Abstract
Myriad cutaneous changes, both physiologic and pathologic, occur in the context of pregnancy. Pregnancy-related alterations of the skin may be classified as: (1) physiologic changes; (2) changes to cutaneous neoplasms; (3) preexisting skin disease or internal disease with skin manifestations affected by pregnancy; (4) pruritus in pregnancy; and (5) dermatoses specific to pregnancy. This chapter reviews the nonspecific and specific dermatologic changes observed in pregnancy, emphasizing the need for accurate diagnosis and prompt recognition of any associated maternal or fetal risks.
Keywords
Atopic dermatitis, Impetigo herpetiformis, Intrahepatic cholestasis, Melasma, Pemphigoid gestationis, Polymorphic eruption of pregnancy, Pregnancy, Pruritus, Striae gravidarum
- •
Physiologic changes associated with pregnancy have effects on the skin including pigmentary changes such as linea nigra and melasma; vascular changes such as telangiectasia, varicosities, and spider angiomata; connective tissue changes such as striae distensae; and changes on glandular structures, hair, nails, and mucosal surfaces.
- •
Pregnancy can also impact neoplasms both benign and malignant.
- •
There is a variable and often unpredictable effect of pregnancy on preexisting chronic skin diseases including psoriasis, atopic dermatitis, dermatomyositis, lupus erythematosus, and infections including viral, fungal, and mycobacterial in nature.
- •
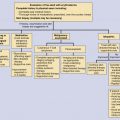
Pruritus is a prominent feature of pregnancy that might be related to a preexisting condition, to cholestasis, or occur in association with a “specific” dermatosis of pregnancy.
- •
There are two major “specific” pregnancy dermatoses: polymorphic eruption of pregnancy (formerly known as pruritic urticarial papules and plaques of pregnancy) and pemphigoid gestationis.
Myriad cutaneous changes, both physiologic and pathologic, occur in the context of pregnancy. Pregnancy-related alterations of the skin may be classified as: (1) physiologic changes; (2) changes to cutaneous neoplasms; (3) preexisting skin disease or internal disease with skin manifestations affected by pregnancy; (4) pruritus in pregnancy; and (5) dermatoses specific to pregnancy. This chapter reviews the nonspecific and specific dermatologic changes observed in pregnancy, emphasizing the need for accurate diagnosis and prompt recognition of any associated maternal or fetal risks.
Physiologic Skin Changes
Pregnancy causes physiologic changes to the skin, hair, nails, and mucous membranes. Observed changes in skin during pregnancy result from alterations in pigmentation, vasculature, connective tissue, and glands. Although sometimes striking, such physiologic changes have no impact on maternal or fetal health.
Pigmentary Changes
Hyperpigmentation
Up to 90% of pregnant women demonstrate some degree of hyperpigmentation, which most often is localized and discrete. Generalized hyperpigmentation rarely occurs in pregnancy. When observed, additional etiologies (i.e., adrenal insufficiency, thyrotoxicosis) should be considered. Hyperpigmentation during pregnancy most commonly manifests as linea nigra, a darkening of the linea alba (the tendinous median line on the anterior abdominal wall spanning from the pubic symphysis to the xiphoid process), which appears in the first trimester of pregnancy and is more pronounced in women with darker skin types. Physiologic hyperpigmentation also affects the nipples, areolae, neck, axillae, genitalia, perineum, perianal skin, and medial thighs. Hyperpigmentation resolves gradually postpartum over several months.
Pigmentary demarcation lines, sharp delineations between areas of more and less pigmented skin, occurring most commonly on the lower extremities (type B Futcher lines), have been reported to darken or appear de novo during pregnancy. Uncommon pigmentary patterns that can be encountered in pregnancy include pseudoacanthosis nigricans, dermal melanocytosis, and vulvar melanosis.
Melasma (chloasma, “mask of pregnancy”) presents as symmetric, irregular hyperpigmented patches involving sun-exposed areas of the cheeks and nose (malar pattern); the forehead, nose, cheeks, upper cutaneous lip, and chin (centrofacial pattern); or the ramus of the mandible (mandibular pattern). Prevalence of melasma in pregnancy ranges from 5% to 46%, varying greatly by demographic population and geography. Risk factors for melasma include intermediate skin phototypes (Fitzpatrick III–IV), ultraviolet (UV) radiation exposure, family history of melasma, oral contraceptive pill use, and thyroid dysfunction, as well as number of pregnancies and age at first pregnancy. Approximately half of women report onset of melasma in the context of pregnancy or oral contraceptive pill use. The pathogenesis of melasma is poorly understood; elevated levels of estrogen, progesterone, and melanocyte-stimulating hormone during pregnancy may play a role.
