Sternal Wound Infection
Description
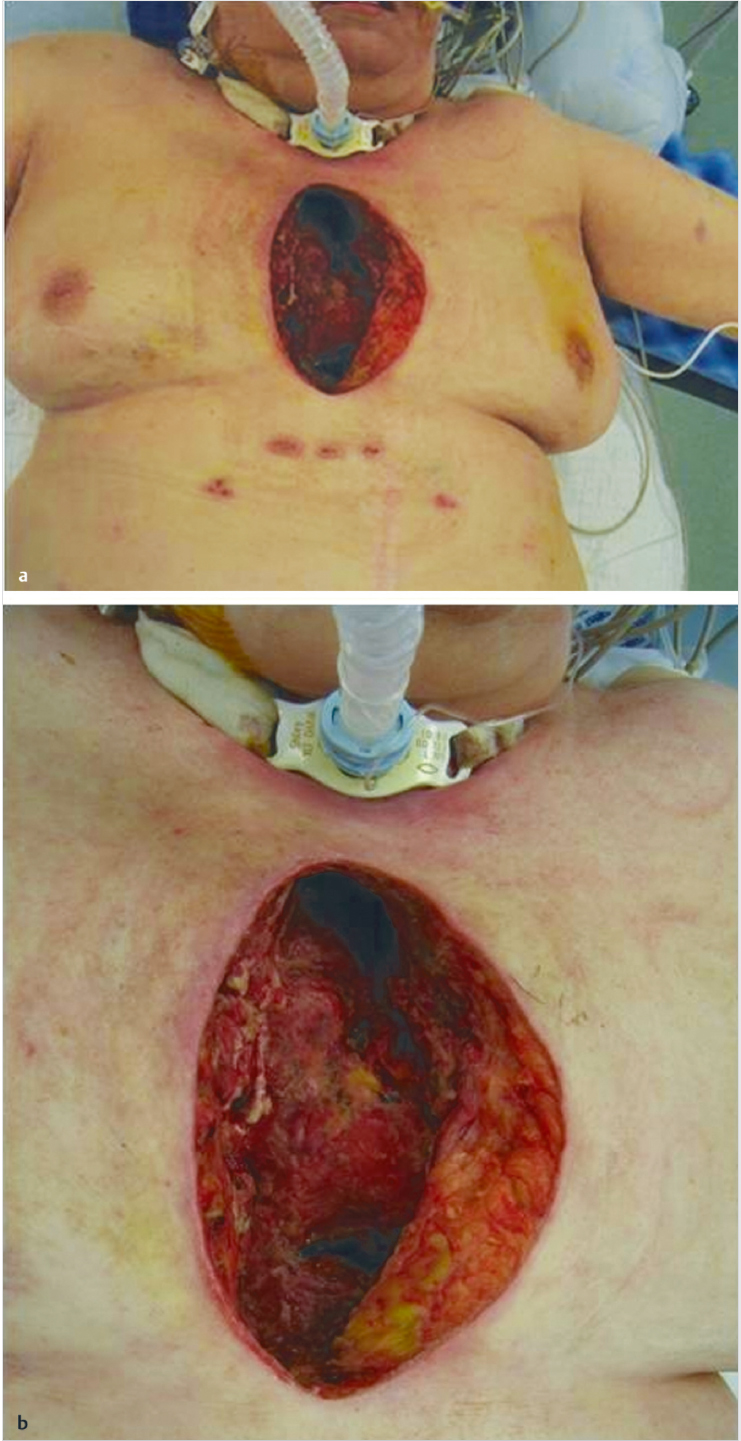
Patient with evidence of an anterior midline chest wall wound measuring roughly 15 × 8 cm.
The sternal edges and mediastinum are exposed without evidence of gross purulence or extensive necrotic tissue.
No vascular grafts are visible.
Work-up
History
Etiology: Sternal wound infection (following median sternotomy), tumor resection, radiation (ulcers, osteoradionecrosis).
Duration of wound.
Current wound care.
Comorbidities: Respiratory insufficiency, sepsis, cardiac disease.
Review previous operative reports (e.g., vessels used, ribs resected).
Physical examination
Vital signs: Is the patient stable?
Size and depth of defect.
Presence of infected or necrotic tissue.
Exposed grafts, vascular devices, or mediastinum.
Prior surgical scars on chest or abdomen.
Congenital abnormalities: Poland syndrome, pectus excavatum/carinatum.
Pertinent imaging or diagnostic studies
Chest X-ray: Presence of sternal wires and evaluation of lung fields.
Computed tomography: Evaluation for deep abscesses if persistent fevers and sepsis.
Magnetic resonance imaging: Most useful in chronic sternal defects for evaluation of extent of infection and/or osteomyelitis.
Angiography: Allows study of available vessels and their patency.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


