Clinical Presentation
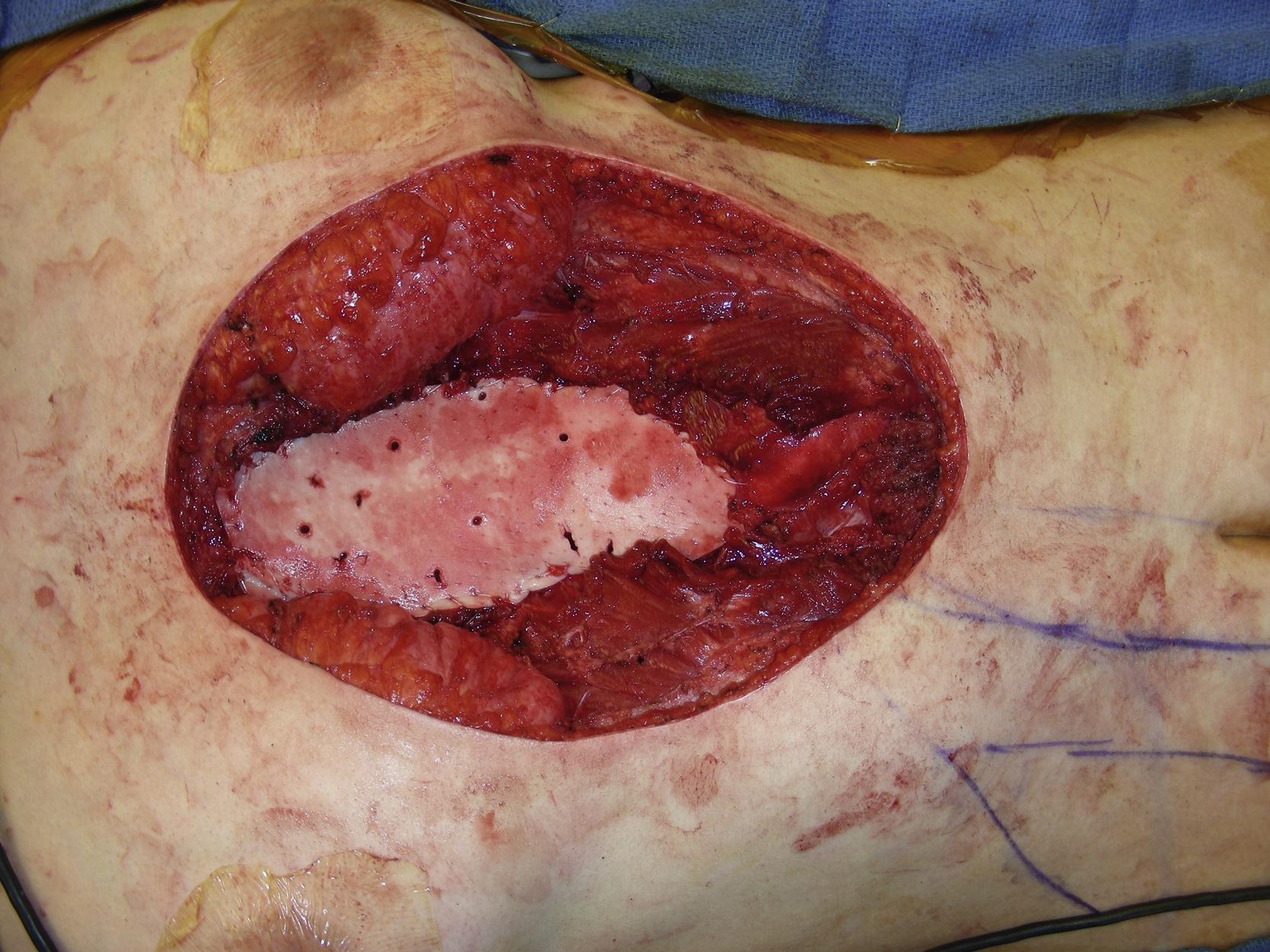
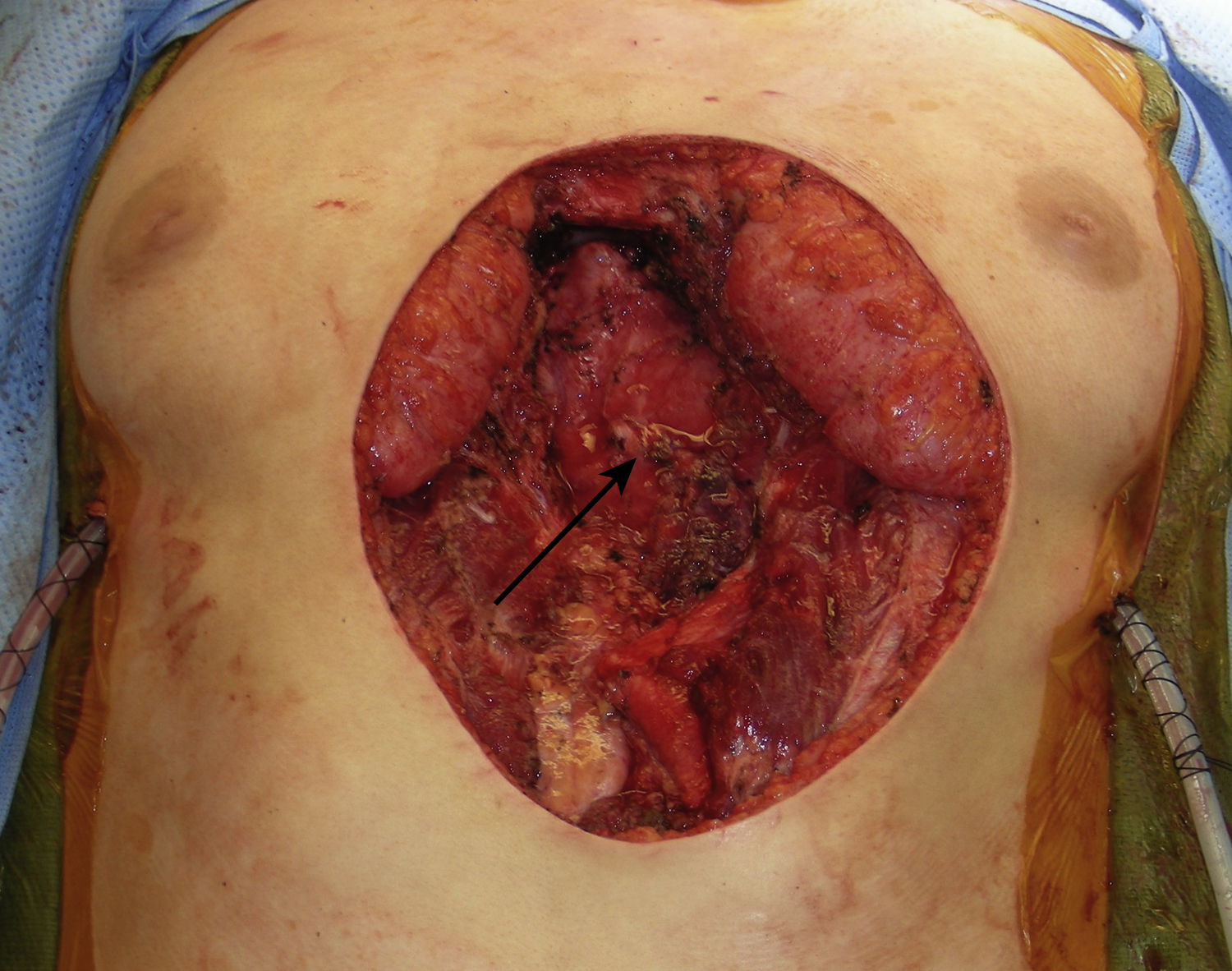
A 19-year-old White female had a large soft tissue mass in her lower chest and sternal area. Preoperative biopsy showed desmoid type of fibromatosis. She underwent resection of this soft tissue mass by the pediatric cardiothoracic surgery service and the plastic surgery service was asked to provide lower chest wall reconstruction after the tumor resection. After resection, the entire skin defect of the lower sternal and upper abdominal areas measured 18 × 14 cm to the rectus abdominis muscles on both sides. Both sides of the anterior rectus sheath were also resected ( Fig. 23.1 ). The lower sternal bony defect measured 13 × 6 cm ( Fig. 23.2 ). Two chest tubes were placed by the primary service. The left superior epigastric vessels were apparently transected during the resection. However, the right superior epigastric vessels remained intact.

Operative Plan and Special Considerations
This was a large composite defect of the lower chest and upper abdomen with a sizable sternal bony defect. Only a small portion of the skin defect could be closed primarily after undermining. The sternal bony defect should be reconstructed with at least semirigid material. In this case, Strattice, a relatively rigid biological mesh was selected for the sternal bony reconstruction. A right rectus abdominis muscle could be used as a turnover flap to provide reliable soft tissue coverage to the Strattice. The muscle flap, based on the right superior epigastric vessels, could be elevated from the abdominal wall on the right side. It reached to at least midsternal level and was covered with a split-thickness skin graft for definitive wound closure. This composite defect could be reconstructed with a semirigid biological mesh and a well-vascularized skin grafted muscle flap with almost no donor site morbidities because the rectus abdominis muscle flap donor site could be closed primarily.
