Key Points
- ▪
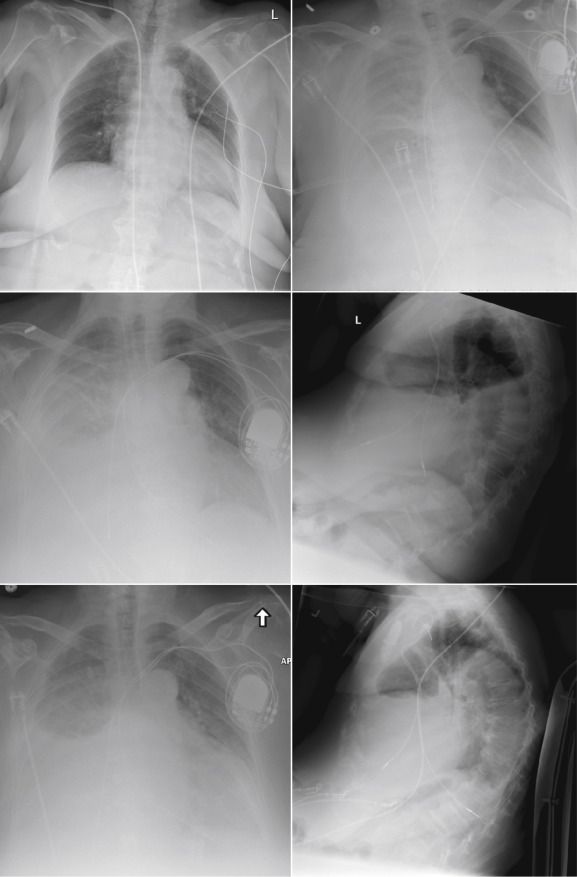
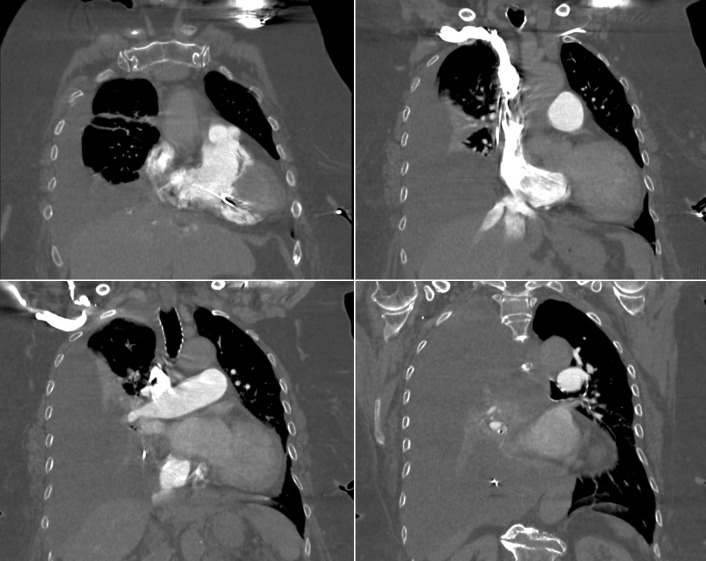
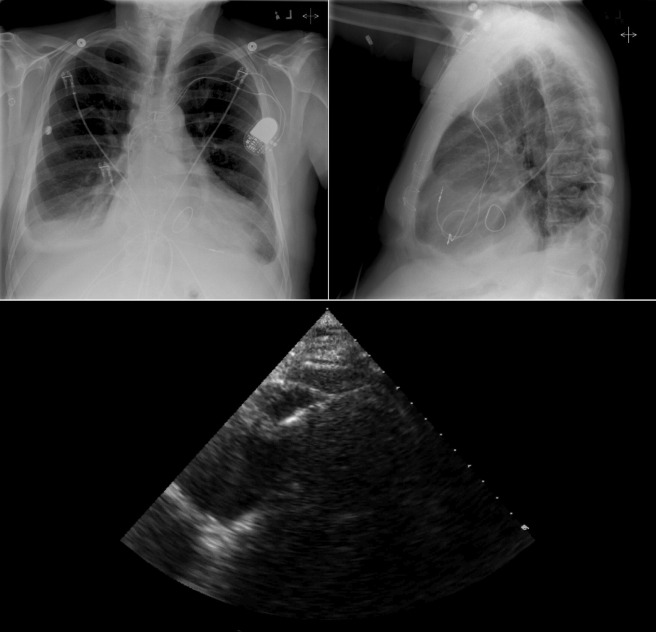
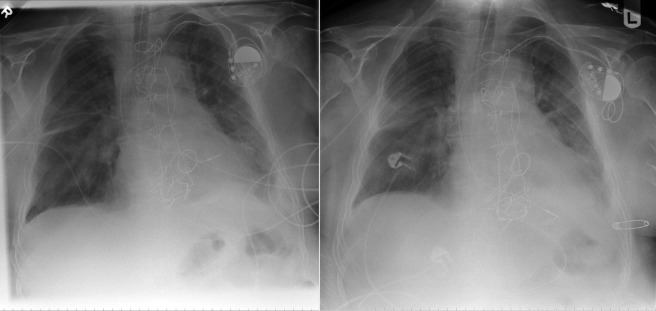
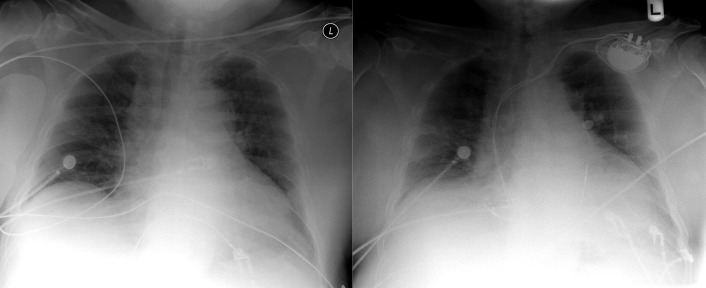
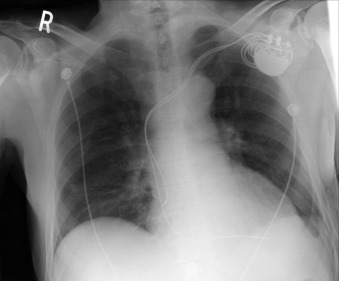
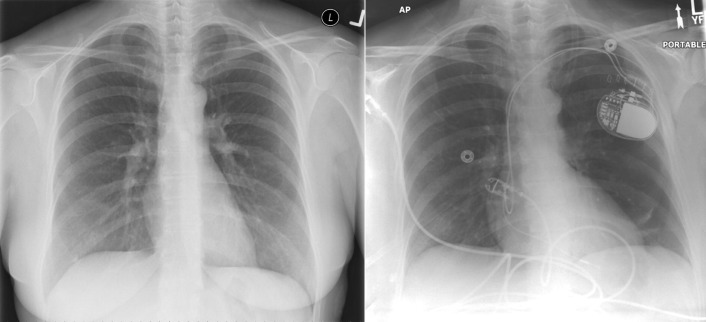
Chest radiography has a standard role in the identification of several potential complications such as pneumothorax, hemothorax, and several forms of malposition after insertion of pacemakers, implantable cardioverter defibrillators (ICDs), and cardiac resynchronization therapy devices.
