Case 1
Clinical Presentation
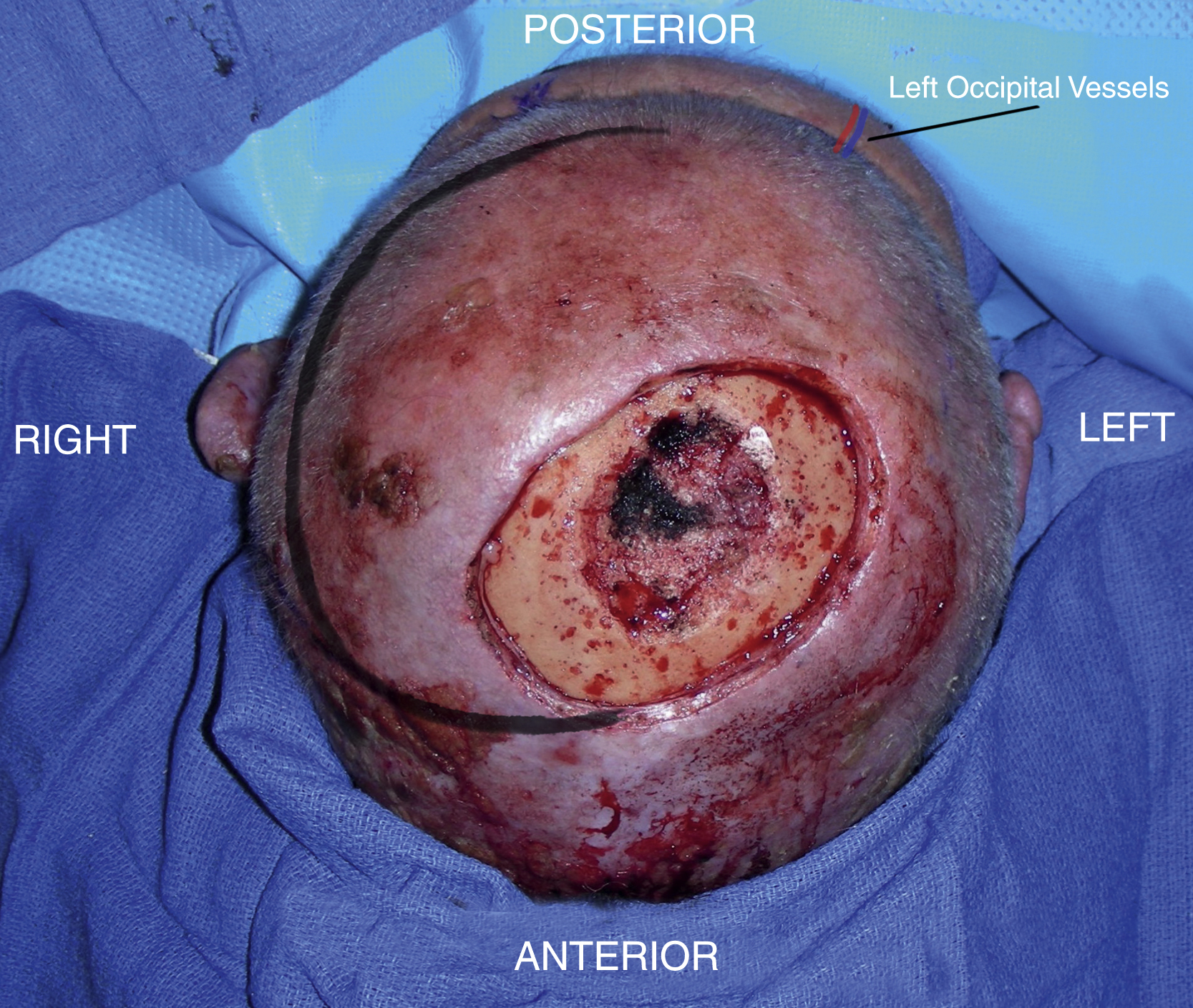
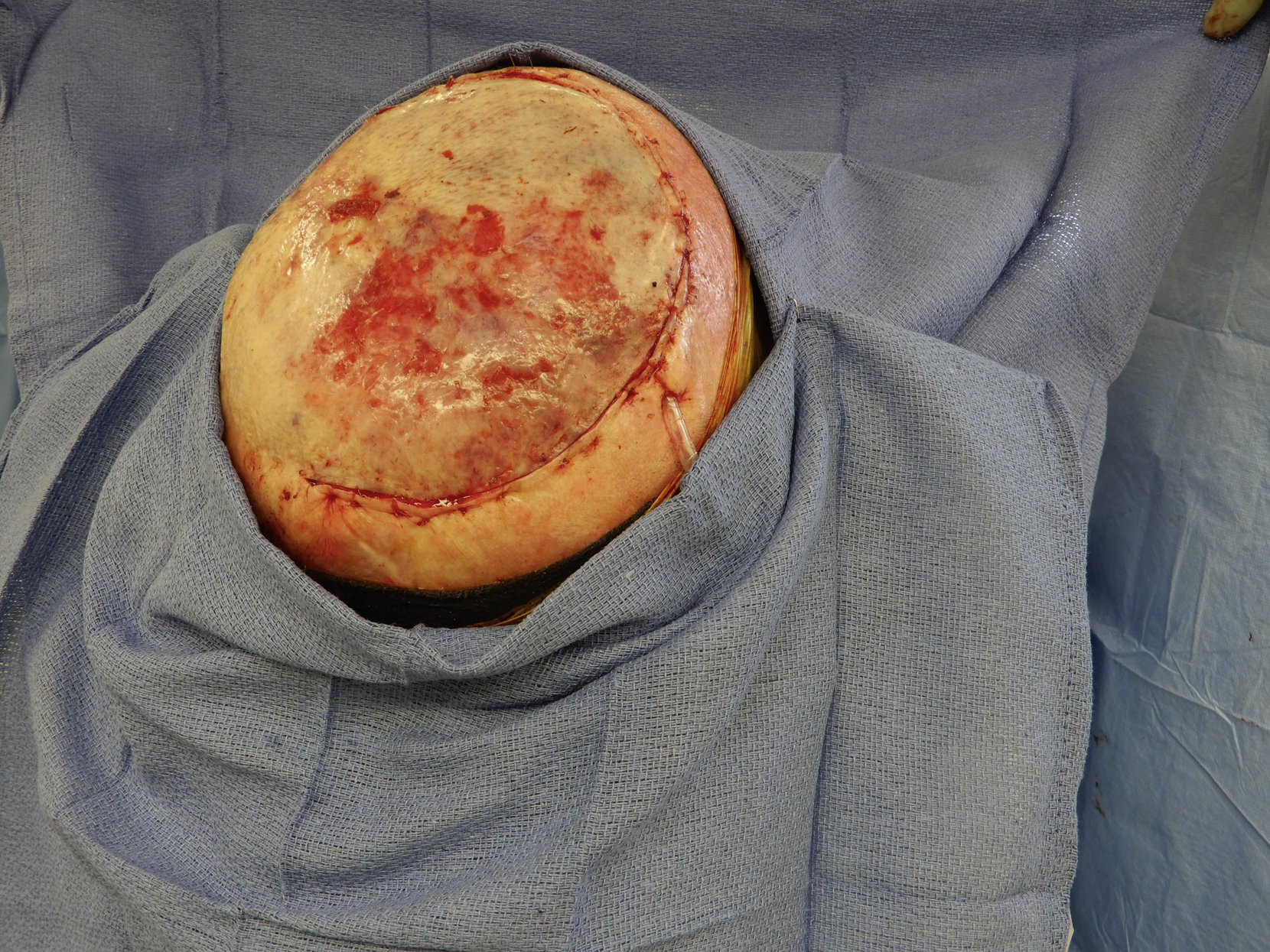
An 85-year-old White male with recurrent squamous cell carcinoma of his central scalp underwent additional surgical excision of the scalp including deep margin by the surgical oncology service. Once the peripheral and deep margin assessments by intraoperative frozen sections confirmed cancer was not present, the patient had a 10 × 7 cm full-thickness scalp defect with exposed skull. In the central part of the defect, a portion of the outer table of the skull was also removed ( Fig. 1.1 ).

Operative Plan and Special Considerations
After assessing his available scalp donor sites including the quality of his remaining scalp tissue and possible blood supply for the design of a large scalp rotation flap, it was decided that the flap could be designed based on the left occipital vessels.
Operative Procedures
