Case 1
Clinical Presentation
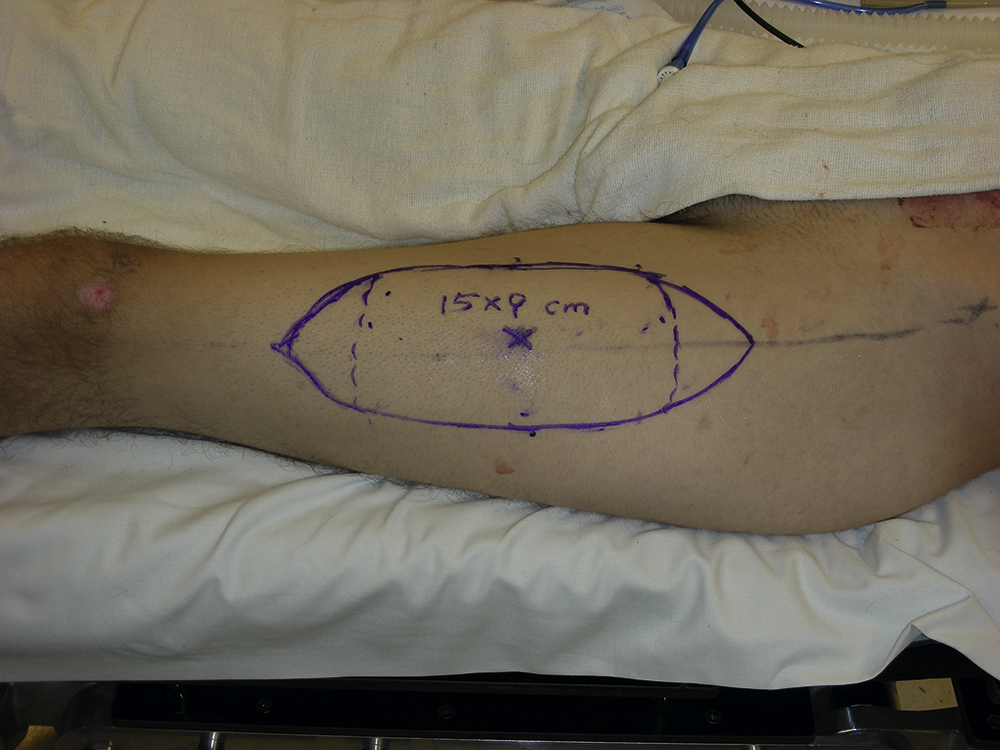
An 18-year-old man fell off a moving vehicle and was then struck by the same vehicle. He was intubated and was in critical condition. Initial injuries included an open skull fracture with exposed intracranial contents, scalp avulsion, left-sided facial avulsion, left superior and lateral orbital wall fractures, bilateral sphenoid sinus fractures, bilateral temporomandibular joint fractures with extension into the intraarticular space on the right, left mastoid fracture, and a cervical spine fracture. Once stabilized, the patient was immediately taken to the operating room by the trauma service for debridement of open wounds. He was found to have a soft-tissue defect measuring 10 × 14 cm of the left face and scalp with a missing zygomatic arch, avulsed left ear, and avulsed left facial nerve. Nine days later, a second facial wound debridement was performed by the plastic surgery service and careful planning for reconstruction was done in the operating room ( Figs. 10.1 and 10.2 ).


