Abstract
Purpura is an important physical finding, both for serious and incidental disease. The ability to rapidly sort through diagnostic possibilities depends on recognition of morphologic subsets of purpura, and knowing the differential diagnoses relevant for each subset. Understanding the likely pathophysiology of each syndrome and narrowing the likely diagnostic differential by subsetting by morphology, number, and distribution of purpuric lesions enable efficient testing and confirmation of diagnosis.
Keywords
Ecchymosis, Microvascular occlusion, Palpable purpura, Petechia, Retiform purpura, Simple hemorrhage, Vasculitis
- •
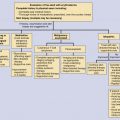
Purpura has an extended and complex differential diagnosis, but can be sorted into three main pathophysiologies: simple hemorrhage, inflammatory (vessel-directed) hemorrhage, and microvascular occlusion.
- •
Recognition of patterns of morphology, number and distribution can rapidly narrow the diagnostic possibilities enabling a focused and efficient work-up to confirm the diagnosis.
- •
The differential diagnosis of cutaneous microvascular occlusion only minimally overlaps with traditional differential diagnosis of deep venous thrombosis or pulmonary emboli.
- •
Distinguishing inflammatory hemorrhage from microvascular occlusion can be difficult because of the clinical and histologic evolution of lesions, but is critical to proper treatment.
Purpura
The clinical finding of purpura is associated not only with some of the most rapidly life-threatening illnesses known, but also with some of the most common and benign conditions of daily life. Although the evaluation of a patient with purpura can occasionally be complicated, in many cases a good history and physical examination in conjunction with simple tests may be all that is required.
Purpura is a generic term for visible hemorrhage in the skin and mucous membranes. More specific terms describe particular types of purpura, and subtyping purpura is essential for an efficient diagnosis. The term petechia generally implies an area of hemorrhage 4 mm or less in diameter ( Fig. 15-1 ). An ecchymosis is a deep reddish-blue, purplish, or blue-black macule, usually at least 1 to 1.5 cm in its greatest dimension. As used in this chapter, the terms petechiae and ecchymoses are also restricted to lesions that are macular (nonpalpable) and without a blanchable component, consistent with simple hemorrhage. A contusion is a major trauma-induced lesion that may be purpuric, and frequently has trauma-related soft-tissue swelling and tenderness. The traditional term palpable purpura is best applied to a lesion that is partially but not completely blanchable, implying a component of early inflammation. Retiform or branching purpura is a term that describes hemorrhage, which may be inflammatory or noninflammatory, but is characterized by a distinctive shape, with branching or reticulate patterning of the whole lesion or of its edges. Noninflammatory retiform purpura most characteristically is due to microvascular occlusive disease in the skin.

Pathogenesis
Cutaneous hemorrhage may result from intravascular, vascular, and extravascular causes, and many differential diagnoses use this approach. It may be more helpful to approach the bedside diagnosis of purpura from a morphologic perspective, using the distinctive morphology of purpura to decide between three possible broad pathogenic mechanisms: simple hemorrhage, inflammatory hemorrhage (vessel-directed inflammation), or occlusive hemorrhage with minimal inflammation. This differential applies to lesions of purpura that are primary, meaning that the mechanism of the lesion is also the sole cause of the hemorrhage. Clinical judgment is needed to distinguish primary hemorrhage from hemorrhage secondary to scratching lesions or associated with inflammation such as cellulitis or stasis dermatitis.
Simple Hemorrhage
Simple hemorrhage can be divided into findings with two separate sets of differential diagnoses: petechial or ecchymotic lesions.
Petechial Simple Hemorrhage
Thrombocytopenia or Platelet Dysfunction
Platelet counts above 50,000/mm 3 are usually not accompanied by purpura unless an abnormality of platelet function exists or there is a separate injury. Therefore, thrombocytopenia that might result in hemorrhage occurs at platelet counts of 50,000/mm 3 or less, and typically is not seen until the platelet count is 10,000/mm 3 or below. This is due largely to the role of platelets in releasing a variety of molecules necessary for endothelial cell health, including preserving the cadherin-mediated tight junctions between endothelial cells. Severe thrombocytopenia results in a degradation of endothelial cell health, and an increase in vascular permeability with red cell extravasation, particularly in areas of increased hydrostatic pressure. A variety of disorders can at times produce this degree of thrombocytopenia ( Table 15-1 ). Although severe thrombocytopenia may result in ecchymotic hemorrhage, usually the predominant morphology in any given patient is petechial. Conversely, platelet function defects may result in petechial hemorrhage and must be considered in this differential, but more often lead to scattered minor trauma-related ecchymoses. Although thrombocytopenic hemorrhage may occur anywhere, typically it is increased in dependent areas or at sites of minor trauma.
