Abstract
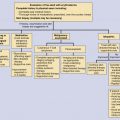
Cutaneous fungal infections with systemic involvement can be divided clinically into subcutaneous mycoses and systemic mycoses, based on mode of acquisition and the extent of tissue involvement. Subcutaneous mycoses are considered “implantation mycoses,” typically acquired via traumatic percutaneous inoculation from a contaminated object. These are caused by taxonomically diverse fungi that ordinarily subsist on decaying organic matter and have few intrinsic virulence factors. They are most common in tropical and warm temperate areas.
Systemic mycoses are considered “inhalational mycoses,” typically acquired via the respiratory route and can disseminate, usually hematogenously, to the skin and all other organs and tissues. The inhalational mycoses comprise two subgroups: four diseases (histoplasmosis, coccidioidomycosis, blastomycosis, paracoccidioidomycosis) that generally have well-established geographic ranges. These disorders usually cause subclinical or transient pulmonary infections in immunocompetent individuals and more serious infections in immunocompromised patients. Nevertheless, they may disseminate to involve the skin in both immunocompetent and immunocompromised hosts. In immunocompetent hosts, cutaneous involvement often presents with chronic crusted or granulomatous papules or plaques.
The second group of systemic mycoses includes opportunistic diseases (e.g., cryptococcosis, mucormycosis, aspergillosis) that occur mostly in immunocompromised hosts. These, too, may involve the skin after hematogenous dissemination. Because of the nature of the host’s immunologic status, these infections often present as acute, rapidly evolving, life-threatening infections.
Keywords
Aspergillosis, Candidiasis, Coccidioidomycosis, Cryptococcosis, Dermatomycoses, Hematogenous dissemination, Histoplasmosis, Mucormycosis, Opportunistic fungal infections, Sporotrichosis, Subcutaneous mycoses, Systemic mycoses
- •
Fungal pathogens affect the skin in many ways: superficial fungi, such as the dermatophytes, rarely cause systemic disease. Subcutaneous mycoses, such as sporotrichosis, mycetoma, and chromoblastomycosis, are typically caused by minor, inadvertent trauma that introduces environmental fungi into the skin and subcutaneous tissues. Host immunologic response toward these typically low-virulence fungi is muted.
- •
The classic systemic mycoses (histoplasmosis, coccidioidomycosis, blastomycosis, and paracoccidioidomycosis) are nearly always acquired via inhalation of fungal spores. Once in the lungs, the fungi adopt a pathogenic yeast-phase growth pattern. Infections are often limited to a transient pneumonitis but can disseminate hematogenously to any organ, although the skin is perhaps the most common target of a disseminated systemic mycosis.
- •
Immunocompromised patients are vulnerable to severe, rapidly life-threatening fungal diseases, such as aspergillosis and mucormycosis.
- •
Treatment for subcutaneous mycoses often requires dual therapy, e.g., oral antifungal agents with adjunctive surgical debridement.
- •
Treatment for inhalational mycoses is not required in cases of transient subclinical infections. For more severe cases (and especially in immunocompromised patients), treatment may consist of intravenous antifungal medications followed by prolonged oral suppressive therapy.
- •
There are literally tens of thousands of fungal species on earth of which less than 25 infect humans regularly—although perhaps hundreds have been isolated as rare causes of systemic disease, particularly in immunocompromised patients.
For clinical purposes, cutaneous fungal infections with systemic involvement can be divided into subcutaneous mycoses and systemic mycoses , based on the mode of acquisition and the extent of tissue involvement. The subcutaneous mycoses, of which sporotrichosis is the best known, may be considered “implantation mycoses” because they are typically acquired via traumatic percutaneous inoculation from a contaminated object.
The systemic mycoses, in contrast, may be considered “inhalational mycoses” because they are typically acquired via the respiratory route. The systemic mycoses comprise two subgroups: four diseases (histoplasmosis, coccidioidomycosis, blastomycosis, paracoccidioidomycosis) that usually cause subclinical or transient, self-limited pulmonary infections in immunocompetent individuals. Nevertheless, they may disseminate to involve the skin in both immunocompetent and immunocompromised hosts. In immunocompetent hosts, cutaneous involvement often presents with chronic crusted or granulomatous papules or plaques.
