Rehabilitative Burn Scar Management
Michael A. Serghiou
Jonathan Niszczak
KEY POINTS
A comprehensive program of rehabilitation is essential in the recovery of the burn patient.
Hypertrophic scar formation is one of the most prominent sequelae of burn injury; this chapter emphasizes the role of rehabilitation in managing hypertrophic scars that have the potential to limit function and result in catastrophic cosmetic outcomes for the burn survivor.
Focus in this chapter is placed on (a) the formation of hypertrophic scar; (b) scar assessment; (c) scar management to include pressure therapy, inserts, massage, and heat modalities; (d) orthotics; and (e) exercise.
Scar Formation
Wounds normally heal by forming scar to replace the injured or destroyed tissues at the injury site. This replacement scar tissue is much more restrictive than normal skin tissue, and often leads to complications in both functional movements and aesthetic appearance. Stedman1 defined scar as the fibrous tissue that replaces normal tissues that have been destroyed by an injury or disease. Historically, the earliest references to scarring are provided by Linares who credits the first full medical description of scars to Petz in 1790 (see Chapter 1).2
As the burn wound begins to heal or after skin grafting operations have been completed, scars begin to form. In general, the longer a wound remains open the higher the chances are for the development of hypertrophic scars (see Chapter 6).3,4 From a morphologic perspective, the two pathologic scar types (hypertrophic and keloid) differ in that keloid scars are mainly composed of thick type III collagen fibers with associated cyclooxygenase (COX)-2 overexpression, whereas hypertrophic scars are mainly composed of thin type I collagen fibers with a COX-1 overexpression (see Chapter 5).5 These two scar types differ in their timing of formation in that keloids tend to develop later in the healing process. Also, hypertrophic scars remain within the wound margins, whereas keloids proliferate outside of the wound margins.
Scar Hypertrophy
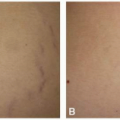
Scar hypertrophy has a prevalence of over 65% after burn injury.6 Factors that may contribute to the development of hypertrophic scars include: wound infection, the patient’s genetic makeup, repeatedly harvested donor sites, the patient’s age, chronic inflammation, location of the injury, and skin tension (see Chapter 7).7 An overgrowth of scar tissue is classified as hypertrophic or keloidal, both of which may be considered dermatoproliferative disorders of the skin.8 Hypertrophic scars are typically characterized as raised, red, rigid, painful, pruritic and may restrict joint motion or skin mobility within the confines of the burn.9 In contrast, keloid scars extend beyond the margins of the original injury advancing into the surrounding soft tissue and are somewhat less contractile in form (Fig. 19-1).9 Hypertrophic scars are not cosmetically appealing and can have a negative impact on a patient’s self-esteem and body image.10 Generally, the deeper the burn injury, the longer the inflammatory wound process, or the longer a wound remains unhealed, the greater the potential for formation of hypertrophic scars (see Chapters 6, 8, and 9).3,4,11 Burn scar contractures may occur because of the effect of myofibroblasts and free actin in the scar.12 Contractures are characterized as either intrinsic (loss of tissue in the injured area with subsequent distortion of the involved anatomic part) or extrinsic (loss of tissue is at a distance from the affected area, but the distorted structures are not injured themselves).13 As the wound heals, collagen fibers are deposited to bridge the wound, forming an immature (active) scar.14,15,16 Extensive study with well-defined, randomized controlled trials is lacking in understanding hypertrophic scar development in part because of the limited consensus on an adequate animal model of abnormal scarring.8 However, progress continues to be made in understanding and potentially unlocking the scar development cascade, including the signal mediator transforming growth factor β, the overproduction of extracellular matrix, and keratinocyte signal expression research.17,18,19
Scar Assessment
It is critically important for a burn rehabilitation specialist to assess the burn scar carefully before initiating
management (see Chapter 28). Burn scar assessment, even though time consuming, is vital in the rehabilitative process as it relates to functional and cosmetic outcomes. Several scar assessment tools and scales have been developed to quantify the burn scar and can be used to determine the effectiveness of scar management protocols and track outcomes in rehabilitation. Some of these scar assessment devices are objective (provide quantitative measurements of scar parameters/characteristics) and some are more subjective (provide qualitative measurement of the scar and are observer dependent). Individual tools designed to assess the burn scar specifically address various scar parameters including pliability (Pneumatonometer,20,21 Cutometer,22,23 Tonometer,24,25 and Extensometer26), firmness (Durometer27), color (Chromameter, DermaSpectrometer, Mexameter, and Colorimeter28), thickness (Ultrasound scanners23,29,30,31), tissue perfusion (Laser Doppler imaging [LDI]32,33,34,35), and three-dimensional topography.32,36,37 These tools are considered more objective in assessing the burn scar, although their validity and reliability in assessing all scar types have been questioned.
