Clinical Presentation
A 67-year-old White male had a chronic wound in the right axilla secondary to previous radiation for treatment of his advanced metastatic lung cancer. He had responded incredibly well to chemotherapy for his lung cancer and had been cancer-free since the completion of the last chemotherapy. The patient was referred by his medical oncologist for possible closure of this longstanding wound in his right axilla. On initial examination, he had a 2 × 2 cm deep open wound with significant indurated and fibrotic surrounding tissues from his previous radiation ( Figs. 15.1 and 15.2 ).

Operative Plan and Special Considerations
Adequate debridement was planned to excise all fibrotic tissues around and deep to the open wound. Such a debridement should be done to healthy and normal-looking tissue either around or at the base of the wound. Care should be taken to avoid injuries to neurovascular structures in the axilla while removing all deep fibrotic tissues. Because of the location of potential soft tissue defect after the debridement, a pedicled parascapular flap could be a good option for reconstruction of the axillary wound. The flap can be elevated and tunneled to the defect without any tension. In addition, the flap donor site can be closed primarily without any problems.
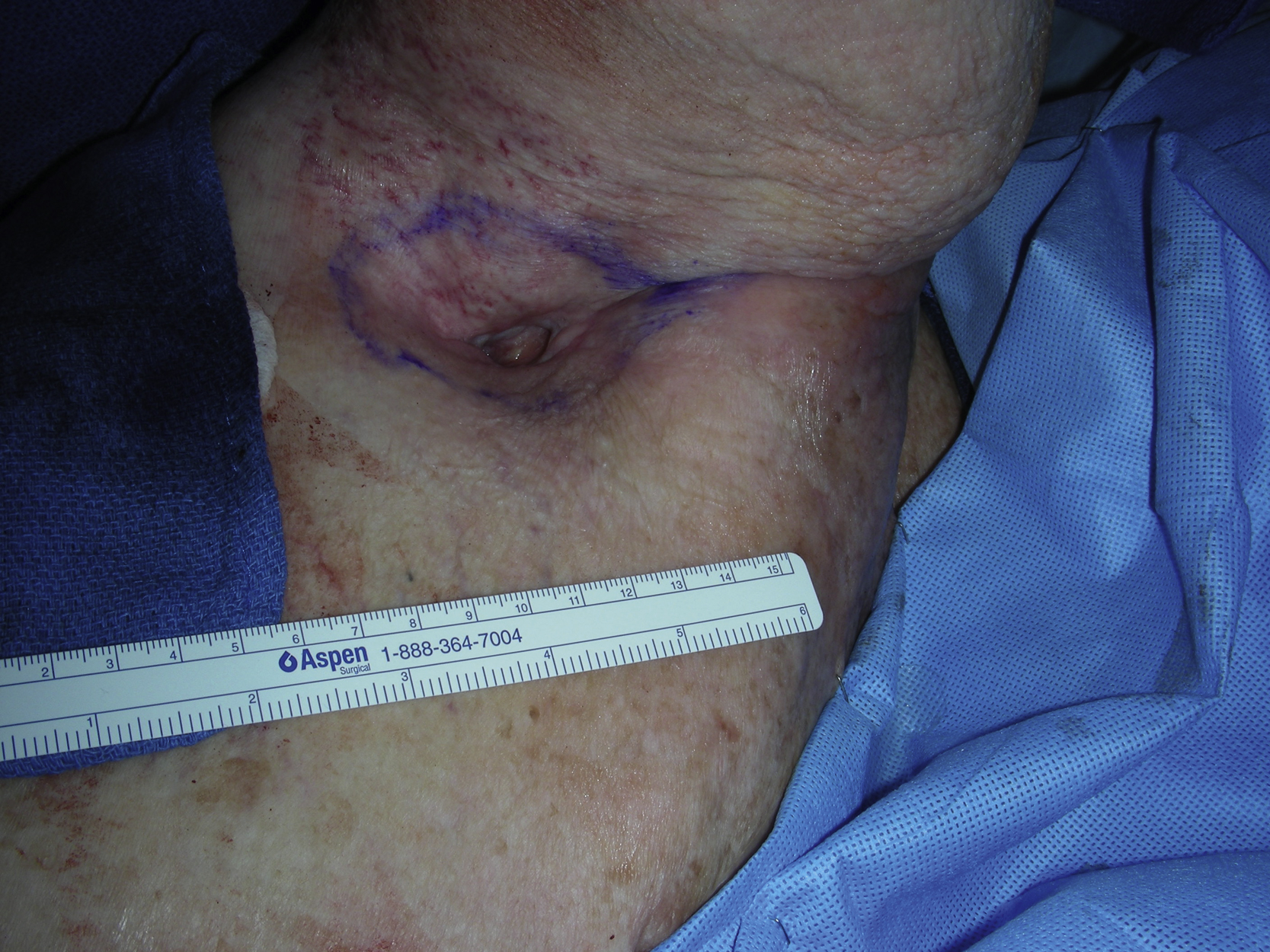
Operative Procedures
Under general anesthesia with the patient in the left lateral decubitus position, his right axillar wound was debrided and the wound excision was carefully done, under direct vision, to the healthy-looking tissue free of fibrosis. After debridement, the new wound measured 8 × 5 cm ( Fig. 15.3 ). The wound was irrigated with Pulsavac.

The pedicled parascapular fasciocutaneous flap was designed over the right back ( Fig. 15.4 ). A handheld Doppler was used to map the descending branch of the circumflex scapular vessel. An 8 × 5 cm skin paddle was marked on the back because it could easily reach to the right axilla without any tension. The proposed skin incision was infiltrated with 1% lidocaine with 1:100,000 epinephrine.