Operative Procedures
Under general anesthesia with the patient in the supine position, the reconstructive procedure started after an adequate tumor resection. A 5-cm posterior rectus sheath defect over the upper abdomen was repaired with 2-0 PDS sutures in a figure-of-eight. The lower sternal bony defect, measuring 13 × 6 cm, was reconstructed with Strattice. The selected Strattice had several perforated holes. Scissors were used to prepare a 13 × 6 cm Strattice, which was placed onto the lower sternal bony defect while the dermal side was facing up, approximated with several interrupted 2-0 PDS sutures followed by 2-0 PDS sutures in simple running fashion ( Fig. 23.3 ).

A right paramedian skin incision was designed in the right abdomen ( Fig. 23.4 ). The proposed incision was infiltrated with 1% lidocaine with 1:100,000 epinephrine. The procedure was started by making a paramedian incision to the anterior rectus sheath. Once the anterior rectus sheath was opened, the dissection was performed around the rectus abdominis muscle. During dissection, several tendious intersections were dissected free. The rectus abdominis muscle was identified and after further dissection around the muscle, its entire length was dissected free. The right inferior epigastric vessels were identified and divided with hemoclips near the muscle’s origin. The muscle was then divided with electrocautery very close to the suprapubic symphysis area and the muscle flap was completely dissected free from the posterior rectus sheath. Before further dissection of the muscle, the superior epigastric vessels were identified. The flap was then turned over to cover the soft tissue defect in the lower sternal area ( Fig. 23.5 ). The muscle flap was completely inset into the defect to cover the entire exposed Strattice and was approximated to the adjacent tissue with several interrupted 3-0 Vicryl sutures ( Fig. 23.6 ).