Case 1
Clinical Presentation
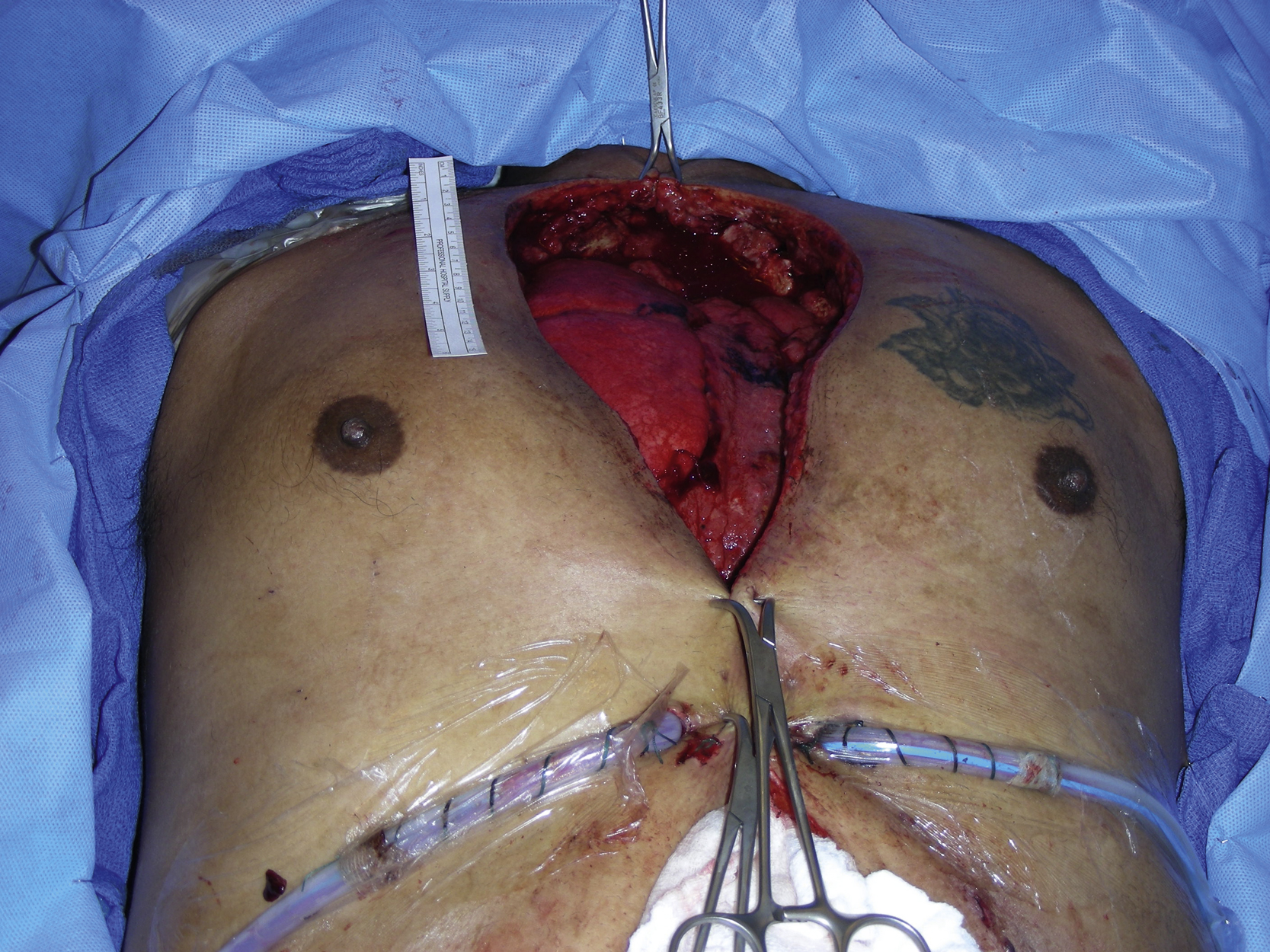
A 72-year-old Iranian male with multiple medical problems, including coronary artery disease, severe aortic valve stenosis, chronic occlusive pulmonary disease, and congestive heart failure, underwent coronary artery bypass grafting and aortic valve replacement as part of the preparation for a total gastrectomy because of a newly diagnosed large gastric carcinoma. He had a complicated postoperative course with prolonged treatment in the intensive care unit. He developed a dehiscence of the lower sternal wound and was urgently taken to the operating room by the cardiothoracic service for sternal wound debridement ( Fig. 21.1 ). All wires were removed during the initial debridement. The plastic surgery service was asked to provide soft tissue coverage to his sternal wound.

