and Frank Hölzle2
(1)
Department of Oral and Maxillofacial Surgery, Klinikum rechts der Isar, Technische Universität Munich, Munich, Germany
(2)
Department of Oral and Maxillofacial Surgery, University Hospital of RWTH Aachen University, Aachen, Germany
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-3-319-53670-5_12) contains supplementary material, which is available to authorized users.
12.1 Development and Indications
The soleus perforator flap basically is a “true perforator flap” with a short pedicle, consisting of septo- or septomyocutaneous perforators on which anastomoses are performed; thus, none of the main vessels of the lower leg has to be sacrificed. The perforators mostly arise from the peroneal vessels and are exposed at the proximal half of the lateral lower leg to allow for primary closure. Because of the similar anatomy of the skin paddle, the raising of this flap will easily be learned by surgeons being familiar with the osteocutaneous fibular flap.
Before short-pedicle perforator flaps like the soleus perforator flap were established, free flaps from the lower leg were raised at the tibial posterior [631], tibial anterior [385, 582], and peroneal vessels [625], which served as the vascular pedicle.
The tibial posterior flap was first described by Zhang et al. [631] as a distally based fasciocutaneous flap for defect coverage at the foot and lower leg. In an anatomical study on 20 cadavers, the author found a high number of septocutaneous perforators coming from the tibial posterior artery. According to this study, three septocutaneous perforators from the tibial posterior artery can be found in the proximal, seven in the middle, and three in the distal lower leg. A precise description on the number and location of the septocutaneous branches of the tibial posterior artery was also given by Carriquiry and coworkers, who found four to five such perforators, each being located 9–12, 17–19, and 22–24 cm above the medial ankle [70]. Amarante et al. used this flap as a distally pedicled transplant for defect coverage at the foot, and they reported about two regular branches which they found 4 and 6.5 cm above the medial ankle [11]. Similar findings were published by Koshima et al., who also preferred to raise flaps from the tibial posterior artery at the distal half of the lower leg due to the high number of septocutaneous perforators in this region [297]. To avoid sacrifice of this main vessel of the lower leg, they anastomosed their flaps directly to the perforator, leaving the tibial posterior artery intact [297]. Hung and coworkers later transferred this flap by means of microvascular anastomoses at the tibial posterior vessels for the covering of extended defects of the extremities [239]. A special indication of the free tibial posterior perforator flap was described by Chen et al., who performed reconstructions of the esophagus in three cases [82].
Focusing on the tibial anterior artery, Morrison and Shen described on the basis of their own cadaveric dissections the proximal third of the lower leg to be the most reliable donor area to raise flaps based on septocutaneous perforators branching off from this artery, each having a vascular territory of 15 × 10 cm [385]. According to the first clinical applications, three types of tibial anterior flaps were described [385, 468, 582], all of them mainly being used for local defect coverage at the lower leg. The main advantages of flaps based on septocutaneous perforators from the tibial anterior artery are their wide arch of rotation, their thinness, and the ease of flap raising, making them an ideal transplant for defect coverage at the foot [385].
Although Yoshimura et al. early described the possibility of raising cutaneous flaps on the peroneal vessels [625–627], only a few publications report about the usefulness of this flap until now. This paucity of clinical applications can be explained by the fact that cutaneous perfusion by the perforating vessels was reported to be unreliable [67, 70, 568], the localization perforators to be extremely variable [67, 482], and the exposure of the peroneal vessels with an intact fibula as being difficult [406, 568].
The demanding technique in raising the peroneal flap and the general disadvantage to sacrifice one of the main arteries when using conventional flaps in the lower leg led to further modifications in flap design. With the development of perforator flaps on other regions of the body, also the lower leg was taken into consideration as a donor site for perforator flaps with a short pedicle. Since the anatomy of the cutaneous perforators was well known from the above-mentioned studies, it was only a small step to raise short-pedicle “true” perforator flaps without sacrifice of the source vessels. The small cutaneous vessels in these types of flaps are traced to the source artery by retrograde dissection, so that adequate pedicle length and diameter for anastomosis can be obtained [601, 604].