The patient was placed in a prone position. The left occipital vessels were easily identified using a pencil Doppler and were used as the pedicle of a large posteriorly based scalp rotation flap ( Fig. 1.2 ). The flap design was marked and all the proposed scalp incisions were infiltrated with 1% lidocaine with 1:100,000 epinephrine.
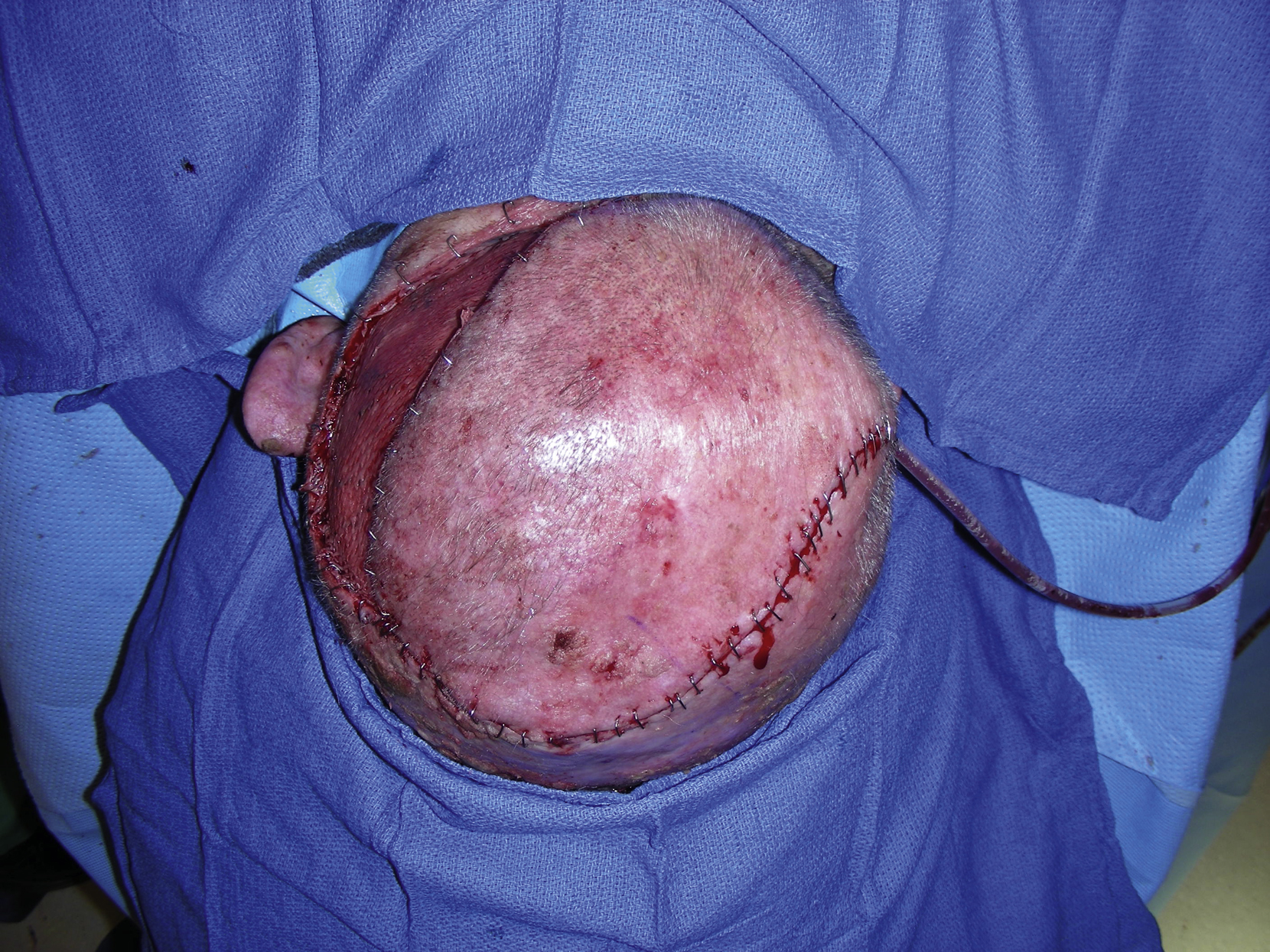
The procedure to free the periosteum from the subgaleal space was started within the scalp defect. The large scalp rotation flap was then elevated after incision of the scalp with knife and electrocautery. Elevation in the subgaleal space and an adequate rotation of flap to the defect were accomplished. During dissection, the contralateral side of the occipital vessel was divided in order to have more freedom of rotation. The flap was inset into the defect and secured temporarily with skin staples. The scalp flap donor site was covered with a meshed split-thickness skin graft harvested from the right lateral thigh ( Fig. 1.3 ). A 10 flat JP was inserted under the flap and the closure was performed in two layers. The deep dermal layer was approximated with several interrupted 3-0 Monocryl sutures and the skin was approximated with staples ( Fig. 1.4 ). The “dog ear” in the proximal flap was trimmed away from the flap and also approximated with skin staples ( Fig. 1.5 ). The pedicle vessels were easily identified with a pencil Doppler at the end of procedure. The skin graft site was covered with Xeroform, bacitracin ointment, fluffs, and a VAC sponge, which was secured with multiple skin staples.


Follow-Up Results
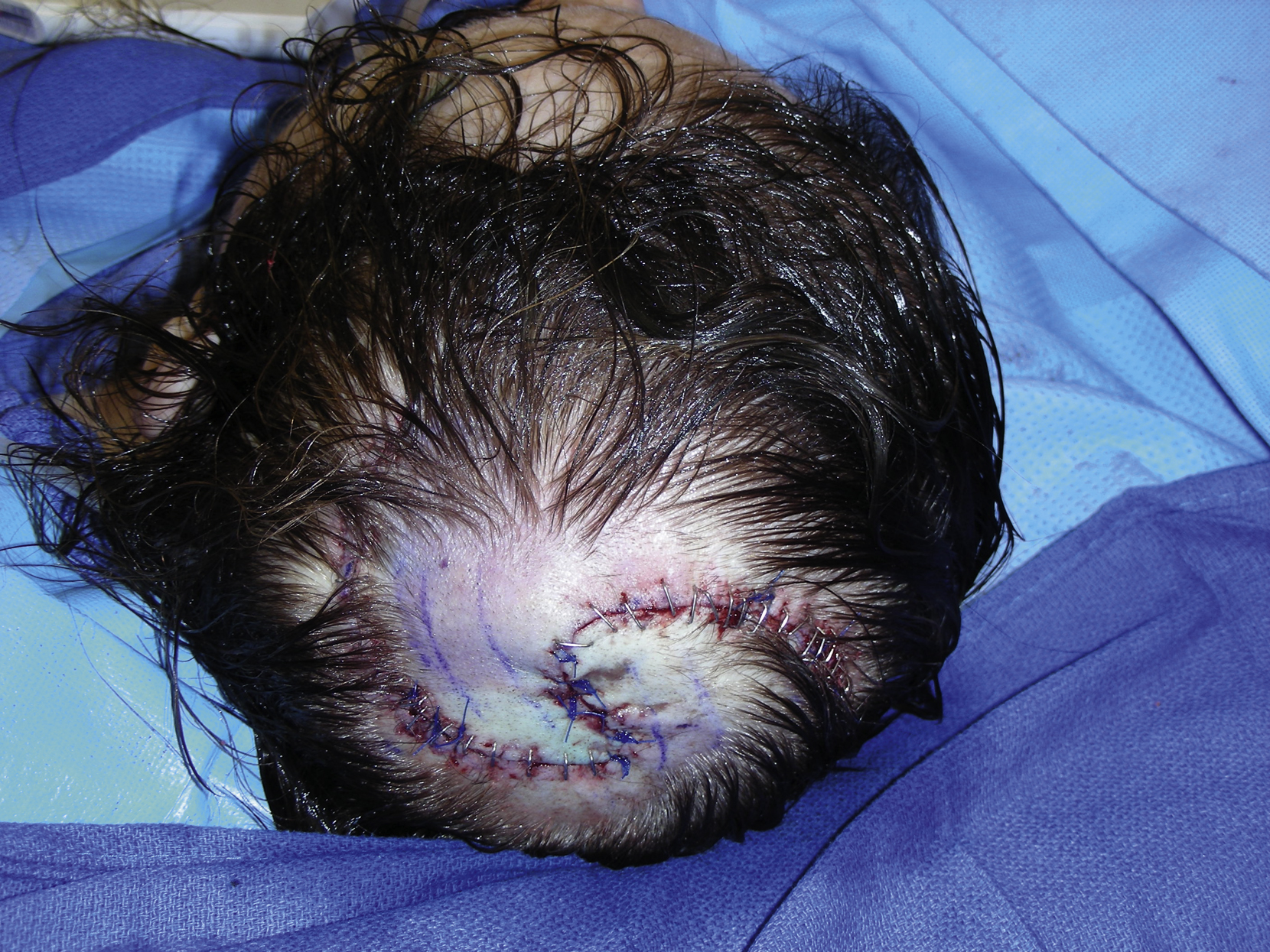
The patient did well postoperatively without complications related to the flap reconstruction. He was discharged from the hospital on postoperative day 5. The drain was removed during the first week after discharge. His scalp flap reconstruction and skin graft sites healed uneventfully ( Figs. 1.6–1.8 ).