management (see Chapter 28). Burn scar assessment, even though time consuming, is vital in the rehabilitative process as it relates to functional and cosmetic outcomes. Several scar assessment tools and scales have been developed to quantify the burn scar and can be used to determine the effectiveness of scar management protocols and track outcomes in rehabilitation. Some of these scar assessment devices are objective (provide quantitative measurements of scar parameters/characteristics) and some are more subjective (provide qualitative measurement of the scar and are observer dependent). Individual tools designed to assess the burn scar specifically address various scar parameters including pliability (Pneumatonometer,20,21 Cutometer,22,23 Tonometer,24,25 and Extensometer26), firmness (Durometer27), color (Chromameter, DermaSpectrometer, Mexameter, and Colorimeter28), thickness (Ultrasound scanners23,29,30,31), tissue perfusion (Laser Doppler imaging [LDI]32,33,34,35), and three-dimensional topography.32,36,37 These tools are considered more objective in assessing the burn scar, although their validity and reliability in assessing all scar types have been questioned.
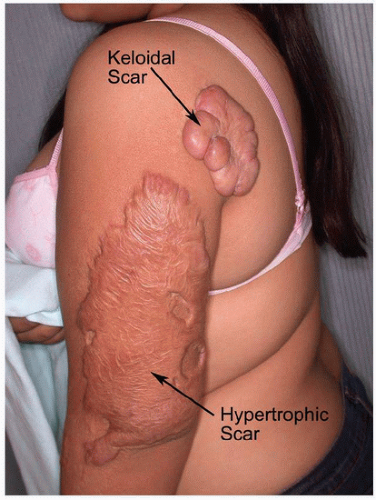 FIGURE 19-1 Hypertrophic scar and keloid scar. |
Several scar assessment scales have been developed to provide a more comprehensive way to assess the burn scar. The Vancouver Burn Scar Assessment (VBSA) developed by Sullivan et al.38 in the 1990s is currently the most frequently utilized burn scar assessment scale, even though it was originally developed over 25 years ago. The VBSA subjectively assesses physical scar parameters that relate to the healing and maturation of scars. These include scar pigmentation, vascularity, pliability, and height.39 Through the years other authors have attempted to improve upon the original VBSA, with some success highlighted in the publications of Baryza and Nedelec.40,41,42 The VBSA is considered to be subjective and it is utilized to track the maturation progress of small linear scars within an individual, rather than between individuals. Other prominent scar assessment scales include the Patient and Observer Scar Assessment (POSAS) and the Manchester Scar Scale (MSS). Fearmonti et al.43 have described and compared various scar scales and individual scar assessment tools highlighting their limitations. To date, a comprehensive, reliable, and valid burn scar assessment that looks into all scar parameters relevant to burn rehabilitation remains elusive.44 Individual scar assessment tools that assess single scar parameters may in some cases show some validity and reliability. However, they are generally expensive and their use in burn rehabilitation is often impractical.43,45
Rehabilitative Management of Scars
Despite significant improvements in medicine in recent years, hypertrophic scars remain very problematic and are difficult to manage. Improvements in medical life-saving procedures have improved the survivability of extensive total body surface area (TBSA) burns, so it is imperative that rehabilitative techniques also advance to achieve optimal functional and aesthetic outcomes. To that extent, it is imperative that scar management should be a continual process that is reviewed during every aspect of wound maturation. The best treatment for scars is to prevent their appearance, so vigilance is key. Even though the mechanism of scar maturation is not yet fully understood, clinically most rehabilitation specialists treat hypertrophic scars through combinations of the following modalities—pressure therapy, exercise/range of motion (ROM), inserts, splints, massage, heat modalities, and silicones.