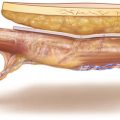
12.2 Anatomy
Numerous anatomical studies have been performed to investigate the number and course of the cutaneous branches of the peroneal artery. In dissections on 80 cadavers, Schusterman and coworkers [482] found 3.74 cutaneous perforators from the peroneal artery, 1.3 of them showing a septocutaneous and 1.9 a myocutaneous vessel course; 0.6 vessels in average were adherent at the fascia between the soleus and the peroneus muscles without piercing these muscles. For the osteocutaneous fibula flap, Schusterman proposed to include the whole septum into the skin paddle because of the variability of perforators. Yoshimura, who first described the peroneus flap, found 4.8 cutaneous branches, 71% of them having a myocutaneous course through the flexor hallucis and soleus muscles [626]. Whereas Yoshimura proposed to raise the skin paddle more distally, other authors consider the middle third of the lower leg to be the safest donor area for the skin flap. Further anatomical studies in 30 cadavers have shown that 4.2 perforating vessels in average branch off from the peroneal artery to the skin, tending to run myocutaneously in the proximal third and septocutaneously in the distal third of the lower leg [601]. Like with the main arteries, perforators at the lower leg consist of one artery and two concomitant veins and pierce the strong crural fascia. Although the localization of the cutaneous branches generally is quite variable, Wolff et al. found that the most proximally and distally located perforating vessels are the most uniform. These are consistently found in an area 5–15 cm below the fibula head and in the distal third of the lower leg 8–12 cm above the lateral ankle. To make direct closure of the donor site possible, the donor area in the proximal half of the lower leg is preferred; here, the perforators have a course through the soleus muscle. Selective dye injections have shown that one perforating vessel supplies an average cutaneous area of 12 × 7 cm, which is large enough for a number of reconstructive purposes [601]. To identify the course of the vessels, the perforators must be followed up to their origin from the main arteries. In their anatomical study as well as in their clinical cases, the perforators originated exclusively from the peroneal artery, most of them having a course through the flexor hallucis and soleus muscles; in only 18%, the perforators traveled directly to the skin. Due to the deep location of the peroneal artery and the broad posterior intermuscular septum, the length of the perforators was at least 4–5 cm, and the diameter of the vessels varied between 1 and 1.5 mm for the arteries and 1.5 and 2.5 mm for the veins. Additional small branches from the perforator to the surrounding muscles enable the dissection of a well-perfused muscle cuff; no direct branch to the periosteum or fibula bone was found to originate from the perforators.
Based on a dissection of 20 cadaver legs, Heitmann et al. described 4.8 perforators of the peroneal artery having an external diameter at the posterior border of the fibula between 0.3 and 1.5 mm, being 0.6 mm in average [213]. In an early report, Weber and Pederson have shown the feasibility to connect such small vessels when they salvaged the skin paddle of the osteoseptocutaneous fibular flap by performing independent microvascular anastomoses of the perforators in two osteocutaneous fibular flaps [580]. A similar report was given by Yokoo and coworkers who pointed out that such a maneuver can also become necessary in osteomyocutaneous fibular flaps, if the perforator of the skin paddle as a variation is branching off from the tibialis posterior instead from the peroneal vessels [623]. As a consequence of these clinical experiences, Wong et al. conducted an anatomical study to evaluate the use of the soleus musculocutaneous perforator for skin paddle salvage in such situations. In 18 of 20 limbs, they found one or more musculocutaneous perforators of at least 0.5 mm in diameter, being located within 6 cm of the junction of the middle and lower third of the fibula. In this study, only 50% of the perforators originated from the peroneal artery, and in 35% from the tibial posterior vessels so that the authors proposed to preserve one or two soleus perforators during harvest of the osteocutaneous fibular flap until the existence of the septocutaneous perforator is confirmed [610]. A three-dimensional analysis in eight cadavers using a mixture of lead oxide and gelatin revealed 13 perforators in average, originating from the peroneal, popliteal, and tibial posterior vessels; each perforator supplied an area of about 38 cm2 [529]. Clinical applications of perforator flaps from the lateral lower leg were also described by Kawumara and coworkers. They published their experience with free soleus and free peroneal perforator flaps in 23 patients without sacrifice of any main artery in the lower leg. The perforator pedicle length varied between 6 and 10 cm in soleus perforator flaps with the largest skin paddle being 15 × 9 cm and 4–6 cm in peroneal perforator flaps. The maximal size of the skin paddle was 9 × 4 cm; only one flap was lost in this series [264].
