Decision-Making in Pediatric and Adolescent Hip Disorders
Michael B. Millis
Introduction
Developmental hip diseases—in particular hip dysplasia, Legg-Calvé-Perthes disease, and slipped capital femoral epiphysis (SCFE)—are important not only as a cause of short-term pain and dysfunction but also as the most common cause of osteoarthritis (OA) of the hip in adulthood. For that reason, indications for treatment in the young include situations where symptoms may be limited but radiographs indicate the risk to the untreated hip is high.
For the treatment of developmental hip conditions, the growing years present a period of both opportunity for care and challenge in decision-making. Predicting outcome can be difficult as mild cases may be hard to diagnose clinically and more involved cases can undergo normalization over time. For instance, in treating a patient with developmental dysplasia of the hip (DDH), a period of observation without treatment is recommended to assess the natural progression of hip growth and development (Figure 18.1). However, for the most part, timely diagnosis is essential to predict outcomes. Abnormal hip mechanics rarely correct; failure of improvement on serial images indicates intervention may be warranted. For example, hip subluxation diagnosed on an anteroposterior pelvic radiograph by a break in Shenton line is an indication for intervention (Figure 18.2).
As a first principle, hip anatomy by imaging is a good guide to the mechanical environment, but there is no substitute for good information in making the best decisions. The surgeon must “have a handle on” relevant issues of hip growth, pathomechanics, and surgical and nonsurgical therapies and their consequences to make the best decision for each patient. Optimal treatment of the patient with a hip disorder also requires recognition of the patient/family perspective, which demands education as a prerequisite to the ideal of shared decision-making. Open minds, thoughtful analysis, pattern recognition, and experience guide the treating team. Every individual patient, however, deserves careful consideration for variations on common themes.
Analysis of the Clinical Problem
The History and Interview
The human element in therapeutics may be as important as the mechanical/organic. Deep interest in the stories that patients and families tell can pay rich dividends. After introduction, sitting down with the family is a great groundbreaker. Open-ended questions are ideal starters, with time allowed for considered answers. Checklists help ensure that all important areas of inquiry are covered. In nonacute situations, encouraging the patient/family to send a brief summary story and questions ahead of the first appointment can be reassuring and efficient.
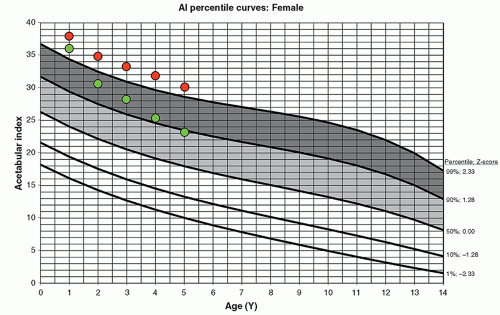 Figure 18-1 ▪ Percentile curves for acetabular index (AI) for females are shown. The critical range representing abnormally high AI for age between the 90th and 99th percentiles is indicated. The dots represent values of AI measured at the time of closed reduction of the hip and each year during subsequent visits. The green dots show what we consider a true remodeling of the acetabulum, whereas the measured AI is decreasing over the years following reduction and there is a change in the percentile categories over time. In comparison, the red dots show what we consider inadequate remodeling of the acetabulum. Despite the decrease in the absolute numbers of the AI, for each measurement, the values are in the same percentile zone, which represents failure to correct over time. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
The Physical Examination
Physical examination offers the opportunity to assess the patient and the hip during function. Each examination also must be age appropriate. There is value in applying stress, to elicit abnormalities that otherwise would be missed, yet inflicting pain is counterproductive. Delaying the examination until after the interview encourages relaxation. Explaining tests and maneuvers and their purpose just before they are done is a confidence-builder, as is doing potentially painful tests last. No examination is complete without measurements and the dynamic assessment of stance and gait. Measure and record. A checklist is essential.
Imaging
Imaging is necessary but not sufficient alone for best therapeutic decision-making without a well-taken history, physical examination, and informed discussion. All available images should be collected to gain temporal sense of the hip issue. Always think in 3 dimensions. Include dynamic imaging if possible. Remember the importance of the soft tissues that are nearly invisible in radiographs. Biplanar imaging assists in understanding of 3-dimensional (3D) reality. Lateral views of the femur (frog leg/Lauenstein; Dunn) and the acetabulum (false profile) are useful. Standing views may reveal subtle instability. Functional views can simulate corrections and clarify questions of congruity and freedom of motion (Figure 18.3).
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