Operative Plan and Special Considerations
Additional more aggressive debridement should be performed first to control local infection and good sternal soft tissue condition. The goal of reconstruction would include obliteration of the sternal dead space with a well-vascularized tissue and the sternal wound closure. Bilateral pectoral major myocutaneous advancement flaps are a good option for this kind of sternal reconstruction. Each side of the pectoral major myocutaneous flap can be elevated individually and advanced toward the midline of the sternal wound so that the sternal soft tissue wound can be approximated without tension. The anterior rectus sheath can also be elevated with each side of the pectoral major muscle to provide additional tissue coverage for better lower sternal wound closure. Such combined bilateral flap reconstructions provide a durable soft tissue reconstruction for the sternal region with maximal obliteration of the underlying sternal dead space.
Operative Procedures
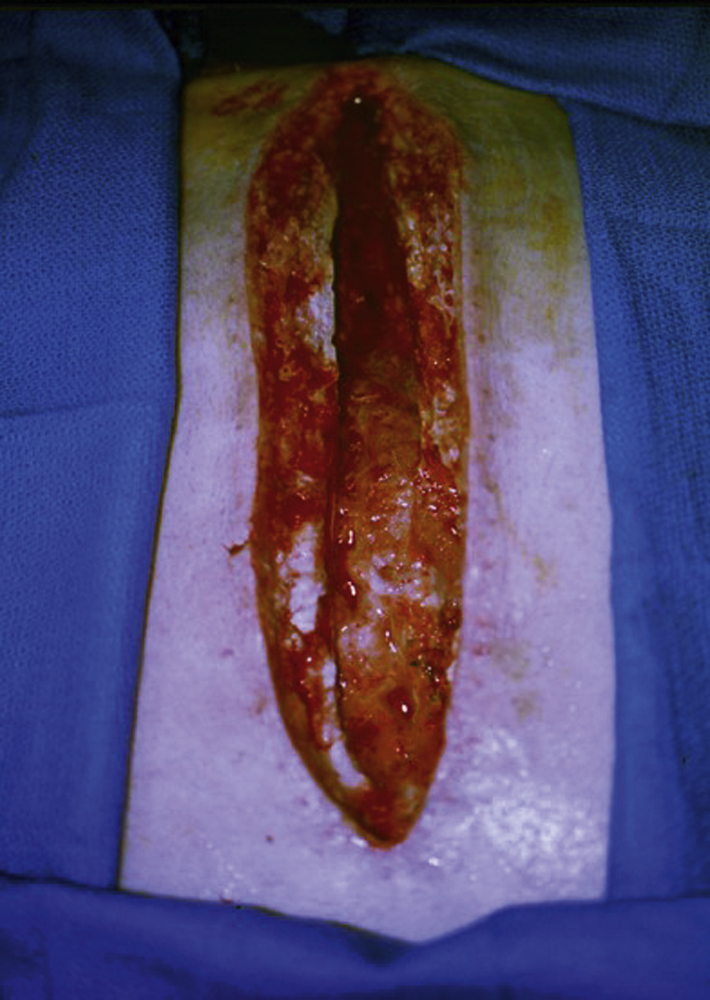
Under general anesthesia with the patient in a supine position, additional aggressive bony and soft tissue debridement was performed by both the cardiothoracic surgery service and the plastic surgery service. The wound was irrigated with warm antibiotic solution. At completion of the additional wound debridement, all wound edges appeared to be fresh and healthy ( Fig. 21.2 ).