Melasma usually resolves with treatment within 1 year postpartum; spontaneous remission rates are low (6%). Pigmentary abnormalities persist in up to 30% of patients; risk factors include previous oral contraceptive pill use and more severe melasma pigmentation. Melasma may recur with subsequent pregnancies or oral contraceptive pill use. Avoidance of UV exposure and regular use of broad-spectrum sunscreen (≥SPF30) have preventive and therapeutic benefit. Patients should be advised to avoid potentially irritating and sensitizing cosmetics and to consider nonhormonal methods of contraception. Melasma can be treated postpartum with hydroquinone, azelaic acid, topical retinoids, or combinations thereof. Additional postpartum treatment modalities include laser treatment and chemical peels.
Jaundice
The serum bilirubin level may increase in 2% to 6% of uncomplicated pregnancies but is almost always less than 2 mg/dL. Severe hepatic dysfunction during pregnancy is rare. The most common cause of jaundice in pregnant women is viral hepatitis. Jaundice can develop in severe cases of intrahepatic cholestasis of pregnancy (ICP) (see “Pruritus in Pregnancy” section).
Vascular Changes
Elevated estrogen levels and increased blood volume during pregnancy result in proliferation of blood vessels, vascular distention, vasomotor instability, and increased cutaneous blood flow. Cutaneous vascular changes typically regress postpartum.
Palmar Erythema
Approximately two-thirds of white women and one-third of black women develop palmar erythema in pregnancy with onset in the first trimester. Palmar erythema tends to be symmetric and may be diffuse or limited to the thenar and hypothenar eminences, metocarpophalangeal joints, and finger pulps. Patients may report intermittent burning sensation. In pregnancy, there is no association between palmary erythema and hepatic or thyroid dysfunction. Palmar erythema resolves postpartum.
Spider Angioma
Spider angiomas (arterial spiders, nevi araneus, spider nevi, vascular spiders) occur in about two-thirds of white women and 11% of black women with onset between the second and fifth months of pregnancy. Spider angioma presents as a central erythematous papule (dilated arteriole) with radiating telangiectactic branches, often surrounded by a 3- to 4-mm anemic halo. Spider angiomas of pregnancy develop most commonly in areas drained by the superior vena cava (i.e., head, neck, upper chest, upper extremities). The majority resolve within 3 months of delivery. Cosmetic treatment modalities for persistent angiomas include electrodesiccation, intense pulsed light, and vascular laser.
Edema
Nonpitting edema of the eyelids, face, and lower extremities may develop later in pregnancy and is seen in one-third of women by week 38. Eyelid edema occurs in approximately 50% of pregnant women, whereas benign lower-extremity edema develops in about 70%. The presence of edema in a pregnant woman should alert the physician to the possibility of pregnancy-induced hypertension, which carries a significant risk to mother and fetus, and appropriate further evaluation should be undertaken.
Varicosities
Compression of the pelvic and femoral vessels by the gravid uterus results in the formation of lower-extremity (saphenous), vulvar, and hemorrhoidal varicosities. Genetic predisposition poses additional risk. Lower-extremity varicosities occur in 40% of pregnant women. Rest, lower-extremity elevation, avoidance of prolonged standing or sitting, use of gradient compression/elastic stockings and sleeping in a left lateral decubitus position may improve lower body circulation and reduce varicosity-associated symptoms. Varicosities may improve postpartum but generally do not regress completely. Postpartum treatment options include sclerotherapy, laser, and phlebectomy. Varicosities are likely to recur in subsequent pregnancies.
Cutis Marmorata
Cutis marmorata presents as transient, bluish, mottled patches on the lower extremities with cold exposure. Attributed to vasomotor instability secondary to increased estrogen levels, cutis marmorata is not unique to pregnancy and has no impact on maternal or fetal health.
Connective Tissue Changes
Striae Gravidarum
Striae gravidarum (striae distensae, stretch marks) are a common though poorly understood phenomenon. Prevalence ranges from 50% to 90%, and all races are susceptible. Onset of striae formation in pregnancy occurs prior to 24 weeks gestation in 43% of women. The etiology of striae gravidarum is unknown. Hormonal and physical factors are believed to result in a reduced number and altered orientation of dermal elastic fibers and fibrillin microfibrils. Risk factors for striae gravidarum include family history of striae gravidarum, personal history of breast or thigh striae, younger maternal age, and greater weight gain during pregnancy. Striae gravidarum initially present as pink to violaceous linear or arcuate patches, which gradually transform into hypopigmented atrophic, finely wrinkled plaques. The most common locations are the abdomen, breasts, and thighs; additional sites include the buttocks, hips, lower back, and upper arms. Striae may become less apparent over time but do not fully disappear. To date, no successful preventive treatments for striae gravidarum formation have been identified. Vascular laser and intense pulsed light improve the erythema of early striae. Topical retinoids (with or without glycolic acid) and laser and light treatment modalities may improve striae appearance.
