Spondylolysis/Spondylolistheses
M. Timothy Hresko
Pars Repair
Operative Indications
Failed nonoperative treatment of documented pars intra-articularis defect
MRI—absence of intervertebral disk degeneration
Less than 5 mm of translation of superior vertebral body
Pain relief on pars injection
Equipment
Intraoperative imaging: fluoroscopy or navigation
Cannulated drill system, 4.5 mm solid screws (laminar “Buck” screw technique)
18-gauge stainless steel “Luque wires” or spinal cable (“Scott” wire technique, most applicable for L4 or cephalad)
Pedicle screw system (pedicle screw technique)
Positioning
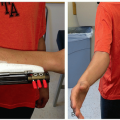
Prone on radiolucent table (Figure 7.1A)
Flex hips to reduce anterior pelvis tilt and lumbar lordosis (Figure 7.1B)
Procedure-Specific Checklist
Implant for your specific procedure
Intraoperative fluoroscopy to confirm surgical site at correct location
Compare to preop imaging—be cognizant of transitional LS vertebrae
Surgical Approach
Surface landmark of dimple of Venus (posterior iliac spine) at level of S1 spinous process
Midline approach 8 cm cephalad from S1
Raise skin flap to iliac crest
Elevate muscle from L5 lamina to L4-L5 facet, lateral to base of transverse process (if using Scott wire technique elevate to tip of TP and ventral on the specific vertebrae)
Maintain ligament of posterior process to L4, L5, S1
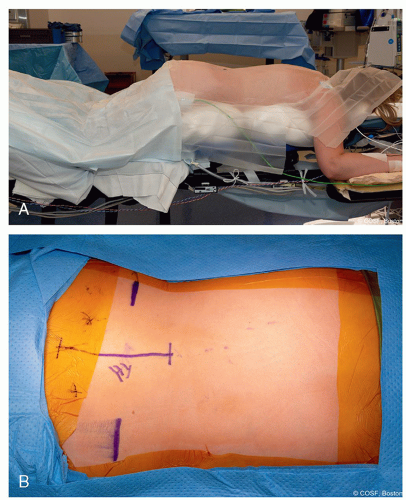 Figure 7-1 ▪ A, Position on radiolucent table with hip flexed 30° to 45°. B, Incision based on surface anatomy of posterior iliac spine and iliac crest. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
Techniques in Steps
Common to All Technique
Obtain bone graft from iliac crest—cancellous
Use Rongeur, curette, or burrs to clean out pars defect
Buck screw technique (Figure 7.2A-C)
Preoperative CT to confirm lamina intact—absence of bifid lamina
Use fluoroscopy and K-wire to plan path for cannulated drill AP and lateral fluoroscopy
Burr starting point at inferior aspect of ipsilateral lamina
Percutaneous insertion of threaded guide pin for cannulated drill inserted midline and distal to incision, angled lateral and ventral under fluoroscopy
Advance guide pin to pars defect
Place bone graft
Advance guide pin to anterior superior cortex
Drill over wire and far cortex
Remove wire and place solid 4.5 mm screw—bicortical
Repeat on contralateral side
Decorticate base of TP and lamina
Place additional bone graft on lamina
Close wound
Pass loop wire over lateral aspect of TP to base of TP
Alternative is place pedicle screw or bone screw and washer in pedicle and loop wire under the washer