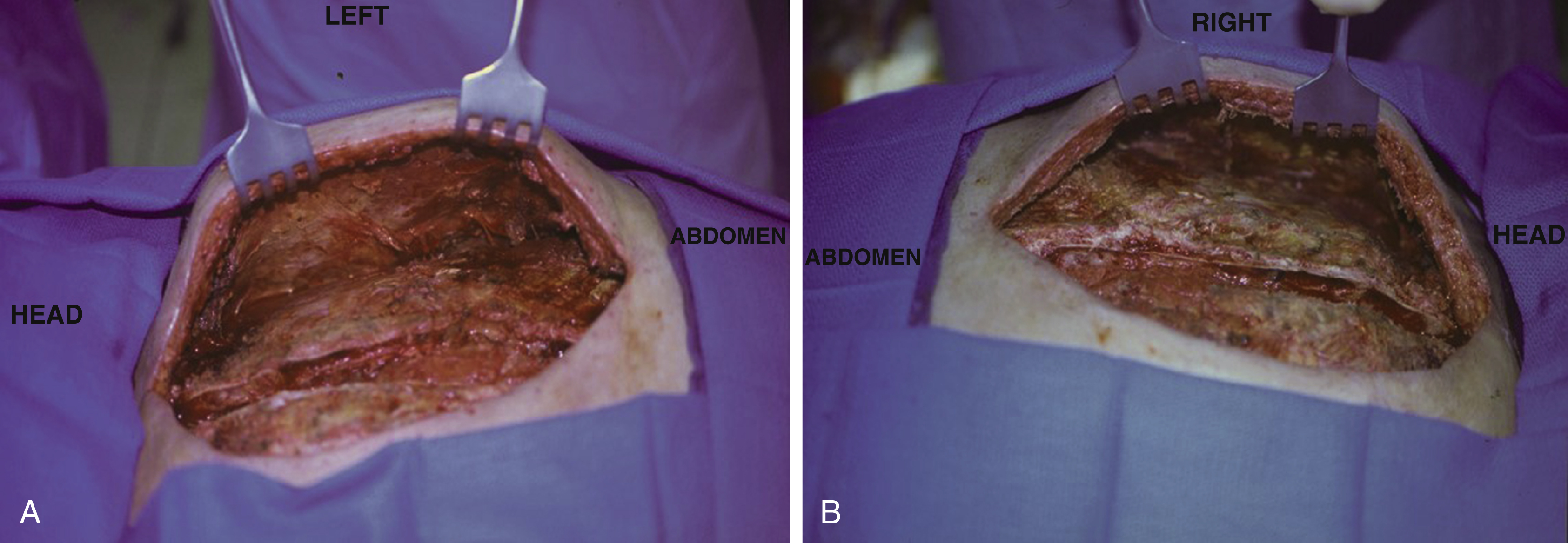
The left pectoral major myocutaneous flap was elevated first. Under direct vision, the flap was elevated from the chest wall as a single unit. The submuscular space was entered and dissection was carried out in this tissue plane with the aid of a mammary light retractor. The flap dissection was performed toward the anterior axillary line and the lateral board of the muscle was released. Inferiorly, the muscle was elevated in conjunction with the anterior rectus sheath. The entire flap could easily be advanced across the midline of the sternal wound and the flap dissection was completed ( Fig. 21.3A ). The right pectoral major myocutaneous flap was dissected in the same way ( Fig. 21.3B ).
Both flaps were advanced and approximated in the midline of the sternal wound and final closure was performed in three layers after hemostasis and placement of a drain under each muscle flap. The muscle layer was approximated with interrupted 2-0 PDS sutures. The deep dermal layer was approximated with interrupted 3-0 Monocryl sutures. The skin closure was performed with skin staples ( Fig. 21.4 ).

Follow-Up Results
The patient had a slow recovery with a complicated postoperative course. His sternal wound eventually healed well without any major issues related to the sternal wound reconstruction. He was discharged from the hospital 49 days after the open-heart surgery and 26 days after the sternal flap reconstruction. The drain was removed about 3 weeks after the sternal wound closure ( Fig. 21.5 ).

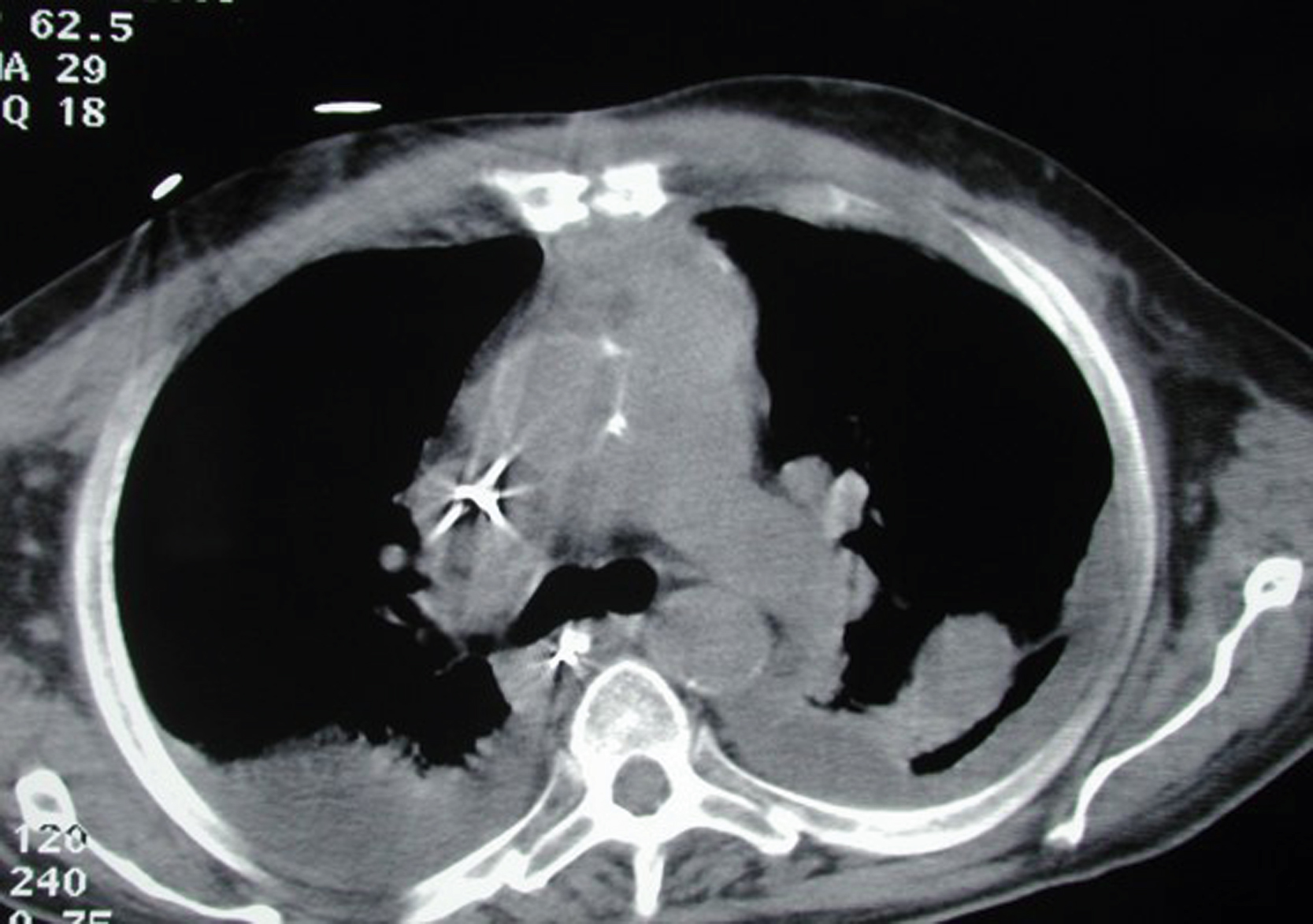
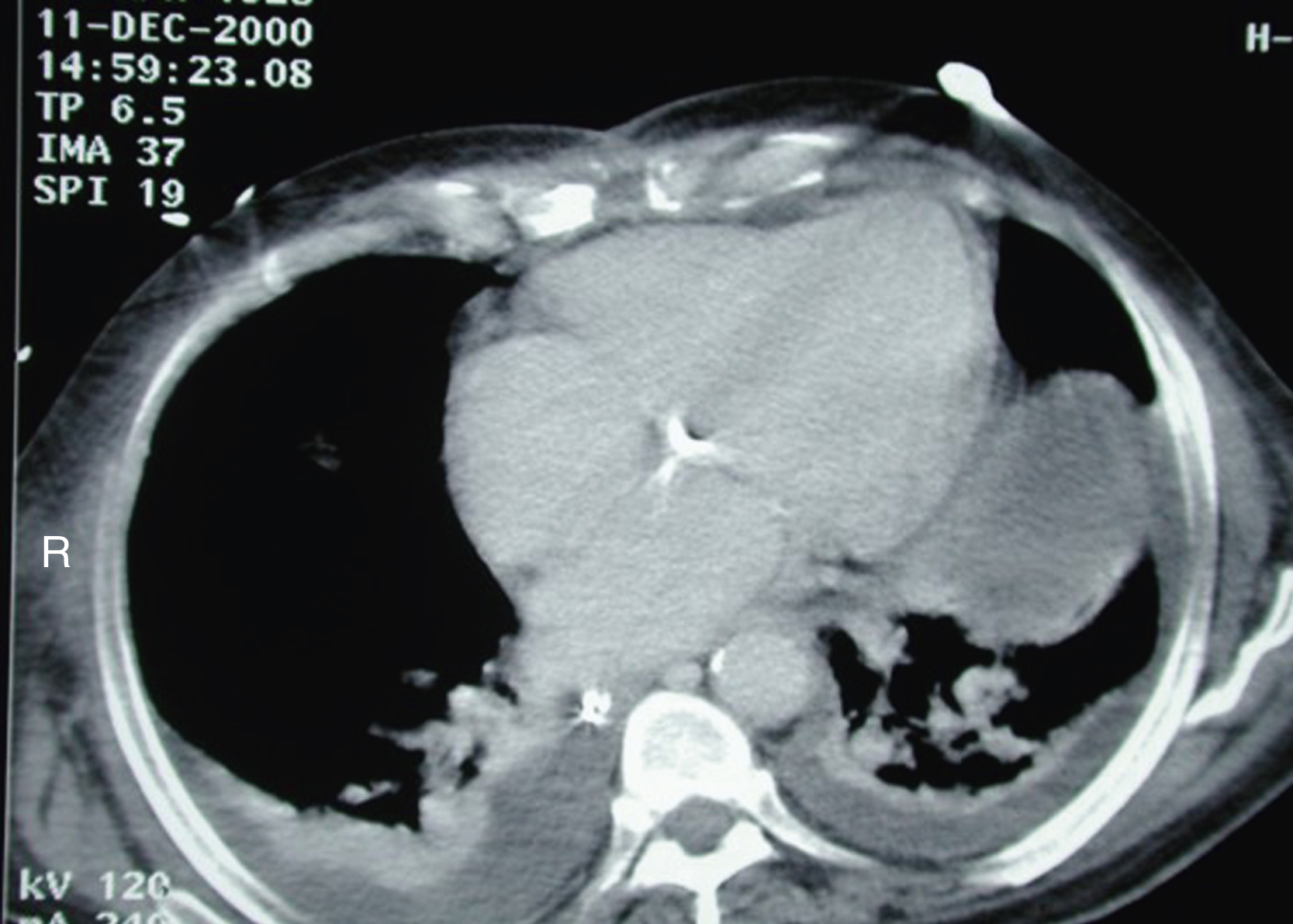