- ▪
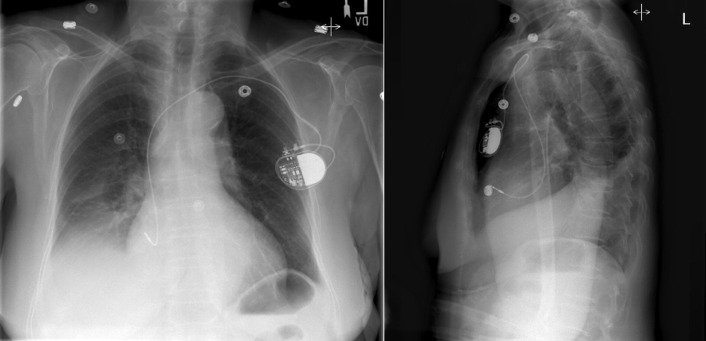
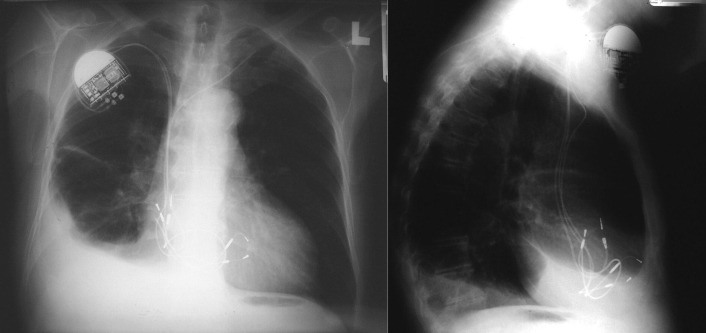
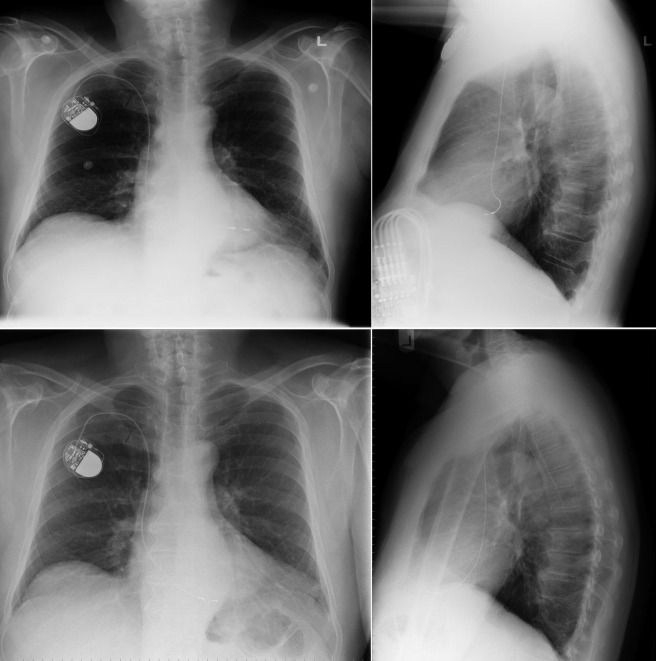
Pacemaker leads are apparent, and ICDs are more obvious because of their larger coils. Coronary sinus leads for cardiac resynchronization therapy are finer leads.
Endocardial Pacer Leads
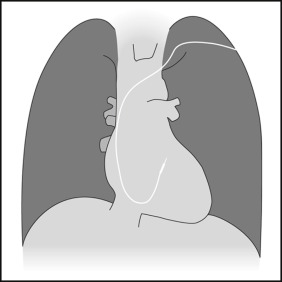
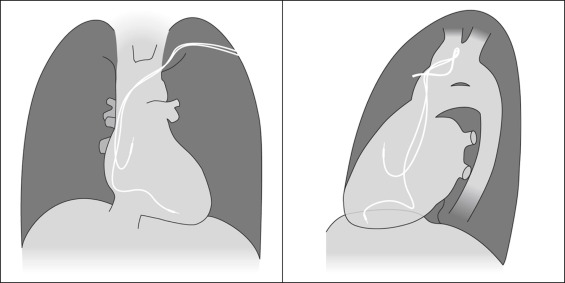
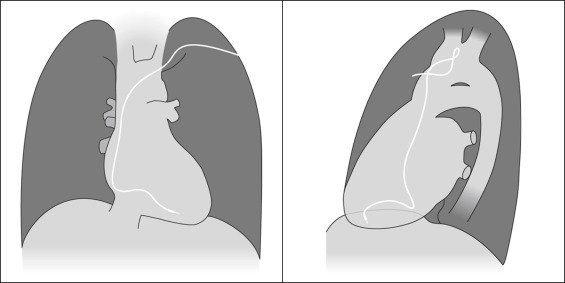
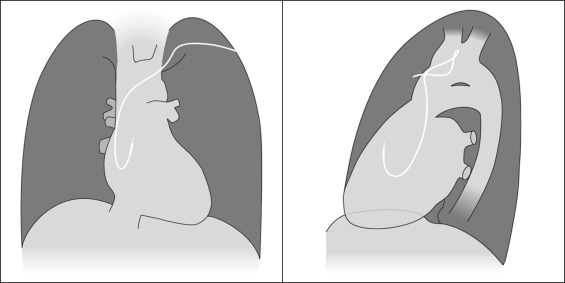
The position and integrity of endocardial pacer leads should be verified, especially when pacemaker dysfunction is clinically suspected ( Graphics 23-1 to 23-4 ; Figs. 23-1 to 23-15 ).The most common cause of pacemaker dysfunction that is apparent on the chest radiography is distal lead displacement/misplacement.
- □
With a right atrial lead , the tip should be in the right atrial appendage.
- □
With a right ventricular lead , the tip should lie anteriorly at the apex of the heart.