Pressure Garment Therapy
Pressure therapy has long been utilized to manage scars that are red, thick, and elevated and are widespread in nature. Pressure therapy, which should be instituted early on in the burn scar maturation process, is by far the most widely used and recognized modality. Means of pressure therapy include pressure garments, inserts, and conforming orthotics. The first medical reference to describe the use of pressure for the treatment of immature scars was written by Johnson in 1678 referencing the work of Ambroise Paré in the 16th century.2 Other important historical events described by Linares include the use of elastic bandages in 1860, pressure provided by plaster casting in 1881, and the use of traction to treat scars in 1902. Linares’ historical review also includes descriptions of Nason’s work in 1942 in which he observed that pressure exerted onto the injured skin by undergarment elastic produced ischemia, which in turn stopped the overproduction of scar tissue.2,46
The use of pressure in effectively depressing scars was well documented by Silverstein and Larson in the 1970s; their observations and studies led to the development of pressure garments that today appear to be the “gold standard” in managing developing scars. When an active scar is compressed it blanches, which indicates decreased blood flow in the area.47 Although the mechanism of action of pressure garments has not been fully elucidated, it has been hypothesized that less blood leads to decreased oxygenation in the tissues, which in turns leads to decreased collagen production, establishing a balance between collagen synthesis and collagen breakdown (lysis). When a balance in
the production and breakdown of collagen is reached, the resultant scar appears flatter.48 Kealey et al.49 conducted a prospective randomized study to investigate the efficacy of pressure garments in patients who survived burn injuries. In this study, patients were randomly assigned to receive either pressure garments or no pressure garments. Assessment of scar maturity included use of the VBSA. The results of this study revealed no significant differences between the two groups when age, body surface area burned, length of hospital stay, or time to wound maturation were compared. Other studies have reported problems related to lack of adherence due to the application schedule, discomfort, blistering, ulceration or scar breakdown, swelling of extremities, and skeletal and dental deformity due to excessive pressures. These issues can lead to significant side effects, poor compliance, and even permanent deformity.46,47,49,50,51,52,53,54
the production and breakdown of collagen is reached, the resultant scar appears flatter.48 Kealey et al.49 conducted a prospective randomized study to investigate the efficacy of pressure garments in patients who survived burn injuries. In this study, patients were randomly assigned to receive either pressure garments or no pressure garments. Assessment of scar maturity included use of the VBSA. The results of this study revealed no significant differences between the two groups when age, body surface area burned, length of hospital stay, or time to wound maturation were compared. Other studies have reported problems related to lack of adherence due to the application schedule, discomfort, blistering, ulceration or scar breakdown, swelling of extremities, and skeletal and dental deformity due to excessive pressures. These issues can lead to significant side effects, poor compliance, and even permanent deformity.46,47,49,50,51,52,53,54