The patient was readmitted to the hospital 1 month later and a total gastrectomy with a Roux-en-Y esophageal jejunostomy and feeding jejunostomy was performed by the surgical oncology service. His postoperative course was complicated by prosthetic valve bacterial endocarditis, sepsis, and multisystem organ failure. He was also found to have a seroma under the intact closure of the upper sternal flap reconstruction ( Fig. 21.6 ). The sternal flap site was stable and there was no cellulitis. The etiology of this fluid collection was thought to be an infiltration after a central line placement. Approximately 100 cc of cloudy fluid was aspirated and a pressure dressing was applied to the sternal area. The final culture showed Candida albicans . Follow-up chest CT scans showed a healed sternal soft tissue closure with no substernal fluid collection ( Figs. 21.7 and 21.8 ).


Final Outcome
The patient had a well-healed sternal wound after bilateral pectoral major myocutaneous advancement flap reconstructions for sternal wound dehiscence ( Fig. 21.9 ). His postoperative course after total gastrectomy was complicated by prosthetic valve endocarditis, sepsis, and multisystem organ failure. He eventually died 2 months after the total gastrectomy.
Pearls for Success
Bilateral pectoral major myocutaneous advancement flaps are a good option for closure of a sternal wound. In general, the amount of the sternal bony defect after debridement does not warrant a rigid reconstruction and the potential dead space would need attention for soft tissue filling in addition to a reliable soft tissue wound closure. The pectoral major myocutaneous flap can be elevated as a single