Decorticate base of TP and lamina
Pass free end of wire through posterior ligament in “figure of 8” fashion and secure on contralateral side of spinous process
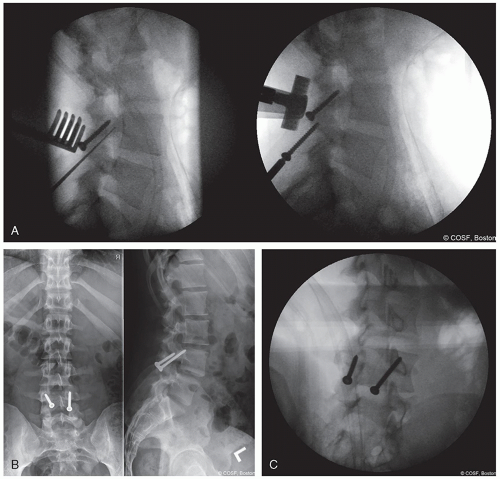
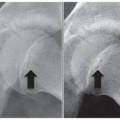
Figure 7-2 ▪ A, Image of lateral lumbar spine showing insertion angle of drill and screw. B, AP and lateral of lumbar spine Buck screw. C, Oblique image showing bicortical fixation. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
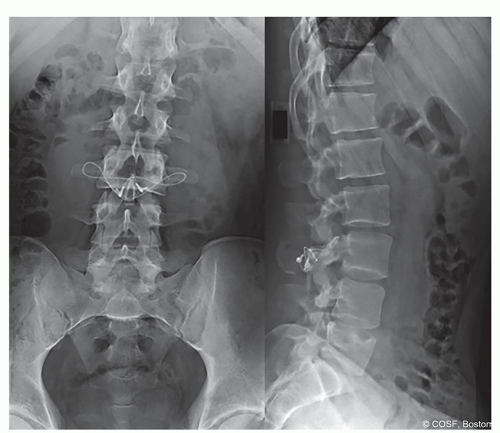
Figure 7-3 ▪ Scott wiring AP and lateral. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
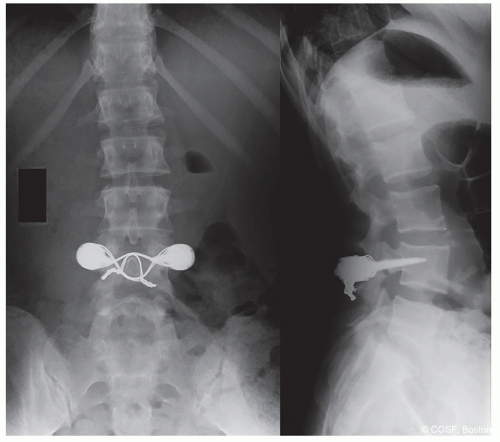
Figure 7-4 ▪ Pedicle screw plus wiring MR4201677. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
Insert bone graft in pars defect and lamina ventral to wire
Place contralateral wire in a similar fashion
Tighten both wires
Close wound
Pedicle screw
Place bilateral polyaxial pedicle screws avoiding facet joint
Decorticate base of TP and lamina
Insert bone graft into pars defect, base of TP, and lamina
Implant secured to posterior process. Implant options:
Contour 4.5 mm rod in “U” shape passed rod inferior to L5 spinous process
Polyethylene cord instead of rod (physician directed use, not FDA approved)
Wire
Insert rod into pedicle screw head and compress
Postoperative Care
Optional use of lumbosacral orthosis
Out of bed to chair and ambulate as tolerated
Short course of oral opioid; avoid nonsteroid anti-inflammatory drugs
Restricted lumbar hyperextension/flexion activity 4 to 6 weeks
CT scan at 3 months to assess healing and return to conditioning for sport
Complications
Infection
Nonunion
Loss of motion of cephalad disk space due to facet impingement or dissection around TP (Scott wiring)
Posterolateral Fusion—In Situ
Operative Indications
Failed nonoperative treatment of documented spondylolysis or low-grade (<50% slippage) spondylolisthesisRelated posts:
 Occiput and Posterior Cervical Instrumentation
Occiput and Posterior Cervical Instrumentation
 Decision-Making in Pediatric and Adolescent Hip Disorders
Decision-Making in Pediatric and Adolescent Hip Disorders
 Clubfoot Casting and Heel Cord Lengthening
Clubfoot Casting and Heel Cord Lengthening
 Radioulnar Synostosis Derotation Osteotomy
Radioulnar Synostosis Derotation Osteotomy
 Neuromuscular Hip Surgery: Prevention to Reconstruction
Neuromuscular Hip Surgery: Prevention to Reconstruction
 Minimally Invasive Techniques for Foot Deformity Correction
Minimally Invasive Techniques for Foot Deformity Correction

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