The systemic mycoses also include a subgroup of opportunistic diseases (e.g., cryptococcosis, mucormycosis, aspergillosis) that occur almost exclusively in immunocompromised hosts. These, too, may involve the skin after hematogenous dissemination. Because of the nature of the host’s immunologic status, these infections often present as acute, rapidly evolving, necrotizing infections.
The most prevalent cutaneous mycoses, dermatophyte infections, are caused by keratinophilic fungi that infect epidermis, hair, and nails but rarely cause systemic disease (extremely rare instances in severely compromised hosts). These will not be discussed further. Notably, active untreated dermatophyte infections can damage the epidermal barrier and serve as a portal of entry for other infectious agents, particularly bacteria and yeasts, and complete dermatologic examination is important when searching for potential sources of infection in all hosts.
Subcutaneous Mycoses with Systemic Manifestations
The subcutaneous mycoses are caused by taxonomically diverse fungi that ordinarily subsist on decaying organic matter and have few intrinsic virulence factors. Typically people acquire these conditions through minor, often unnoticed, percutaneous trauma with dead or decaying plant materials. Mammalian immune responses to these organisms are rarely vigorous and rarely effective; therefore these mycoses usually develop into chronic, unremitting infections that are confined to skin and subcutaneous tissues. Subcutaneous mycoses are most common among people in tropical and warm temperate areas who are routinely exposed to decaying organic matter. Farmers and people who gather firewood, especially if they are barefoot, are at greatest risk.
Several other subcutaneous infections that follow minor trauma, specifically pythiosis, rhinosporidiosis, actinomycetoma, and protothecosis, are occasionally included in sections on fungal diseases, even though taxonomic tools show that the pathogens are, indeed, not fungi. These will not be discussed further.
Sporotrichosis
Sporotrichosis, caused by Sporothrix schenckii , has worldwide distribution, but occurs most commonly in warm, humid areas where conditions favor its saprophytic growth. The organism typically enters the skin through minor injuries with plant materials, such as rose thorns, sphagnum moss, and damp straw, on which the fungus grows. Rarely, Sporothrix spores may be inhaled, causing pulmonary infection with subsequent cutaneous dissemination. Currently, the largest disease clusters of any type of sporotrichosis are among children in Brazil’s urban slums, where feral cats serve as the reservoir.
Clinical Manifestations
Classic sporotrichosis begins as a small painless papule at the inoculation site ( Fig. 33-1 ). Lesions usually evolve into firm, violaceous, dermal nodules. The surface may ulcerate, forming a sporotrichotic chancre with a ragged necrotic base, surrounded by epitheliomatous hyperplasia. When primary lesions are on distal extremities, local extension, called sporotrichoid spread, may occur via cutaneous lymphatic channels. This produces an ascending chain of either smooth dermal nodules or of ulcerating subcutaneous nodules ( Fig. 33-2 ). Lesions are most common on the hands and arms, but fixed centrofacial disease may occur in children, especially those with cat exposure ( Fig. 33-3 ).



Disseminated sporotrichosis is rare; it requires hematogenous dissemination from either primary cutaneous infection or primary inhalational disease. The most common extracutaneous sites are lungs, bones, and meninges. Risk factors for dissemination include hematologic/lymphoreticular malignancies, alcoholism, immunosuppressive medications, and AIDS.
Diagnosis
Because Sporothrix organisms are usually sparse in tissue, histopathologic diagnosis of sporotrichosis has low sensitivity. Culture on standard Sabouraud’s agar quickly grows a distinctive dark mold.
Treatment
Itraconazole is preferred to treat localized disease in immunocompetent adults. Oral potassium iodide solution is added in resistant cases. Disseminated disease usually requires amphotericin B followed by prolonged itraconazole therapy. In Brazil and Mexico, countries with high rates of sporotrichosis, oral terbinafine is the standard treatment.
Other Subcutaneous Mycoses
Uncommon inoculation mycoses, such as chromoblastomycosis, eumycetoma, lobomycosis, and entomophthoromycosis, are generally limited to cutaneous and subcutaneous tissues. Dissemination is rare, but may occur in immunocompromised patients. These will not be discussed further.
