Clubfoot Casting and Heel Cord Lengthening
James R. Kasser
Treatment of Clubfoot Using the Ponseti Method
I had the good fortune to spend time with Dr Ponseti in 1998, which resulted in major change in my management of clubfoot. Since that time, I have used his method of cast correction with minimal change to the technique he first showed me. He was a gracious man, first sending me his book on clubfoot treatment followed by a weeklong visit to our institution. He quickly convinced me of the value of his treatment method (Figure 27.1). I then spent some time with him refining my understanding of his technique and believe, as many do, that it revolutionized clubfoot management and will remain the standard of care.
Most clubfeet are diagnosed by ultrasound at 18 to 24 weeks’ gestation in modern times (Figure 27.2). In our state, Massachusetts, well over 90% of clubfeet are diagnosed by ultrasound prenatally. In many cases, families seek information about clubfoot management and potential associated problems
for their unborn child immediately following this fetal diagnosis. Orthopedic surgeons need to provide information to families once the fetal diagnosis of clubfoot is made and construct a plan for management including information about the expected outcome. This will relieve anxiety and provide valuable information to the family. Families may get involved in support groups online or in person, speak with other families with clubfoot diagnosis, and may want to see patients being treated for clubfoot or see cases with long-term follow-up. In the absence of this information, expectant parents may erroneously believe that the diagnosis of clubfoot equates to lifelong disability.
for their unborn child immediately following this fetal diagnosis. Orthopedic surgeons need to provide information to families once the fetal diagnosis of clubfoot is made and construct a plan for management including information about the expected outcome. This will relieve anxiety and provide valuable information to the family. Families may get involved in support groups online or in person, speak with other families with clubfoot diagnosis, and may want to see patients being treated for clubfoot or see cases with long-term follow-up. In the absence of this information, expectant parents may erroneously believe that the diagnosis of clubfoot equates to lifelong disability.
 Figure 27-1 ▪ Dr Ponseti (foreground) instructing in the utilization of his clubfoot casting technique. We converted to Ponseti method as the primary treatment for clubfoot deformity in 1998. |
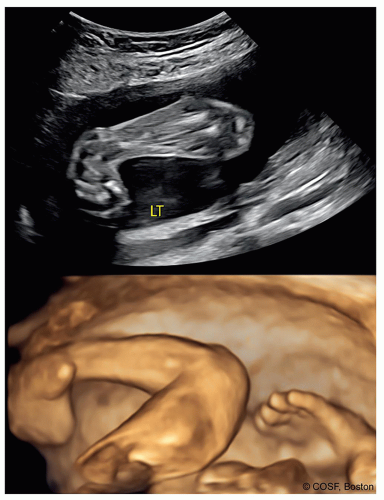 Figure 27-2 ▪ Nearly all clubfoot deformity is diagnosed prenatally by ultrasound. Characteristic appearance includes a supinated fixed deformity with an angle less than 90° between the first ray and the long axis of the tibia. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
At first evaluation following delivery, a diagnosis of clubfoot made prenatally is confirmed and classified. The false-positive rate for clubfoot based on ultrasound at 18 to 24 weeks is in the range of 10%. A classification system for clubfoot should be used. Either the Dimeglio or Pirani system is commonly the basis for classification of severity of foot deformity. We use the Dimeglio system (Figure 27.3).
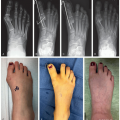
The deformity in clubfoot is a combination of the following (Figure 27.4):
Cavus with plantar flexion, primarily of the first ray unless this is an atypical clubfoot.
Medial and plantar displacement of the navicular with calcaneonavicular ligament shortening
Medial displacement of the calcaneus under the talus, appearing as varus deformity
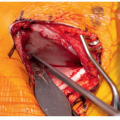
Equinus with a short Achilles tendon, tight posterior capsule, and tight posterior calcaneal fibular ligament
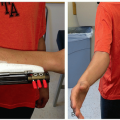
The treatment for clubfoot is manipulation and staged casting—“the Ponseti method.” The materials needed are Webril or cotton padding, stockinet or similar material to prevent the top of the cast from irritating the thigh, and plaster or soft fiberglass roll. Serial casting and manipulation are the standard treatment. A long leg cast must always be used in order to correct the clubfoot deformity (Figure 27.5).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