|
Intravascular Pressure Spikes
Petechial hemorrhage may also result from strong or repetitive localized increases in intravascular pressure. For example, straining during childbirth may produce petechial hemorrhage above the clavicles, solely from the vigorous Valsalva-like pressure effects. This can also occur with vigorous repetitive coughing or retching. In children, vigorous crying may produce a similar supraclavicular distribution of petechial hemorrhage. Ligature placement or strangulation may also produce distinctive patterns of petechial hemorrhage.
Minimally Inflammatory Microvascular Syndromes
There are a variety of minimally inflammatory syndromes affecting the very smallest dermal vessels, which may result in petechial hemorrhage, most included within the syndromes of the chronic pigmented purpuras and benign hypergammaglobulinemic purpura of Waldenström (see Vascular Causes, below).
Platelet function is also important. Intravascular hemorrhage associated with normal platelet counts may result from congenital or hereditary platelet function defects. More commonly encountered are acquired platelet function defects, especially those caused by drugs or metabolic abnormalities, such as severe renal or hepatic impairment. Another type of acquired platelet function defect occurs in patients with monoclonal gammopathies in which there may be interference with normal platelet function by the protein. Finally, patients with myeloproliferative disease and thrombocytosis in the range of 1,000,000/mm 3 will often have platelet dysfunction, and such patients may have problems with both hemorrhage and thrombosis.
Coagulation Cascade Problems in Hemostasis
The ability to form a normal platelet plug is the most important factor for normal hemostasis in the small vessels that supply the skin. The coagulation cascade system becomes important as the diameter of the vessel increases, and increasing forces of pressure and flow require reinforcement of the platelet plug by fibrin clots. This explains why patients with hemophilia or other procoagulant deficiencies of the coagulation cascade system usually do not present with spontaneous petechial hemorrhage. Instead, they present with relatively minor trauma-related injury of larger vessels in skin, fat, joint, or muscle, with the development of an overlying ecchymosis.
Other Intravascular Causes of Hemorrhage
Petechiae may develop in nondependent areas as a result of abrupt increases in capillary and postcapillary venule pressure. Forceful and repetitive Valsalva-like maneuvers, such as paroxysmal vomiting, violent coughing, or straining during childbirth, can cause petechial hemorrhage in supraclavicular areas even in patients whose platelet number and function are normal.
The Gardner–Diamond syndrome, or psychogenic purpura, is sometimes included in discussions of intravascular causes of hemorrhage. Whether this syndrome results from more than factitious disease remains suspect.
Vascular Causes
Vascular causes of hemorrhage include both inflammatory and noninflammatory disorders.
Inflammatory Causes
Inflammatory hemorrhage should include only those disorders in which vessel-directed inflammation is evident. Perivascular inflammation that is not vessel-directed should not be considered vasculitis, and it does not result in palpable purpura, the hallmark but not universal lesion of inflammatory hemorrhage. Lesions of palpable purpura are characterized by a port-wine color, incomplete blanching on pressure or diascopy, and palpability ( Fig. 15-2 ). Partial blanching of an early lesion is an important physical finding, with erythema correlating with inflammation and purpura with hemorrhage. Such lesions, when due to immune complex deposition, usually develop first in dependent areas, which in a bedridden patient may be the back and buttocks. An important cause of palpable purpura is small-vessel leukocytoclastic vasculitis, which has a variety of causes, including idiopathic, postinfectious, and drug-related; IgA-predominant vasculitis (Henoch–Schönlein purpura); mixed cryoglobulinemia; connective tissue disease, such as systemic lupus erythematosus and rheumatoid arthritis; and granulomatosis with polyangiitis (GPA), formerly Wegener’s granulomatosis, or allergic granulomatous polyangiitis (AGA) of Churg–Strauss s with or without granulomatous changes. However, the physical findings of palpable purpura may occasionally result from disorders in which vessel-directed inflammation is caused by a predominantly mononuclear cell infiltrate, as in erythema multiforme, and the pityriasis lichenoides group (especially PLEVA [pityriasis lichenoides et varioliformis acuta] syndrome). Patients with the aforementioned conditions who have leukocytoclastic vasculitis demonstrable in young cutaneous lesions may have biopsy specimens from older or treated lesions that show only perivascular lymphocytes.