar, it is ethically imperative that surgeons present not only the benefit of reducing scars, but also the increased risk of scars from the procedure. Surgeons are well trained in assessing different risks for the same procedure based on ethnicity, skin type, incision location and direction, history, duration of symptoms, and comorbidities. However, physicians must also recognize that the same procedure may carry different benefits for individual patients. For instance, a fashion model may elect to have her gallbladder removed using natural orifice techniques to avoid the scars, even when informed that the novel technique is less well understood in terms of complications when compared with traditional gallbladder removal.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


