Key Points
- ▪
The single most important role of chest radiography in valvular disease is to establish or document the presence of heart failure.
- ▪
The different valvular lesions reveal themselves through their respective influence on chamber dilation that is specific to the disorder.
Acquired Valvulopathies
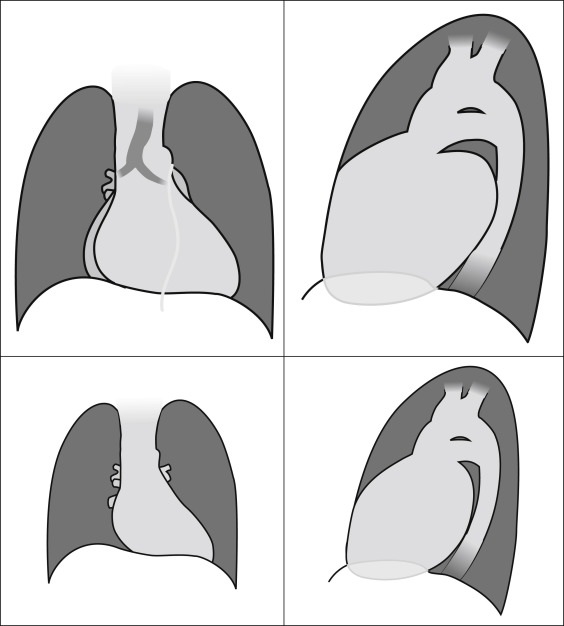
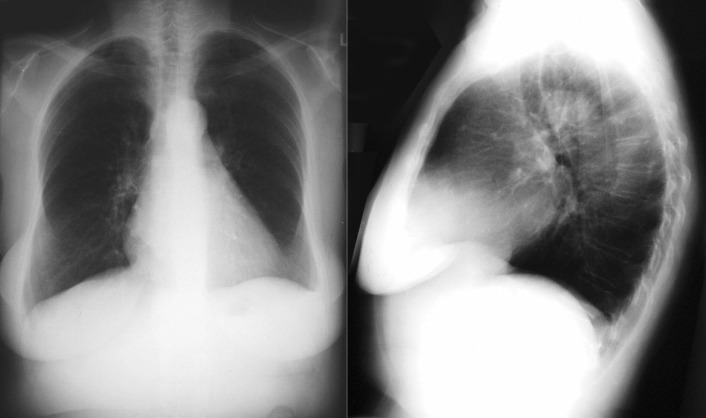
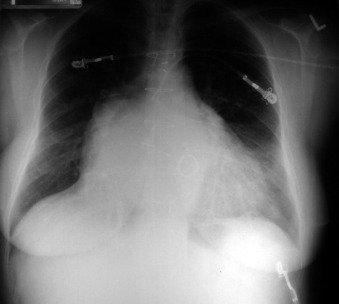
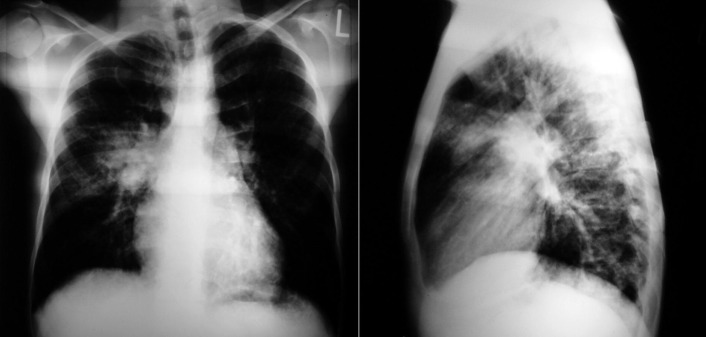
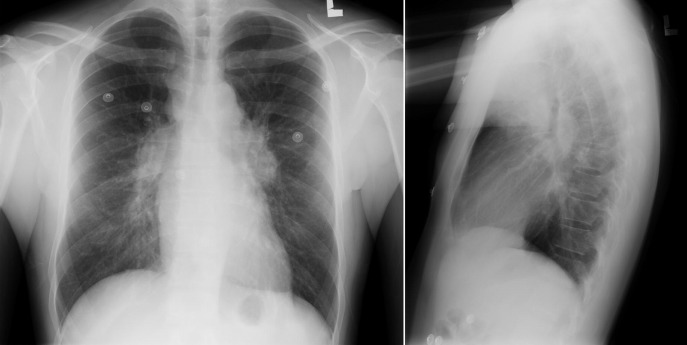
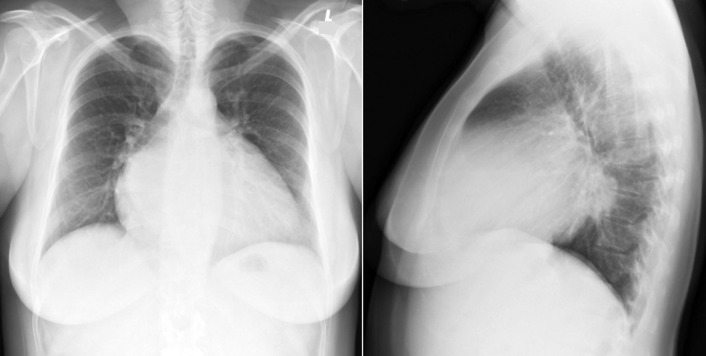
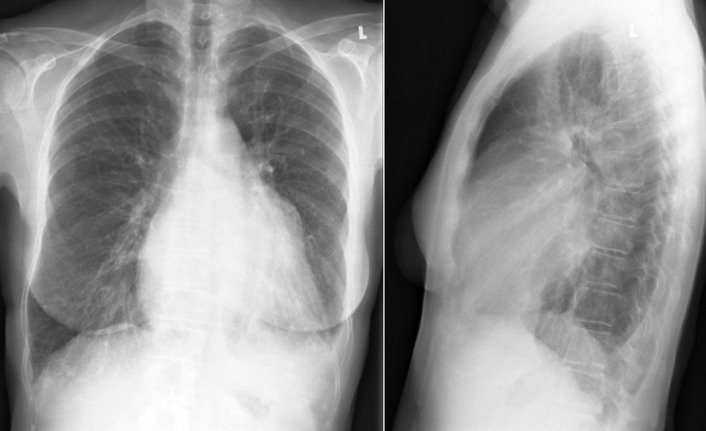
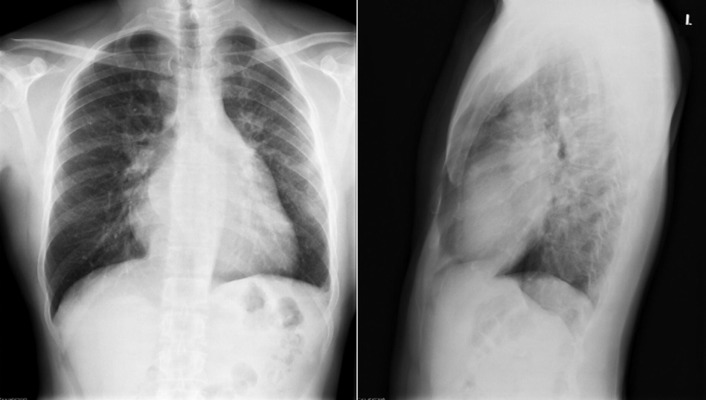
Mitral Stenosis
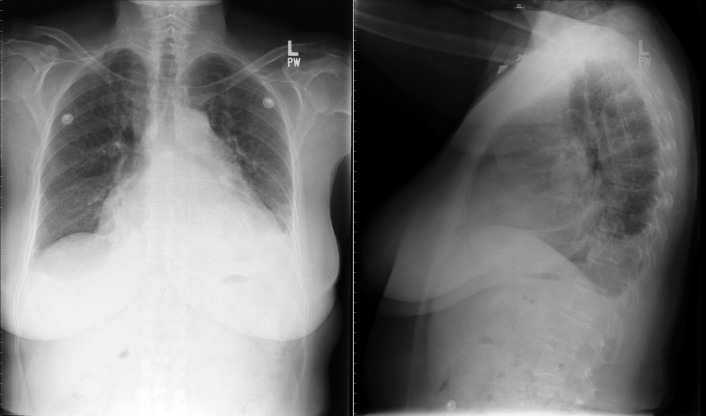
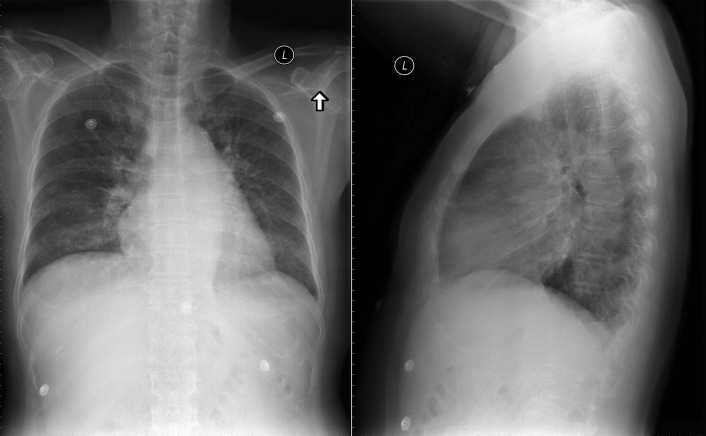