Final Outcome
The patient’s scalp flap reconstruction and skin graft sites healed well. He returned to his normal life and activities and no local recurrence was found during a 1-year follow-up.
Pearls for Success
The design of a large scalp rotation flap should be based on a vascular pedicle that would provide a more consistent and reliable blood supply to the flap. Depending on the location of the scalp defect, such a design can be based on the location of any vessels that provide blood supply to the normal scalp. The pedicle vessels can be easily identified by a pencil Doppler. Scoring the galea under the flap may expand the flap tissue and make the flap inset easier and its closure less difficult. The excess tissue in the proximal aspect of the flap can be excised on the nonflap site and by doing so, the “dog ear” can be safely excised primarily without compromising the blood supply to the flap.
Case 2
Clinical Presentation
A 65-year-old White female had a scalp melanoma and underwent wide local excision of her occipitoparietal scalp lesion with a 1.5 cm margin after sentinel lymph node biopsy by the surgical oncology service ( Fig. 1.9 ). She had a 3.5 × 3.5 cm scalp defect down to the periosteum ( Fig. 1.10 ). The plastic surgery service was asked to perform a scalp reconstruction to repair the scalp defect.


Operative Plan and Special Considerations
Based on the size and shape of the scalp defect, bilateral rotation and advancement flaps (Yin-Yang flaps) were designed for this patient because the size of the defect was moderate and the shape of the defect was circular. In this way, her scalp defect could be closed primarily and no skin graft was needed. In addition, alopecia of the scalp after such a reconstruction could be avoided.
Operative Procedures
The bilateral scalp rotation and advancement (Yin-Yang) flaps were designed and marked ( Fig. 1.11 ). Each flap was designed large enough to close this circular defect without changing hairline style. All proposed incisions were infiltrated with 1% lidocaine with 1:100,000 epinephrine. The subgaleal dissection was then performed