Practical Aspects of Facial Reconstruction
The practical goal of facial reconstruction is to provide the most aesthetic and functional repair possible, striving to meet or exceed the patient’s expectations. The goal is to restore the appearance and function to a point in time before the patient developed skin cancer and required Mohs or excisional surgery. Unfortunately, surgery to remove the cancer and to repair the surgical defect creates scars. The successful reconstructive surgeon minimizes scars through a number of techniques, such as closure at the junction of cosmetic units or subunits, avoidance of deviation of free margins and anatomical landmarks, and reconstruction with tissue of similar color and texture. Above all, take the patient’s expectations into account. Some patients will prefer the simplest option possible, which may be second intention healing, whereas others may be particularly meticulous and require a more exacting reconstruction. In some instances, patients may be resistant to a flap repair as additional incisions must be made to create and mobilize the flap. In these instances, although a flap repair might provide a superior cosmetic or functional result for most patients, a graft repair or second intention healing may be preferable because no additional or iatrogenic incisions and scars are created by the surgeon. Discuss the repair with the patient before surgery, and be open to adjust or change your planned repair on the basis of the patient’s input.
2.1 SECOND INTENTION HEALING
Second intention healing may be an excellent alternative for select defects. For surgical defects on concave areas, repair by second intention healing offers a simple and attractive repair option (Fig. 2.1A). Large defects on the concave surface of the temple heal well by second intention healing so long as the defect is not too close to a free margin or anatomical landmark (Section 4.8). In these situations, where the defect may be close to the eyebrow, lateral canthus, or eyelid, a graft or partial closure repair near the free margin may be used to minimize scar contracture and avoid free margin or anatomical landmark deviation (Section 8.6).
For defects in the conchal bowl of the ear that do not approach the external auditory meatus (EAM), second intention healing may be an excellent choice for repair (Section 7.4). For defects involving a majority of the EAM or risk constriction of the EAM, a full-thickness skin graft, preauricular transposition flap or postauricular pull-through flap may be a better alternative to speed healing and minimize narrowing of the meatus (Sections 7.3 and 7.5); however, if the defect involves only a small portion of the EAM, second intention healing may still be considered.
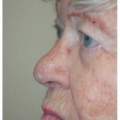
In other facial regions, superficial defects on concave surfaces of the nose (e.g., alar crease) and eyes (e.g., medial canthus) may heal well by second intention healing (Figs. 2.1A, B, C, D, E).
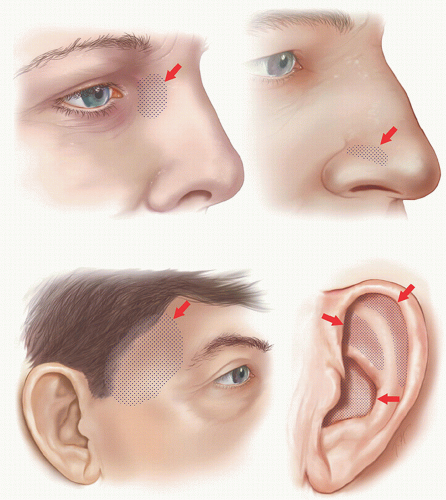 Figure 2.1A. Surgical defects on concave areas of the head may heal well by second intention healing. The diagram demonstrates stippled areas in various locations where second intention healing may be a good consideration. This may include superficial concave areas of the ear, nose, medial canthus, and temple. If a defect involves or approximates an anatomical landmark or free margin, consider repair or partial repair to avoid deviation of the landmark or margin. |
 Figure 2.1B. Superficial defect on the right medial canthus measures approximately 1.1 × 0.7 cm. Patient wanted to avoid additional scars and desired simplest repair. |
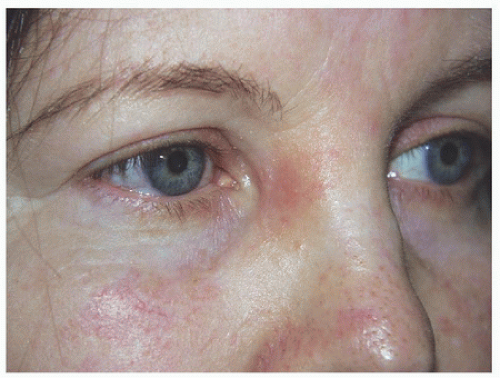 Figure 2.1C. Healed result at 3 months after allowing the wound to heal by second intention healing. |
 Figure 2.1D. Superficial wound on the right alar crease and another smaller wound on the posterior aspect of the nasal ala. |
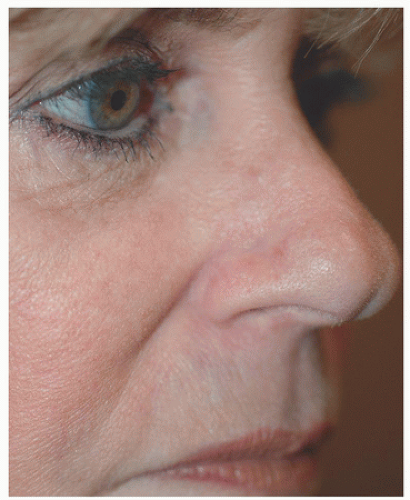 Figure 2.1E. Healed appearance following second intention healing. (Defect on posterior nasal ala was also allowed to heal by second intention healing as it was in relatively concealed location.) |
2.2 SIDE-TO-SIDE REPAIR
Next to second intention healing, the simplest repair is a side-to-side repair. If the defect is elliptical in shape, the wound can be closed without the removal of tissue redundancy, usually referred to as a tricone, standing cone, or “dog ear.” Conversely, most defects in skin cancer surgery tend to be oval, circular, or irregular in shape. As a result, most side-to-side repairs entail removal of one or more dog ears, usually at the poles of the closure, although removal of these dog ears may be designed to occur elsewhere along the incision or angled in a particular direction (Figs. 2.2A, B, C, D).