Operative Plan and Special Considerations
Because of the size of this large facial wound and the missing zygomatic arch and portion of the zygoma, the initial definitive reconstruction would include a free anterolateral thigh (ALT) perforator flap for soft tissue coverage after adequate bony reconstruction for the left zygomatic arch and zygoma. Once the soft tissue wound healed, the patient would need several staged reconstructive and cosmetic procedures to improve the final outcome. Possible future procedures would include a flap debulking procedure, lateral canthopexy or canthoplasty to reposition the lower eyelid position, hairline reconstruction via scalp tissue expansion, scar revisions, and epidermal skin graft to improve the flap’s colour match. The patient was informed about the expected outcomes with conventional and contemporary reconstructive and cosmetic procedures. Preoperatively, the left facial artery and vein were evaluated by duplex scan to determine whether they could be used as recipient vessels for microvascular anastomoses. In addition, perforators in each thigh were mapped by duplex scan so that a preferred site for harvesting a free ALT perforator flap could be decided. In addition, the patient’s other trauma issues were properly managed or cleared by the trauma service for his initial definitive reconstruction.
Operative Procedures
Under general anesthesia, the entire open facial wound and exposed bones were debrided. After irrigation, the wound appeared to be clean and fresh and ready for definitive soft tissue reconstruction.
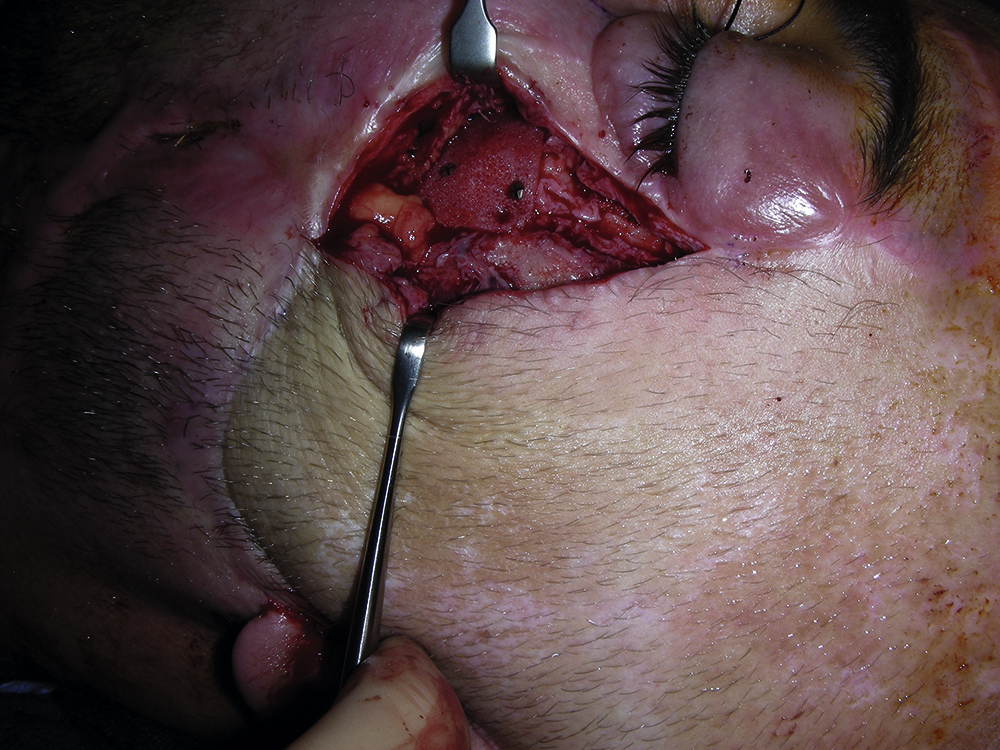
The midface bony reconstruction was performed first. The left zygoma including part of the zygomatic arch was reconstructed with a 7 × 2 cm Medpor implant. The Medpor implant was fashioned to replace the missing bony parts of the midface after being soaked with antibiotic solution. The Medpor implant was used to restore the lateral cheek and lateral orbital rim. This additional fixation was performed with a 1.5-mm plate and secured with multiple screws. A 2.4-mm titanium plate was contoured and placed to act as a zygomatic arch. It was secured with multiple screws ( Fig. 10.3 ).