first inside the defect to raise more than half of the flap on each side. After that the incision was performed to raise the designed scalp flap on each side. Each flap was raised in half of the circular fashion so that it could be rotated and advanced into the defect and approximated in the midline of the circular defect. The extensive undermining was performed from the nonflap side scalp in order to close each flap’s donor site. The scoring under the galea was done so that a relatively tension-free closure could be achieved. Excess scalp tissue of each flap was trimmed and the donor site was closed with several interrupted skin staples. A 7-mm JP drain was inserted under both flaps and a final scalp closure was completed in two layers with interrupted 3-0 PDS sutures for deep closure and the rest of the incision with multiple skin staples or interrupted 3-0 Prolene sutures ( Fig. 1.12 ).

Follow-Up Results
The patient did well postoperatively without any complications related to the flap reconstruction. She was discharged from the hospital on postoperative day 2. The drain was removed during the first week follow-up visit. Her scalp flap sites healed well ( Figs. 1.13 and 1.14 ).


Final Outcome
The scalp flap sites healed well. The patient returned to her normal activities and no local recurrence was identified during follow-up.
Pearls for Success
Each Yin-Yang flap should be designed as a rotation/advancement flap that can cover half of the circular defect. The subgaleal dissection is performed first within the defect on each side to facilitate scalp flap dissection. Scoring the galea under each flap is helpful for a closure with less tension. Extensive undermining of nonflap scalp should be performed to allow primary closure of each flap’s donor site.
Case 3
Clinical Presentation
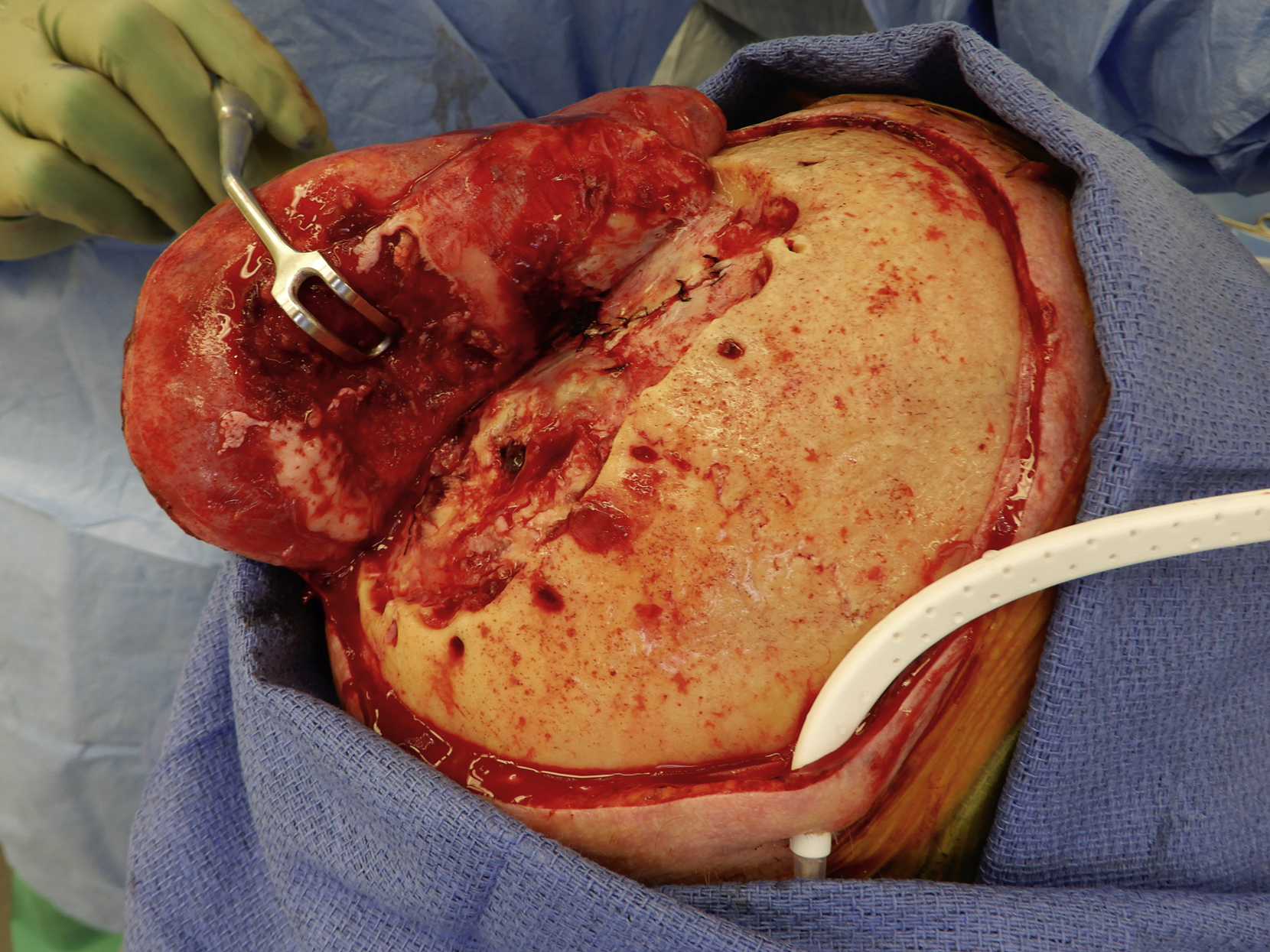