12.3 Advantages and Disadvantages
Previous anatomical studies have shown that the skin of the lower leg is supplied by perforators from all three main vessels [70, 385, 529, 582], and this led to the development of free skin flaps from the tibial anterior [385, 470], tibial posterior [11, 264, 297], and peroneal system [601, 627]. To avoid sacrifice of the main artery, tibialis posterior and medial sural [264] free perforator flaps have been raised and were anastomosed directly on the perforating vessel. These “true” perforator flaps were mainly used for defect coverage in the extremities. In a publication of Tsai and coworkers, a free lateral leg perforator flap was used for reconstruction in a patient with an extended anterior cervical scar contracture [551]. In this case, a 22 × 8 cm2 skin flap was elevated from the whole lateral aspect of the lower leg and was based on two myocutaneous perforators which unified about 2 cm below the fibula head. Because the vascular anatomy of the lateral lower leg has meticulously been investigated in previous studies [70, 482, 529, 626] and is also well known from the osteomyocutaneous fibula transfer, exposure of the perforators and flap raising is possible without technical difficulties. Although strong perforators also can be found in the distal third of the lower leg [11, 623], it is recommended to choose a more proximal donor site because here, direct wound closure is possible for a flap width of up to about 7 cm. Other than with the fibula or peroneus flaps, in which the peroneal artery is sacrificed, no preoperative diagnostics is necessary in the peroneal perforator flap to exclude anatomical variations in the course of the major arteries of the lower leg. Therefore, in the conventional flaps of the lower leg, an important part of surgical planning is angiography, which allows visualization of variations and arteriosclerotic damage of the major vessels. In the peroneal perforator flap, the only preoperative measure which can facilitate flap raising is the use of an audible or color-coded Doppler, which can help to locate the perforator exactly. Especially when small flaps are planned, preoperative mapping of the perforators with the Doppler or, which is more precise, color Doppler duplex imaging [189, 427] is helpful to place the first incision in a distance of about 2–3 cm apart from the vessel, so that after completion of flap raising, it will be located in the center of the skin paddle. Using CT angiography, suitable perforators measuring at least 1 mm could be identified preoperatively [593]. Of great importance for successful flap transfer is the fact that anastomosis are performed without tension on the pedicle. Therefore, this type of flap is recommended only if recipient vessels can be expected close to the defect region. In patients with a deficiency of neck vessels, the reverse-flow facial artery was proposed as a recipient vessel for such short-pedicle perforator flaps [226]. Apart from the minimal donor site morbidity, the soleus perforator flap is primarily thin and pliable because it carries only a slim layer of subcutaneous fatty tissue. Thus, it is considered to be more suitable for intraoral reconstruction [601, 604] than perforator flaps from other donor sites which might need additional thinning.
The main disadvantage of short-pedicle perforator flaps is that they have to be anastomosed at their short and small-diameter vessels, and anastomosing these vessels requires special technical skills [290, 585]. Thus, the mastering of small vessel anastomoses with a diameter of 1 mm is a prerequisite for any surgeon intending to do a short-pedicle perforator flap. Moreover, subtle dissection of the small vessels is mandatory to prevent vascular spasm. It is therefore strongly recommended to choose tall and slim patients for the first perforator flaps, because here greater vessels will facilitate dissecting and anastomosing the pedicle. Nevertheless, the soleus perforator free flap has proven to be a reliable method for intraoral reconstruction [593, 599, 600].
12.4 Patient Positioning
The leg is bent at the knee joint and brought in a prone position to get better access to the lateral and posterior aspect of the calf. This is facilitated by supporting the hip with a beanbag. The entire lower extremity is prepped circumferentially, and the foot is draped leaving the foot pulses accessible. A tourniquet may not be used, because it would make identification of the strength and pulse of the perforator impossible. Preoperative auscultation of the region of the posterior intermuscular septum with a Doppler probe will help to localize the most suitable perforator.
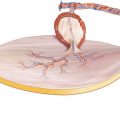
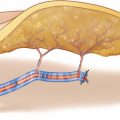
12.5 Flap Design
Because localizing the skin paddle of the soleus perforator flap is completely dependent on the perforator selected for flap raising, the design of the flap cannot be determined before a useful vessel showing a strong pulsation has been exposed. Such a perforator normally can be found a few centimeters distally to the fibular head and along or 1–3 cm posterior to the septum between the peroneal and soleus muscles. The longitudinal axis of the flap is designed parallel to the septum; the length of the flap can reach up to 15 cm, if a strong and pulsatile perforator has been found. The flap width is restricted to about 6–7 cm, which is the limit for tension-free primary closure. The skin incision is marked above the peroneal muscle, keeping a safety distance to the septum of about 2 cm. To prevent injury of the common peroneal nerve, a distance of at least 3 cm is kept to the fibular head (◘ Figs. 12.1, 12.2, 12.3, and 12.4).
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