Glandular Changes
Eccrine gland function increases during pregnancy, which may explain the increased prevalence of miliaria, dyshidrosis, and hyperhidrosis. Reduced palmar sweating, however, has been reported. Apocrine gland activity may decrease during pregnancy, contributing to the reduced prevalence of Fox–Fordyce disease in pregnancy. Pregnancy has varying effects on hidradenitis suppurativa; a minority of pregnant women report improvement in hidradenitis suppurativa during pregnancy. Variable changes in sebaceous gland activity have been reported, and the course of acne during gestation is unpredictable. One study showed that acne was affected by pregnancy in 70% of patients, with 41% experiencing improvement and 29% worsening. Montgomery tubercles form as small brown papules on the areolae in 30% to 50% of women during the first trimester as the result of sebaceous gland hypertrophy; these regress postpartum.
Hair Changes
Hirsutism in pregnancy results from increased activity of ovarian and placental androgens on the pilosebaceous unit and is more prominent in women with abundant body hair or dark hair at baseline. Hirsutism occurs most often on the face but may involve the arms, legs, back, and lower abdomen. While lanugo hair regresses within 6 months postpartum, terminal hair growth is typically permanent. If hirsutism is severe or is accompanied by other signs of virilization, androgen-secreting tumor of the ovary or adrenal gland, luteoma, theca lutein cyst, and polycystic ovary disease should be excluded.
Telogen effluvium refers to hair loss that occurs when a significant proportion of hairs synchronously enter the telogen phase. In the later stages of pregnancy as much as 95% of scalp hair is in anagen phase, which then abruptly cycles into telogen phase after delivery. Postpartum telogen hair counts of 24% at 6 weeks and 65% at 2 months have been reported. Causes for the shift from anagen to telogen may include the stress of delivery and changes in endocrine balance, including prolactin secretion with lactation. Increased hair shedding of variable severity becomes apparent 1 to 5 months postpartum. Hair regrowth occurs spontaneously within 6 to 12 months, but complete resolution may require up to 15 months. Scalp hair density may never return to baseline prepregnancy density, especially in women with concomitant female pattern hair loss.
Frontoparietal hair recession reminiscent of male pattern androgenic alopecia has been reported late in pregnancy; this typically resolves postpartum.
Nail Changes
Nail growth increases during pregnancy. Additional changes include brittleness, distal onycholysis, leukonychia, melanonychia, softening, subungual hyperkeratosis, and transverse grooves. Nail changes may occur as early as the sixth week of gestation. The etiology of these changes remains unclear, but some may also be seen in nonpregnant women taking oral contraceptives. Nail changes generally improve postpartum, and no specific treatment is required. Patients should be evaluated for dermatoses that affect the nail unit (i.e., psoriasis, lichen planus) and infections. External sensitizers (nail polish and polish removers) should be eliminated. Nails should be trimmed short, and the use of a nail moisturizer may provide benefit.
Mucous Membrane Changes
Pregnancy gingivitis affects 30% to 75% of pregnant women. Clinically, it presents in the first trimester as hyperplasia and blunting of the gingival interdental papillae with erythema, edema, ulceration, and bleeding of variable severity. Patients typically have preexisting gingivitis, and pregnancy merely exacerbates the baseline condition. Treatment consists of rigorous dental hygiene, professional debridement/scaling, and occasionally oral antibiotics. Oral pyogenic granulomas develop in 2% of pregnant women (see “Cutaneous Neoplasms Affected By Pregnancy”). Additional mucosal changes in pregnancy include hyperemia and congestion of the nasal mucosa, and a bluish-purple discoloration of the vaginal mucosa (Chadwick’s sign) and the cervix (Goodell’s sign).
Cutaneous Neoplasms Affected by Pregnancy
Various cutaneous neoplasms are affected by pregnancy ( Table 41-1 ).
| Dermatofibroma |
| Dermatofibrosarcoma protuberans |
| Desmoid tumor |
| Glomangioma |
| Glomus tumor |
| Hemangioendothelioma |
| Hemangioma |
| Keloid |
| Leiomyoma |
| Melanocytic nevus |
| Melanoma |
| Molluscum fibrosum gravidarum (acrochordon) |
| Neurofibroma |
| Pyogenic granuloma of pregnancy (granuloma gravidarum) |
Melanocytic Nevus
Preexisting melanocytic nevi may enlarge and/or darken, and new nevi may appear during pregnancy. Prospective studies, however, utilizing dermoscopy and spectrophotometric intracutaneous analysis have not demonstrated significant changes in melanocytic nevi during pregnancy. Women with dysplastic nevus syndrome may exhibit higher rates of clinical changes in their melanocytic nevi during pregnancy compared to nonpregnancy time periods. A changing pigmented lesion in a pregnant woman should not be attributed to pregnancy alone and should be evaluated just as for nonpregnant patients. There is no evidence that gestation induces dysplastic/malignant transformation of preexisting nevi.
