Clinical Presentation
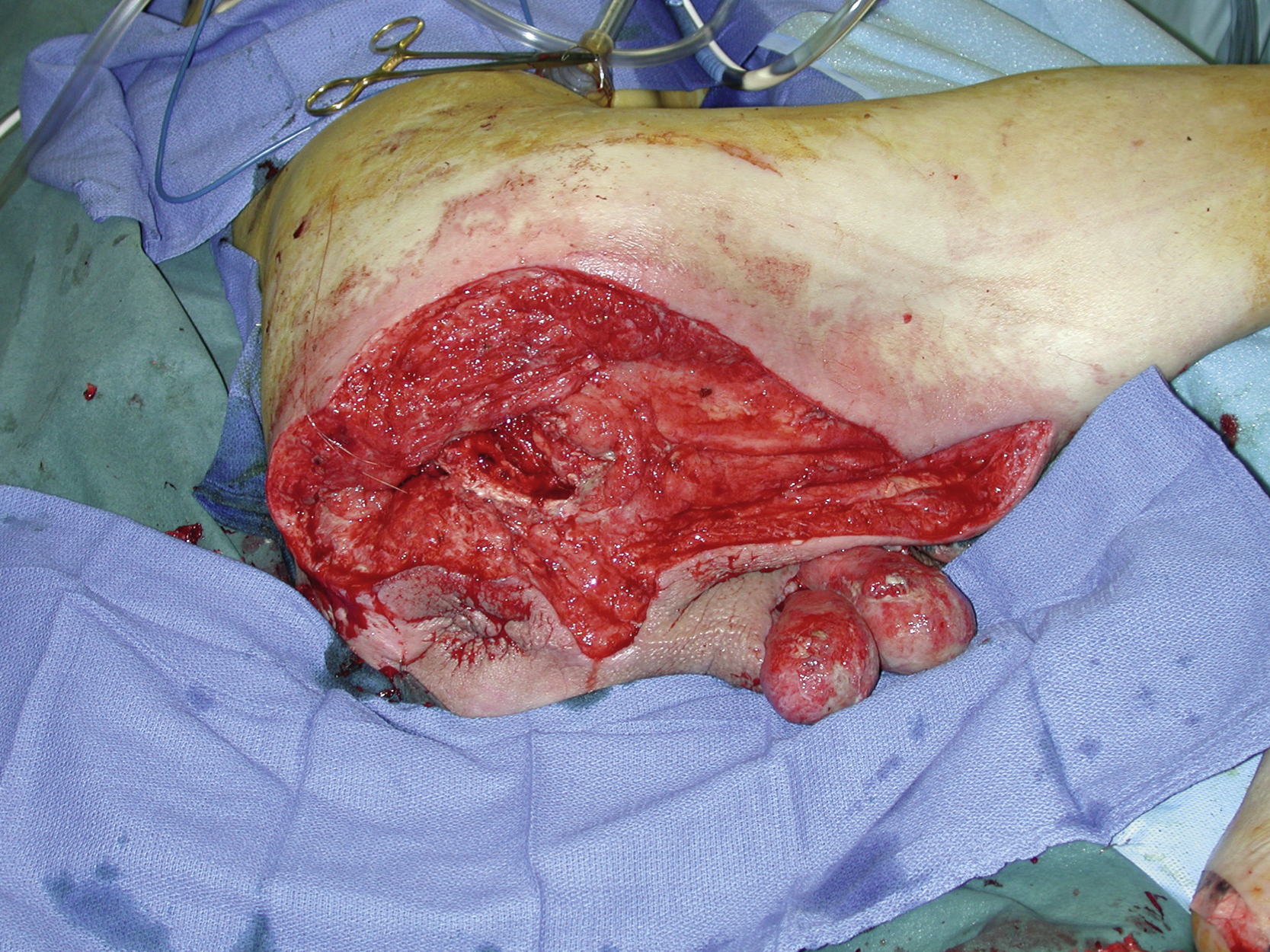
A 76-year-old paraplegic White male with a long-standing history of diabetes developed Fournier’s gangrene and presented to the urology service. The primary service performed emergent radical surgical debridement to control the soft tissue infection. After debridement, a significantly large soft tissue wound involving the entire right ischial, gluteal, and posterior thigh regions as well as bilateral scrotal areas remained ( Fig. 39.1 ). The plastic surgery service was asked for a definitive soft tissue reconstruction. The patient’s medical conditions including diabetes were managed by the medicine service and were reasonably under control.

Operative Plan and Special Considerations
Additional surgical debridement is often necessary before a definitive soft tissue reconstruction. Based on more detailed preoperative evaluation, some parts of the open wound could be closed primarily after local tissue rearrangement or skin undermining. The rest of the open wound including the scrotum could be closed with a split-thickness skin graft (STSG). A combination of STSG and direct wound closure would be necessary for the definitive soft tissue reconstruction. The patient would almost certainly develop recurrent or new ischial pressure sores without proper nursing care.
Operative Procedures
Under general anesthesia with the patient in a left lateral decubitus position, the entire open wound was debrided by the plastic surgery service. All necrotic, unhealthy looking, or colonized tissue was surgically debrided to more healthy bleeding tissue ( Fig. 39.2 ). This was followed by Pulsavac irrigation.
The wound edges in the gluteal and posterior thigh regions were undermined significantly and approximated together with some degree of local tissue rearrangement. Such a wound approximation was accomplished in two layers. The deep dermal was closed with several interrupted 3-0 Monocryl sutures and the skin was closed with skin staples. In this way, nearly half of the wound could be closed without the need for skin grafting.
The remaining open wound including each scrotum was closed with a STSG. All skin grafts were harvested from the bilateral lateral thighs. The STSG with a thickness of 0.015 inch (0.038 cm) was mashed to 1.5 to 1 ratio. All skin grafts were placed over the open gluteal and scrotal wounds and secured with multiple skin staples. Multiple 5-0 chromic sutures were used to immobilize skin grafts over each scrotum ( Fig. 39.3 ). Standard dressings were applied to all skin graft sites and skin graft donor sites.