A 69-year-old White male with recurrent squamous cell cancer of his scalp had previous radiation and additional resection. The patient had developed a scalp wound with exposed skull. Several local reconstructive procedures were unsuccessfully attempted including Integra placement and local scalp rotation flap. He had a small scalp wound with exposed skull and had returned to his workplace in another state. One day ago, the patient was admitted to the neurosurgical service with subdural empyema. He was urgently taken to the operating room by our neurosurgeon for urgent debridement of the infected and necrotic skull and drainage of subdural empyema ( Fig. 1.15 ). The plastic surgery service was asked to perform an emergency scalp reconstruction after neurosurgical procedures in the same setting.

Operative Plan and Special Considerations
Because of the size of potential scalp defect after craniotomy by the neurosurgeon and clear clinical evidence of subdural infection as well as an emergency scalp reconstruction, a free latissimus dorsi muscle flap was selected for his scalp reconstruction. The latissimus flap is reliable and large enough to cover a large scalp wound. In addition, it has a long pedicle that can reach even facial vessels for microvascular anastomoses. A biological mesh, acellular dermal matrix (Strattice) was selected because of its biological nature and some rigidity.
Operative Procedures
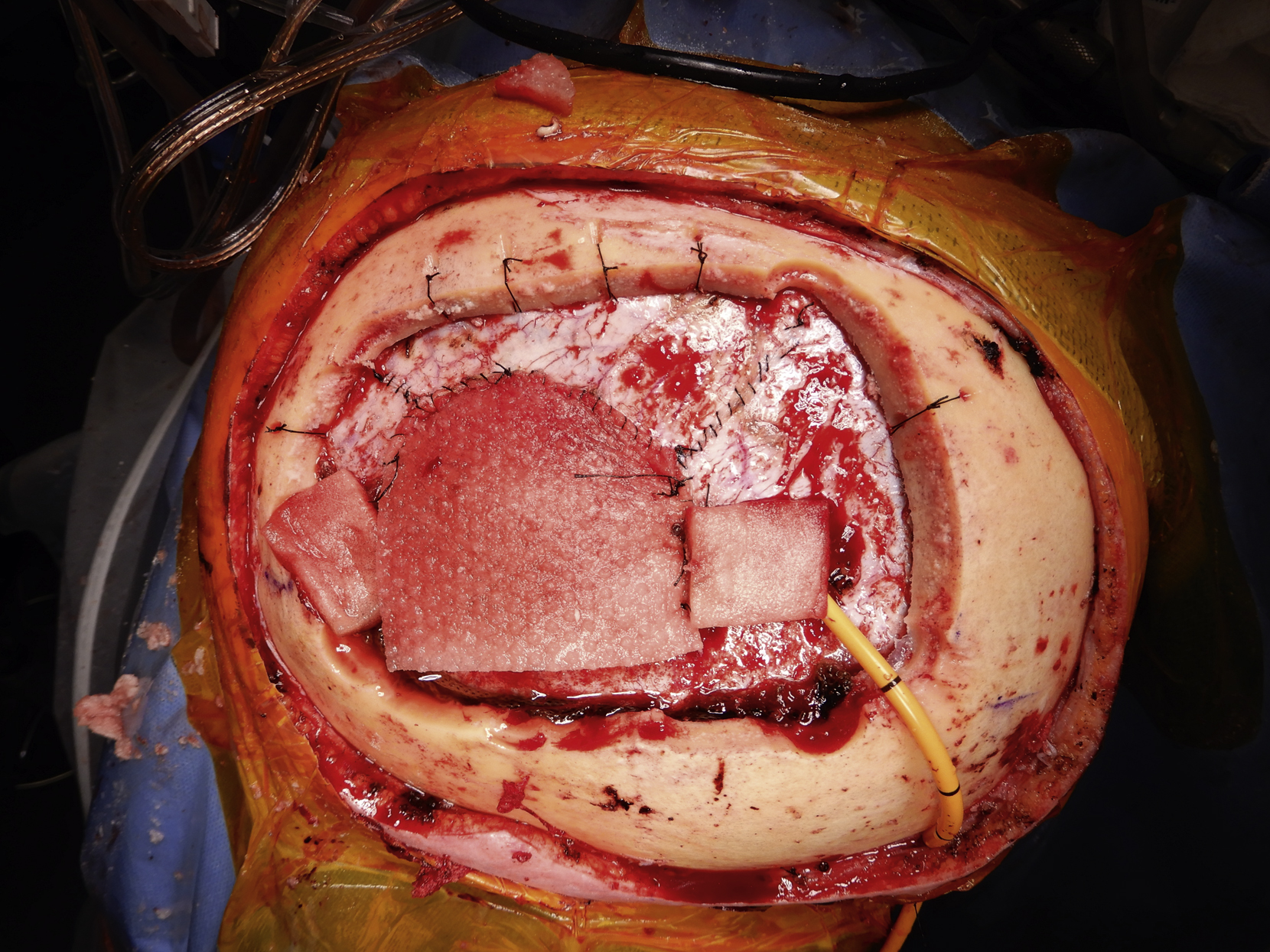
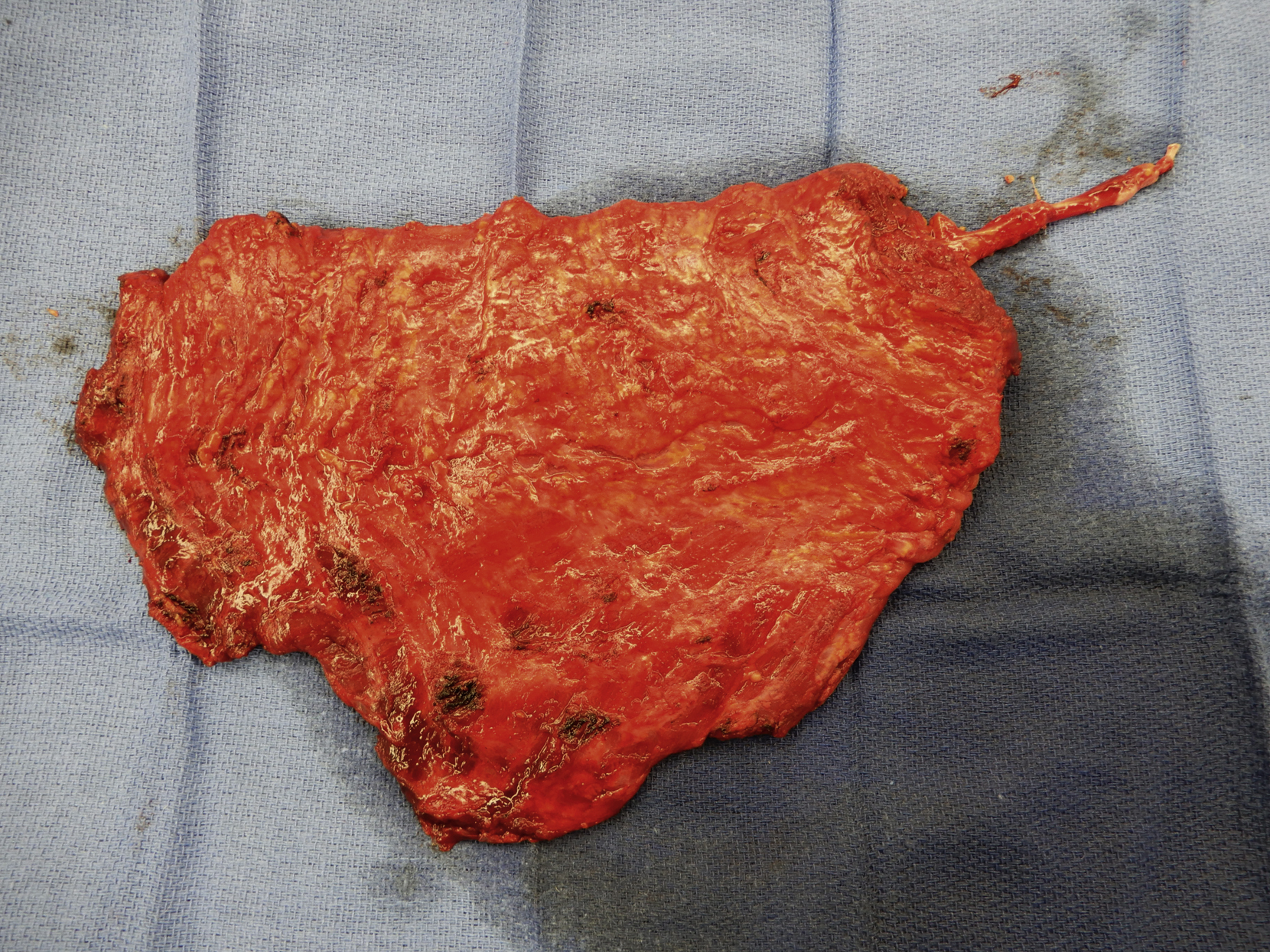
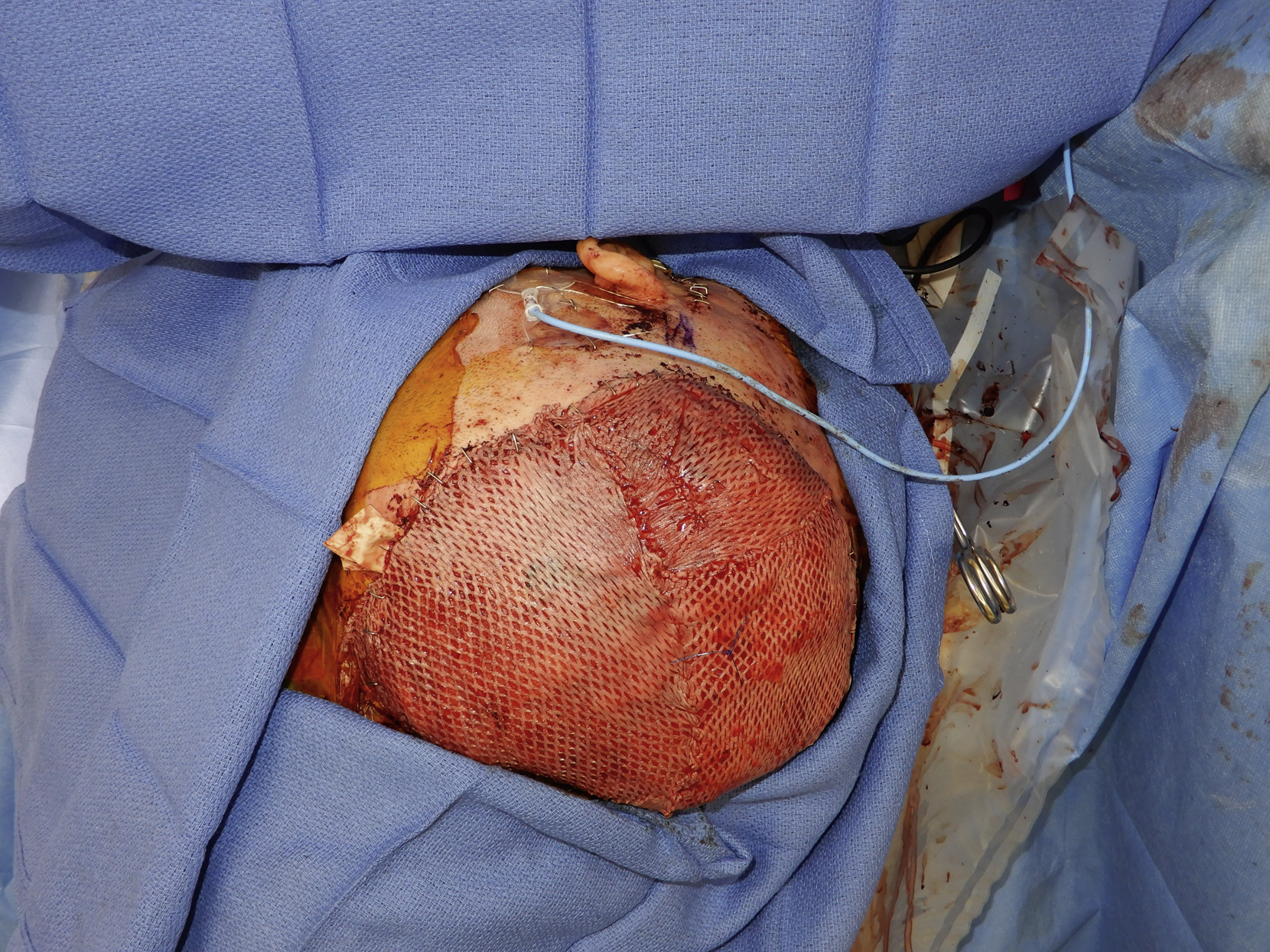
After all neurosurgical procedures were completed, the scalp wound measured 18 × 15 cm and the skull defect measured 11 × 7 cm ( Fig. 1.16 ). The skull defect was repaired first with Strattice. A large piece of Strattice was trimmed to 11 × 7 cm and with dermal side up, it was laid on the dural repair and secured with multiple 3-0 PDS sutures ( Fig. 1.17 ).

Based on duplex scan finding, the superior temporal artery and vein were dissected next. A 5-cm preauricular incision was made through the skin, the subcutaneous tissue, and the SMAS layer down to the superficial temporal vessels ( Fig. 1.18 ). Under loupe magnification, adequate length of both artery and vein were dissected free.