unit and both flaps can be approximated in the midline of the anterior chest in three layers, including the pectoral major muscle from each side. This option can be an excellent choice to fill the defect and obliterate the dead space and can provide a durable soft tissue reconstruction. Each flap can be elevated through the existing sternal wound. Once the lateral and inferior attachments of the pectoral major muscle are released, each flap can be advanced to the midline of the anterior chest without difficulty. If needed, the anterior rectus fascia can be incorporated with the inferior portion of the pectoral major muscle. During the flap dissection, the thoracoacromial vessels should be visualized and protected. Seroma under the lower third of the flap closure can occur and can be managed with needle aspiration. If more bony debridement in the lower sternum is anticipated, the right rectus abdominis muscle turnover flap may be added to provide better obliteration of the dead space in the area because the internal mammary vessels are usually intact on that side.
Case 2
Clinical Presentation
A 43-year-old incarcerated male developed an infection of his sternum caused by coccidioidomycosis. This was widely debrided by the cardiothoracic service to remove all infected tissues. He was left with a large sternal defect, measuring 20 × 12 cm, with exposed right lung and mediastinal structures ( Figs. 21.10 and 21.11 ). The patient remained hemodynamically stable once his systemic infection was under control. The plastic surgery service was asked to close the defect in conjunction with further surgical debridement by the primary service.