Ischial Pressure Sores

Description
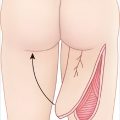
Stage IV ischial pressure ulcer with exposed bone and fibrinous slough.
Work-up
Clean, pink granulation tissue at wound base with no evidence of gross contamination.
Multiple scars indicative of prior surgical management with likely posterior thigh and gluteal rotation flaps.
History
Risk factor assessment: Age, nutritional status, comorbid conditions (diabetes, vascular disease), ambulatory status, spinal cord injury, spasm and previous treatment, continence (urine and fecal), tobacco and substance abuse, presence of shear forces, mental status
Support network
For treatment and continued care.
Home environment and any pressure-reducing devices.
Current wound and skin care regimens.
Previous wounds and interventions.
History of current wound: Duration, previous infection, changes in size.
Physical examination
Location and dimensions of wound, quality of surrounding tissues, focused sensory examination.
Presence of spasm, moisture, soilage.
Evidence of infection.
Pressure ulcer staging (Table 31.1).
Pertinent imaging or diagnostic studies
Laboratory tests: Complete blood count (CBC), complete electrolyte panel, albumin/prealbumin, hemoglobin A1C, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP).
Magnetic resonance (MR) imaging: Osteomyelitis is suggested by the presence of T2 hyperintensity and low intensity on T1 images; sensitive and specific for osteomyelitis.
Tissue biopsy: For pathology in chronic wounds and for culture.
Bone biopsy may be useful to rule out osteomyelitis, especially if suggested on MR imaging.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