The left facial artery and vein were identified and explored next. The facial artery and the vein were dissected free and prepared under loupe magnification for microvascular anastomoses.
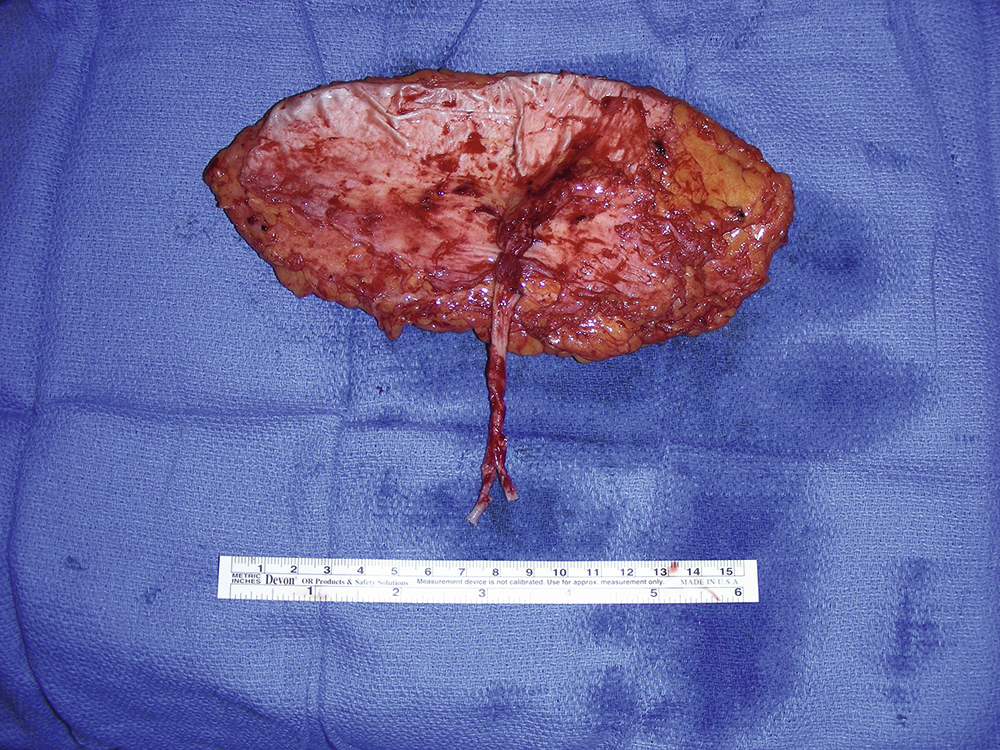
The left ALT perforator flap was harvested ( Fig. 10.4 ). A 15 × 9 cm skin paddle was marked and a single perforator was identified and dissected out. The flap was dissected more superiorly, laterally, and inferiorly in order to have a bigger skin paddle. After about 3-cm intramuscular dissection, the junction of the perforator to the descending branch of the lateral circumflex vessels was identified. During the dissection, a motor nerve to the vastus lateralis muscle was preserved. The pedicle dissection was performed in a retrograde fashion and the most proximal dissection was performed toward the profunda. The pedicle was then divided with a hemoclip ( Fig. 10.5 ).
The flap was prepared under loupe magnification. Both the artery and the vein were prepared with microscissors and flushed with the heparinized saline solution. The flap was temporarily placed on the left facial wound. A skin tunnel was made and the pedicle was placed through the tunnel.
The microvascular anastomosis was performed under microscope. Both facial artery and vein were divided with hemoclips. The arterial microvascular anastomosis was performed in an end-to-end fashion with 8-0 nylon suture. The venous microvascular anastomosis was performed with a 2.5-mm coupler in an end-to-end fashion. Once both arterial and venous anastomoses were completed, there was a good arterial and venous flow and the flap appeared to be well perfused.
A 3 × 0.5 cm full-thickness skin graft was harvested from the distal portion of the flap. The skin graft was defatted and approximated as a small tube with 5-0 chromic sutures. It was sutured to reconstruct the left ear canal and immobilized with a plastic tube.
The flap inset was inserted into the facial defect with multiple 3-0 Monocryl sutures in half-buried mattress fashion after placing a drain. Some of the skin closure was done with a staple. The left neck skin wound was simply approximated with skin staples ( Fig. 10.6 ). The left thigh flap donor site was closed in two layers for deep dermal and skin closure.

Follow-Up Results
On postoperative day 1, moderate venous congestion of the ALT perforator flap was noted and duplex scan also demonstrated possible venous microvascular stenosis. The patient was taken emergently to the operating room for exploration. However, both arterial and venous pedicles appeared patent without twisting or kinking ( Fig. 10.7 ). The flap was monitored through the rest of his hospitalization and remained viable. He was doing well and was discharged from the hospital on postoperative day 10.

The patient subsequently developed lower eyelid ectropion secondary to the lateral orbital scarring and the “pulling” force from the ALT flap ( Figs. 10.8A and B ). Five weeks after the initial reconstruction, he underwent release of the contracture, lateral canthoplasty, resuspension of the ALT flap, and full-thickness skin grafting to a resulting area of open wound ( Figs. 10.9 and 10.10 ).




