Psoriasis
Jeffrey M. Weinberg MD
Psoriasis
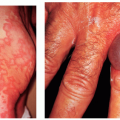
Psoriasis is a hereditary, papulosquamous skin disorder that affects 1.5% to 2% of the population in Western societies. In the United States, there are 3 to 5 million people with psoriasis, which affects men and women equally. Psoriasis can have multiple clinical presentations and varies widely among different individuals. It is typically a chronic and recurring disease that is best characterized by well-demarcated erythematous plaques with scaling. The plaques can be localized, which is the most common presentation, and confined to only certain delineated areas of the body. Most commonly plaques are seen on the elbows, knees, and the scalp. There are other variants of psoriasis. In palmoplantar psoriasis, lesions are limited to the soles of the feet and palms of the hands. In contrast, generalized pustular psoriasis and generalized erythrodermic psoriasis can involve the entire body and be a life-threatening condition, even necessitating hospitalization when seen in association with acute respiratory distress syndrome.
Primary Lesions
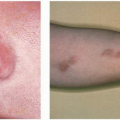
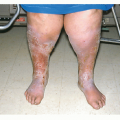
Plaque psoriasis: The lesions are well-demarcated, salmoncolored papules and plaques with thick silvery scaling that typically bleeds when removed (Auspitz’s sign). Lesions can vary greatly in size and shape in addition to distribution, which may be localized or generalized.
Pustular psoriasis: The lesions are typically yellow pustules that can coalesce and evolve into dark-red crusty lesions.
Secondary Lesions
Secondary lesions are less common but can include excoriations, lichenification, (thickening) oozing, and secondary infection.
Distribution
Psoriatic patches most commonly occur on the elbows, knees, and scalp, although involvement can occur on any area of the body, including palms, soles, and even nails.
Course
Psoriasis is typically a chronically recurring disease, although cases of complete resolution do occur. The onset of the disease can occur at any age, but the peaks of onset are in the 20s and 50s.
Causes
While the exact etiology of psoriasis is unknown, there is clearly a hereditary component. When one parent has psoriasis, a child has an 8% chance of having the disease. If both parents have psoriasis, the child’s chance of developing psoriasis increases to as high as 41%. Specific human leukocyte antigen (HLA) types have been noted to have a higher frequency of association with psoriasis, specifically HLA-B13, HLA-B17, HLA-Bw57, and most notably HLA-Cw6.
An acute form of guttate psoriasis, which characteristically develops in children and younger adults, often follows a streptococcal infection and has characteristic smaller sized, drop-shaped lesions.
Triggering factors include physical trauma, which can elicit the lesions, or any type of excessive rubbing or scratching, which can stimulate the proliferative process. Aggravating factors include psychologic stress and certain medications such as systemic glucocorticoids, oral lithium, antimalarial drugs, systemic interferon, beta-blockers, and potentially angiotensinconverting enzyme inhibitors. Alcohol and smoking may also aggravate psoriasis.
Subjective Complaints
Thirty percent of patients present with a complaint of pruritus, especially when psoriasis involves the scalp and anogenital area. Also common are complaints of joint pain, termed psoriatic arthritis, found in 5% to 8% of patients with psoriasis. Interestingly, 10% of patients with psoriatic arthritis have no skin manifestations of the disease. Finally, in a rare acute onset of generalized pustular psoriasis called von Zumbusch syndrome, there is associated weakness, chills, and fever.
Season
Exacerbation is typically seen in the winter, most likely due to the lack of sunlight and low humidity. Natural ultraviolet light typically causes psoriatic symptoms to improve.
Age Group
Contagiousness
Psoriasis is not contagious.
Relation to Employment
Psoriatic lesions occur more typically in areas of skin injury or repeated skin stress or pressure. This is known as the Koebner phenomenon.
Laboratory Findings
The diagnosis of psoriasis is usually made on clinical grounds, and biopsy is not necessary. If biopsy is performed, histologic findings include the following:
1. Acanthosis: thickening of the skin
2. Increased mitosis of keratinocytes, fibroblasts, and endothelial cells
3. Inflammatory cells in the dermis and epidermis
Differential Diagnosis
1. Seborrheic dermatitis: Lesions more yellowish and greasy than those of psoriasis. In the scalp, the scale is usually less thick than in psoriasis. Seborrheic dermatitis and psoriasis can often coexist in some patients.
2. Lichen simplex chronicus: Usually fewer patches than psoriasis, with less of a thick scale.
3. Tinea corporis: Usually a single lesion, with outer scale and central clearing. Potassium hydroxide preparation and fungal culture are positive for fungi.
4. Psoriasiform drug eruptions: Check medication history.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