Systemic Mycoses
Four closely related species of fungi can cause systemic illness in immunocompetent individuals. These are Histoplasma capsulatum (histoplasmosis), Blastomyces dermatitidis (blastomycosis), Coccidioides immitis (coccidioidomycosis), and Paracoccidioides brasiliensis (paracoccidioidomycosis). The diseases are sometimes collectively called endemic mycoses because each was once regarded as having a restricted geographic distribution. They are also classified as thermally dimorphic mycoses because cultured colonies have one of two temperature-dependent morphologic appearances. At room temperature, which mimics their natural, outdoor saprophytic phase, cultures produce molds (extensive networks of hyphae that have a woolly or cottony appearance). In contrast, at body temperature, cultures form uniform, smooth colonies of yeast-like organisms. In histologic sections of diseased tissue (whether from skin, lung, or other organs), one sees only yeast, sometimes forming reproductive buds, but never hyphae. Sporotrichosis and Penicillium marneffei infection are also caused by thermally dimorphic fungi; these conditions are discussed elsewhere in this chapter.
People acquire these diseases mainly via inhalation of spores released by molds in nature, then lead to primary pulmonary infections. Within human tissues, the organisms assume their pathogenic yeast phase, which reproduce by forming buds with distinctive, diagnostic characteristics. In tissue, C. immitis forms distinctive spherical structures that produce daughter endospores internally. In histopathologic specimens, special fungal stains, such as Gomori methenamine silver or periodic acid–Schiff, greatly facilitate identification of these fungi.
A cautionary note is that dimorphic fungi should be cultured and examined in facilities with special mycologic capabilities. At room temperature, the molds, especially C. immitis , produce easily aerosolized propagules that create risk for accidental laboratory transmission.
Primary cutaneous involvement may occur with any of these diseases. It is rare and occurs after percutaneous inoculation of organisms.
Histoplasmosis
Histoplasmosis has been regarded as a disease primarily of the east-central United States, particularly along the Ohio River basin. In fact, H. capsulatum grows naturally in bird or bat guano and is found worldwide. A subspecies, H. capsulatum var. duboisii , causes disease in sub-Saharan Africa. Most histoplasmosis cases are subclinical or present as mild, self-limited pneumonitis. Disseminated histoplasmosis is a common opportunistic infection in patients with AIDS, malignancy, and other forms of immunosuppression.
Clinical Manifestations
Inhalation of spores leads to initial infection, which is asymptomatic in >80% of infected individuals. Many others have transient, self-resolving pneumonitis, often misdiagnosed as bronchitis or atypical bacterial pneumonia. Cutaneous histoplasmosis follows hematogenous dissemination from a primary pulmonary focus. Cutaneous lesions have a variety of nonspecific morphologies, including macules, papules/plaques, pustules/abscesses, ulcers, and purpuric infiltrates. Mucosal, especially oropharyngeal, ulcers are more common than lesions on keratinized skin. Erythema nodosum is a common but nonspecific reactive dermatosis, indicating a strong, successful immunologic response after primary exposure.
Diagnosis
Histoplasmosis is diagnosed by tissue or sputum cultures, serologic antibody tests, and/or urinary antigen studies. Biopsy specimens from skin or mucosa (along with lung, bone marrow, or other infected tissues) show perivascular inflammation with lymphocytes, plasma cells, and characteristic parasitized histiocytes that may contain abundant intracellular yeast, 1 to 3 μm each, which must be distinguished from several similar-sized intracellular pathogens, such as Leishmania . In patients with disseminated disease, bone marrow biopsy and culture may lead to the correct diagnosis. Histoplasmin skin testing is useful for population-based epidemiologic studies, not for establishing individual diagnoses.
Treatment
Patients with severe pulmonary infection or with cutaneous or mucocutaneous lesions, indicative of disseminated disease, require treatment with intravenous amphotericin. In immunocompromised patients, amphotericin is usually followed by long-term oral itraconazole therapy. Conversely, immunocompetent patients with benign, self-limited pneumonitis may be treated with supportive care alone.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