With an oblique incision, the latissimus dorsi muscle was first exposed ( Fig. 1.19 ). Once the lateral border of the muscle was identified, the dissection was done to elevate the muscle off the chest wall. The muscle’s attachment to the posterior iliac crest was divided under direct vision. The muscle was then elevated from its lateral, inferior, and also medial borders. The pedicle dissection was performed toward the axilla. The muscle attachment to the humerus was divided. With proper traction, the thoracodorsal nerve was dissected and divided, and the thoracodorsal artery and vein were dissected free and then divided with hemoclips from the subscapular vessels. The surgical dissection of a free latissimus dorsi flap was completed ( Fig. 1.20 ).

The thoracodorsal artery and vein of the flap was prepared under loupe magnification. The pedicle vessels were flushed with heparinized saline solution. The muscle flap was temporarily inset into the scalp defect and a tunnel was made between the left preauricular area and scalp wound. Both pedicle vessels were then tunneled under the scalp and placed near the superficial temporal vessels.
Under a microscope, the superficial temporal vessels and the pedicle vessels were prepared further. The superficial temporal artery and vein were divided with hemoclips at the level of the tragus. The arterial microanastomosis was performed in an end-to-end fashion with interrupted 8-0 nylon sutures. For the venous microanastomosis, a 3-mm coupler device was used for an end-to-end anastomosis. Once all clamps were released, the muscle flap appeared to be well perfused with no sign of venous congestion. A Cook Doppler probe was placed on the pedicle artery distal to the arterial anastomosis.
The preauricular incision was loosely approximated with several skin staples. The left latissimus dorsi muscle flap donor site was closed in two layers after placement of two drains.
The final inset of the latissimus dorsi muscle flap was performed after excess flap tissue had been excised. The flap was inset into the scalp defect with 3-0 Monocryl sutures in a half-buried horizontal mattress fashion. A Penrose drain was also inserted under the flap. A meshed split-thick skin graft was placed over the muscle flap ( Fig. 1.21 ).