Melanoma
Melanoma is the most common cancer for reproductive-age women. Estimated incidence of melanoma complicating pregnancy ranges from 0.1 to 2.8 per 1000 pregnancies. Despite initial concerns about adverse effects of pregnancy on malignant melanoma, most recent studies consistently demonstrate that pregnancy does not adversely affect the survival of women diagnosed with localized melanoma before, during, or after pregnancy. Melanoma prognosis for the pregnant woman should be based on the same established criteria, including Breslow depth and ulceration, utilized for nonpregnant patients. Transplacental metastasis of maternal malignancy is rare; malignant melanoma, however, is the most common malignancy to metastasize to the placenta (20 cases). In the setting of placental melanoma metastasis, fetal metastasis occurs in only 25%, and the most common sites are the skin and liver. For pregnant women with metastatic melanoma, the risks and benefits of adjuvant systemic therapy should be discussed; the option of termination of pregnancy should be considered early enough to provide adequate time for decision-making.
Molluscum Fibrosum Gravidarum
Molluscum fibrosum gravidarum (acrochordons, skin tags) are soft tissue fibromas that typically occur in the latter half of pregnancy on the skin of the face, neck, chest, axillae, inframammary folds, and groin. Papules may regress postpartum. Residual lesions may be removed via snipping, cryotherapy, or electrocautery.
Neurofibroma
More than half of women with neurofibromatosis type 1 note an increase in the growth of new or existing neurofibromas during pregnancy; one-third of neurofibromas decrease in size after delivery. Large neurofibromas may be complicated by intralesional hemorrhage. It is unclear whether women with neurofibromatosis are at increased risk of hypertension, preterm delivery, growth restriction, or other maternal/fetal complications; close monitoring is recommended.
Pyogenic Granuloma
Pyogenic granuloma of pregnancy (epulis gravidarum, granuloma gravidarum, pregnancy epulis, pregnancy tumor) is a common, benign neoplasm resulting from hyperplasia of capillaries and fibroblasts (lobular capillary hemangioma). Pyogenic granulomas present as red, friable, sessile, or pedunculated papules. Lesions are typically painless but bleed with minimal trauma. Oral pyogenic granulomas, located on the labial, gingival, lingual, palatal, or buccal mucosa, develop in 2% of pregnant women; dental plaque deposits or pregnancy gingivitis may incite their formation. Additional common sites include the face and hands/fingers. Pyogenic granulomas may occur at any time during pregnancy, may recur after removal, and tend to regress postpartum.
Preexisting Skin Diseases and Internal Diseases with Skin Manifestations Affected by Pregnancy
Pregnancy may exert variable, and often unpredictable, effects on both systemic and cutaneous inflammatory diseases due to the altered immunologic profile designed to prevent fetal rejection ( Table 41-2 ). Diseases associated primarily with a Th1-immune response typically improve during pregnancy while Th2-associated disorders tend to deteriorate during gestation. Diseases that are more likely to improve during gestation include chronic plaque psoriasis, linear IgA bullous dermatosis, rheumatoid arthritis, and sarcoidosis.
| Infections |
| Herpes simplex virus infection |
| Human immunodeficiency virus infection and acquired immunodeficiency syndrome |
| Human papillomavirus infection (bowenoid papulosis, condyloma acumuminata, verruca vulgaris) |
| Leprosy |
| Pityrosporum folliculitis |
| Trichomoniasis |
| Varicella-zoster virus infection |
| Vulvovaginal candidiasis |
| Autoimmune Diseases |
| Dermatomyositis |
| Lupus erythematosus |
| Pemphigus foliaceus |
| Pemphigus vulgaris/vegetans |
| Systemic sclerosis |
| Metabolic Diseases |
| Acrodermatitis enteropathica |
| Porphyria cutanea tarda |
| Connective Tissue Diseases |
| Ehlers–Danlos syndrome |
| Pseudoxanthoma elasticum |
| Miscellaneous Disorders |
| Acanthosis nigricans |
| Erythema multiforme |
| Erythema nodosum |
| Erythrokeratoderma variabilis |
| Hereditary hemorrhagic telangiectasia |
| Mycosis fungoides |
| Tuberous sclerosis |
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