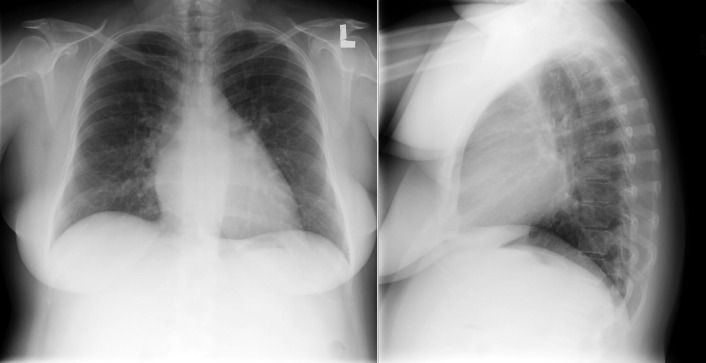
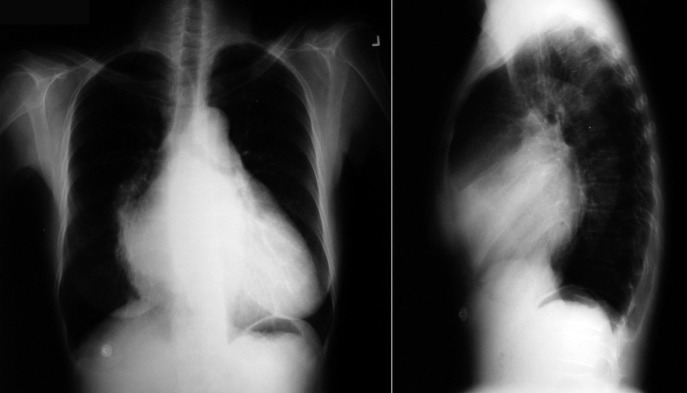
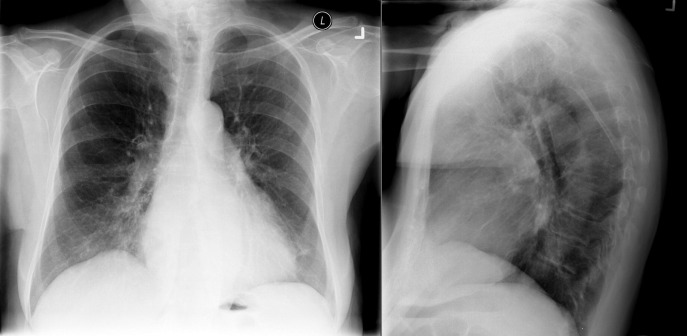
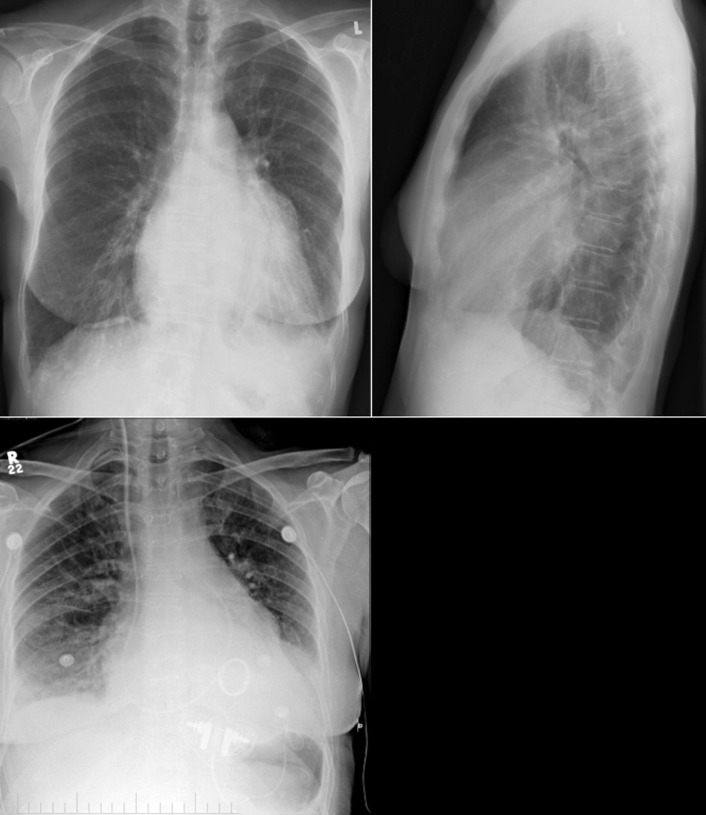
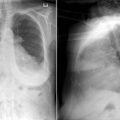
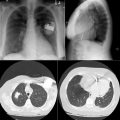
The radiographic findings of mitral stenosis ( Graphic 15-1 ; Figs. 15-1 to 15-16 ) reflect the pressure overload of the left atrium and pulmonary veins, and later of the right heart. As well, the commonly associated chronic atrial fibrillation contributes to (bi)atrial dilation. Associated rheumatic valvular lesions such as mitral regurgitation, tricuspid regurgitation, aortic insufficiency, and aortic stenosis/aortic insufficiency are common, and they alter the appearance of the heart.



Related posts:
 Radiographic Findings by Diagnosis: Cardiomyopathies
Radiographic Findings by Diagnosis: Cardiomyopathies
 Radiographic Findings by Diagnosis: Coronary Artery Disease–Complications of Infarction
Radiographic Findings by Diagnosis: Coronary Artery Disease–Complications of Infarction
 Radiographic Findings by Diagnosis: Pericardial and Pleural Diseases
Radiographic Findings by Diagnosis: Pericardial and Pleural Diseases
 Central Venous and Pulmonary Artery Catheters
Central Venous and Pulmonary Artery Catheters
 Tubes and Drains
Tubes and Drains
 Pacemakers and Implantable Cardioverter Defibrillators
Pacemakers and Implantable Cardioverter Defibrillators
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