On the other hand, studies have also reported the benefits of pressure garments.55,56,57 Several excellent reviews on the efficacy, or lack of efficacy, of pressure garments in the management of hypertrophic burn scars have appeared recently in the literature.58,59 One reason for the absence of strong, undisputed evidence in the efficacy of pressure garments is that garments must be worn continuously for at least 23 hours a day, making adherence difficult to measure.2,52,59 Furthermore, the optimal therapeutic pressure required to depress hypertrophic scars is not yet known.52,60,61,62 The debate regarding the effectiveness of pressure garments continues to this date. Until more definitive evidence is gathered to support the use of pressure garments or prove them ineffective in managing scars, pressure therapy in the form of elastic garments will continue to be a standard component of scar management. It should be noted that all pressure garment studies conducted thus far do not include the examination of burns over joints, nor do they include burns of the hands, neck, and face. It would be unethical to withhold pressure treatment on a patient’s face or the other body surfaces mentioned above just to confirm if pressure works or not.46
As long as the scars are active they may be influenced by pressure therapy. However, not all burn scars require pressure. Patients with burn wounds that heal within 7 to 14 days frequently do not need pressure therapy. Those patients whose wounds heal within 14 to 21 days are closely monitored for pressure therapy needs, and may be advised to use pressure garments prophylactically. A wound that heals after 21 days will generally require the use of pressure garments.48 The correct amount of pressure required to suppress hypertrophic scar formation has not yet been determined. Pressure of as little as 10 mm Hg may be effective in remodeling the scar tissue over time. Pressures over 40 mm Hg, however, may be destructive to tissues and cause paresthesias.47 Traditional forms of pressure therapy include the use of elastic bandages directly applied on the newly healed skin, or on top of the burn dressings. The use of conforming thermoplastics along with elastic bandages (Fig. 19-2) may also be utilized as means of early pressure therapy.63 Once the wounds are almost or completely closed, tubular elastic bandages such as Tubigrip (Mölnlycke Health Care, Göteborg, Sweden) may be utilized. These tubular elastic bandages are offered in different sizes and accommodate all anatomical circumferences (Fig. 19-3). Care should be taken in applying these tubular bandages so that the fragile skin or the freshly applied skin grafts do not sheer, or the minimal dressing underneath is not disturbed. The burn therapist should be aware that these tubular bandages are materials made of a single elastic thread spiraling through the weave of the fabric, and disturbance of the continuous elastic by cutting holes into it will alter the pressure gradient provided by these materials. The tubular elastic bandages should be doubled over the skin surface area treated in order to provide adequate pressure.46,64
 FIGURE 19-2 Elastic bandage provides approximately 10 to 12 mm Hg pressure. |
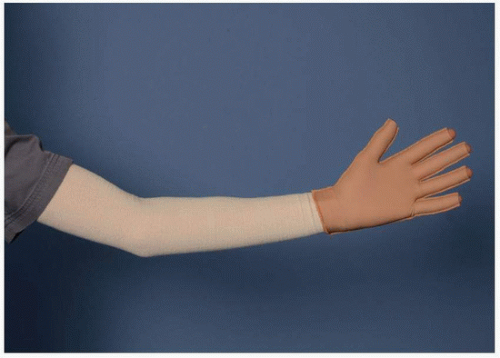 FIGURE 19-3 Tubular elastic bandage (Tubigrip) provides approximately 15 to 17 mm Hg pressure. |
Early pressure application over the hand and digits can be accomplished by the use of thin, elastic, and self-adherent wraps such as Coban (3M, St. Paul, Minnesota) (Fig. 19-4). This form of pressure is excellent for adult and pediatric patients for controlling edema and aids in the early scar management of hands when the shearing forces of a glove cannot be tolerated. Small children are excellent candidates for Coban gloves versus a garment glove because of compliance issues, comprehension of instructions in assisting with the application of a custom glove, and difficulties in obtaining accurate measurements for a custom glove. Coban may be applied over the burn dressings or directly onto the healed digits. The burn therapist needs to be aware that if Coban is wrapped too tightly it may
deform the interosseous structures of the healing hand. However, if Coban is wrapped too loosely it may encourage swelling of the hands when used in combination with arm elastic garments.
deform the interosseous structures of the healing hand. However, if Coban is wrapped too loosely it may encourage swelling of the hands when used in combination with arm elastic garments.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