During subsequent office visits, the patient was noted to have developed hypertrophic scarring of his face and neck, in addition to persistent tearing and difficulty in fully closing his left eye ( Fig. 10.11 ). He was treated with scar massaging and two rounds of Kenalog injections. There was bulkiness of the free flap and thinning of the left midface ( Fig. 10.12 ). About 8 months after his initial revision surgery, he underwent repeated left lateral canthoplasty, debulking of the ALT flap, left midface suspension, and cheek augmentation using Medpor implant ( Figs. 10.13 and 10.14 ).



The ectropion was corrected ( Fig. 10.15 ) and the patient then underwent placement of a scalp tissue expander for hairline scalp reconstruction ( Figs. 10.16 and 10.17 ). Over the next 3 months, he underwent fills to a final volume of 230 mL ( Figs. 10.18 and 10.19 ). The expander was then removed and the resultant expanded temporoparietal scalp flap was advanced to reestablished the anterior temperal hairline scalp ( Fig. 10.20 ).






Once the scalp hairline reconstruction had healed, an additional procedure was undertaken to improve the color mismatch between the ALT flap and the native face/scalp skin ( Fig. 10.21 ). An epidermal skin graft was taken from the parietal scalp and sutured to the flap after de-epithelialization of a 14 × 8 cm region ( Figs. 10.22–10.24 ). The resultant color match was noted to be greatly improved and the graft had near complete take ( Figs. 10.25 and 10.26 ).






Final Outcome
This patient underwent five reconstructive surgical procedures over a 2-year period. He had well-healed soft tissue reconstruction from his free ALT flap and stable bony reconstructions with Medpor implants and titanium reconstruction plates. At follow-up, the patient’s only complaint was some edema in the lower eyelid area, which may represent persistent lymphedema, although at this point he did not want to undergo any other procedures and was satisfied with his cosmetic outcome after such extensive and complex injuries.
Although the skin color match of the ALT flap may continue improving, the persistent swelling in his lower eyelid region remains. He also has persistent scleral show and facial nerve paralysis on the injured side, but he has no major functional issues such as dry eye symptoms. At this point, the patient declines any further major reconstructive procedures such as facial nerve reconstruction. He has near normal-looking appearance and facial contour ( Figs. 10.27 and 10.28 ). He has resumed his normal life and has been followed by the plastic surgery service as needed.


Pearls for Success
The complex facial trauma presented in this case poses a reconstructive challenge for plastic surgeons. Multiple contemporary reconstructive surgical techniques can be used to give the patient an optimal outcome following extensive facial trauma. Medpor implants are composed of porous high-density polyethylene. When implanted in the face, they are stable and resistant to degradation. The advantages include ease of contouring and handling, resistance to infection, and incorporation into the host tissue via vascular ingrowth. Multiple recent studies, however, have shown similar functional outcomes when comparing Medpor implant reconstruction with bone graft, with the advantage of avoiding donor-site morbidity and shorter operating time.
The free ALT perforator flap has a large pedicle length, minimal donor-site morbidity, large and reliable skin paddle, customization of flap size to fulfill soft tissue reconstruction of the facial soft tissue defect. The flap is amenable to thinning, either at the initial operation or at a later stage. A tissue expander can be used for the reconstruction of hair-bearing scalp and epidermal grafting can be used to improve the color match after a facial fasciocutaneous flap reconstruction.
Numerous contemporary reconstructive techniques, including a free ALT perforator flap for soft tissue coverage and Medpor implant for initial midface reconstruction, followed by flap debulking, lateral canthoplasty, midface augmentation and lift, scalp tissue expansion for hairline reconstruction, and epidermal skin grafting for optimal skin color matching, can be used for a patient after severe facial trauma associated with significant soft tissue and bony loss. Good cosmetic and functional outcome can be achieved with our approach, but multiple staged reconstructions are often necessary to yield the best possible reconstructive outcome.
Case 2
Clinical Presentation
A 56-year-old White male sustained a self-inflicted gunshot wound to his left face. He had extensive left facial soft tissue wounds and comminuted fractures of the left zygoma and mandible. An on-call plastic surgeon carried out debridement of the facial soft tissue wounds, placement of multiple external fixators for the comminuted mandibular fractures, and repair of soft tissue wounds ( Figs. 10.29 and 10.30 ). The patient’s care was transferred to the author for more definitive reconstruction of facial soft tissue wounds including an intraoral soft tissue defect and bony fixations for comminuted fractures of the left zygoma and mandible.