Management of Complications
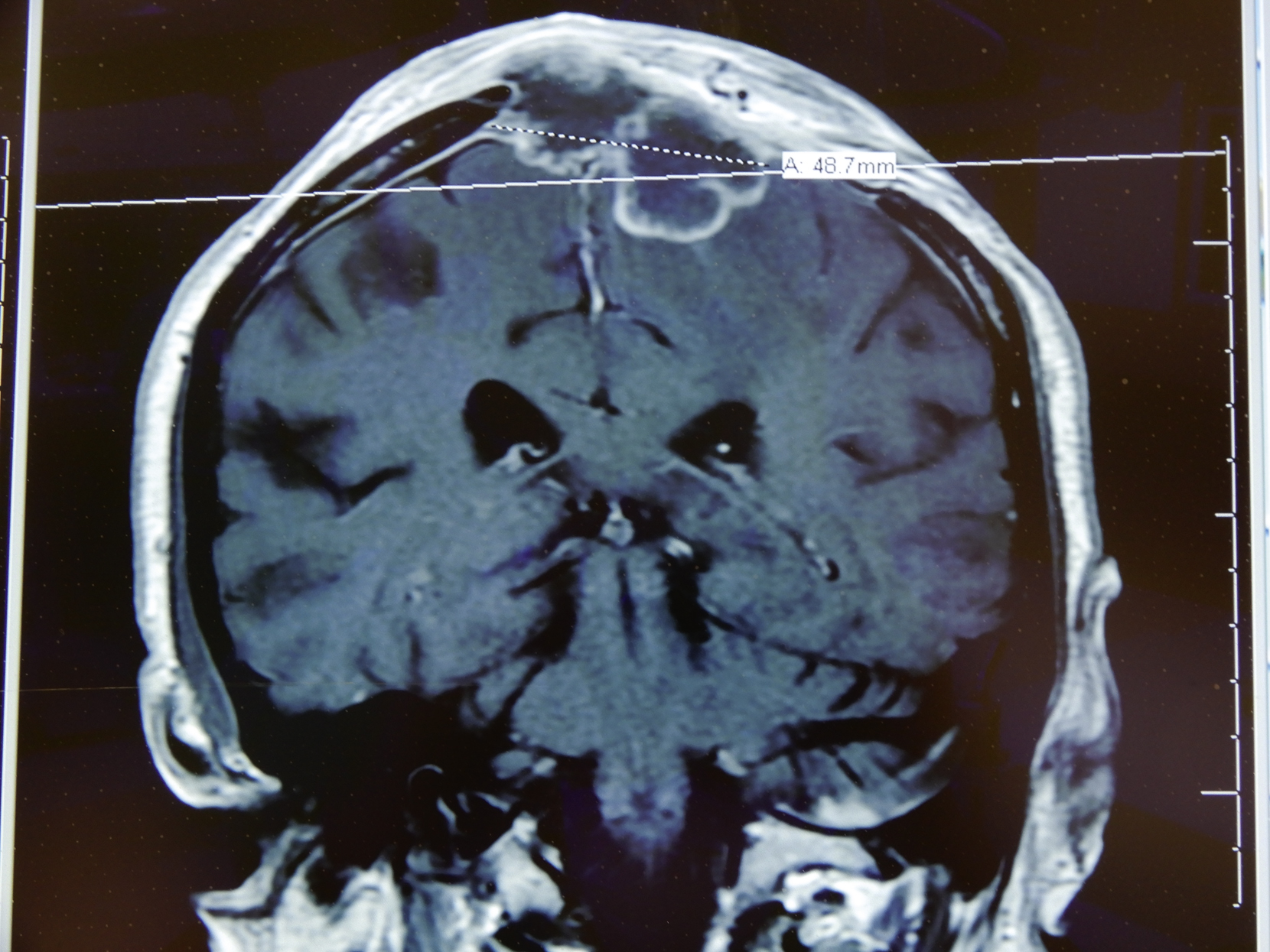
The patient did well postoperatively and there were no flap-related complications. He was discharged home on postoperative day 7. Both the scalp reconstruction site and the flap donor site healed nicely. Unfortunately, he developed recurrent subdural empyema 5 months later ( Fig. 1.22 ). He was urgently taken to the operating room by the neurosurgery service ( Fig. 1.23 ). The well-healed latissimus muscle flap was reelevated by the plastic surgery service and the subdural empyema was debrided and drained after removal of previously placed Strattice ( Fig. 1.24 ). The latissimus dorsi muscle flap was reinset with multiple half-buried horizontal mattress sutures ( Fig. 1.25 ).

Follow-Up Results
The patient did well again postoperatively without any complications related to the free latissimus dorsi muscle flap reconstruction. He was discharged from the hospital on postoperative day 5. The drain was removed during a follow-up visit. His scalp flap reconstruction site again healed well ( Fig. 1.26 ).

Final Outcome
The free latissimus dorsi muscle flap site healed well. The patient has resumed his normal activities and is followed by the neurosurgery service.
Pearls for Success
A free latissimus dorsi muscle is a large and reliable flap to reconstruct a large scalp defect. It has a long pedicle and can be harvested relatively fast in case an emergency free flap surgery is required. It should still be considered the flap of choice for scalp reconstruction when there is infection. Preoperative evaluation of the superficial temporal artery and vein with duplex scan should be performed if possible so that a better recipient vessel with adequate size of both artery and vein can be selected for relatively easier microvascular anastomoses. A near total flap reelevation could be safely performed with attention to the location of the pedicle vessels.
Case 4
Clinical Presentation
An 86-year-old White male had scalp squamous cell cancer and had previously undergone excision and radiation to the area. He had an ulcerated and radiated wound with exposed skull ( Fig. 1.27 ). The patient was referred by an outside hospital for definitive treatment. He was offered a two-stage procedure with the first stage to perform reexcision to remove all ulcerated and unhealthy-looking radiated scalp and to achieve a negative margin after resection ( Figs. 1.28 and 1.29 ). The second stage would be a free tissue transfer for reconstruction of the large scalp wound.

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