To increase the chance of producing an incision and thus a scar that remains fine and well hidden, the wound should be closed along relaxed skin tension lines (RSTL) whenever possible. The RSTL tend to run perpendicular to underlying musculature and fall within real or anticipated rhytides or furrows (see Fig. 1.1).
Through closure of the defect and removal of the dog ears, the final length of the incision and scar is lengthened. In general, the length of the closure (i.e., the length of an elliptical excision) is roughly three times the width of the closure (i.e., the width of the ellipse); however, this ratio can be increased to 4:1 or greater when the closure is over a convex surface (e.g., convex portion of the cheek or around the forearm) (Section 3.1). A key point is to discuss and explain this to the patient in advance of the repair. Most people understand and appreciate the concept of lengthening the repair, removing the dog ears, placement within RSTL, especially when explained in advance of the repair. Better to educate in advance rather than try to justify later.
 Figure 2.2A. Surgical defect on the right cheek. |
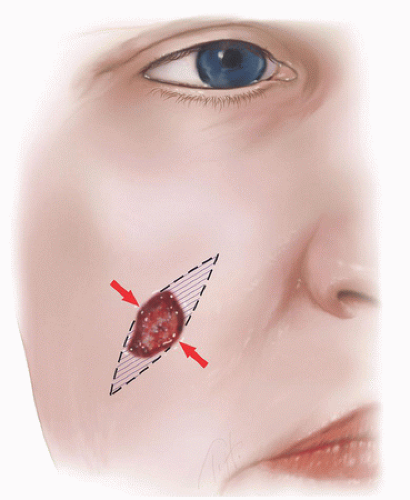 Figure 2.2B. Design of the side-to-side repair. The wound is closed in the direction of relaxed skin tension lines (see also Fig. 1.1). Two tricones or standing cones (“dog ears”) are excised at the poles of the defect, creating an ellipse that measures approximately 3:1 length to width ratio. |
 Figure 2.2C. Wound closed in a side-to-side fashion along relaxed skin tension lines with excision of tricones. (Wound closed with 4-0 polyglactin 910 buried vertical mattress sutures and epidermis approximated and everted with 6-0 polypropylene simple interrupted sutures.) |
 Figure 2.2D. Final healed result. (Telangiectasias present preoperatively as well and could be treated with pulsed dye laser.) |
For side-to-side repairs approaching a free margin or anatomical landmark, consider changing the direction of the dog ear excision. In other words, remain within RSTL whenever possible but not at the expense of deviating the free margin or anatomical landmark. For example, for lower eyelid defects that can be closed in a side-to-side fashion, as you approach the lid margin, you might have to redirect the incision line upward (rather than remaining within the fine lines on the eyelid skin) and end up more perpendicular to the lid margin to avoid secondary tension vectors, which might result in ectropion.
2.3 ADVANCEMENT FLAPS
Although advancement flaps permit slightly more tissue movement than side-to-side repair, one of their main benefits is to allow the placement of incision lines and tricones (dog ears) in more favorable positions (Figs. 2.3A, B, C, D). Doing this helps advancement flaps to recruit an additional amount of tissue laxity in comparison with side-to-side repair (Section 5.2). Another benefit of moving incision lines and tricones is the avoidance of violating free margins or boundaries (e.g., crossing the alar crease when repairing the sidewall) or of crossing into another cosmetic unit or subunit (e.g., crossing into the nasal tip when repairing the nasal dorsum).
The closure tension vectors remain parallel to the primary motion of the flap so there is little or no tension redirection, but in some instances, a unilateral or bilateral advancement flap may offer distinct advantages over other types of flaps (e.g., transposition). These may include repairs on the forehead or midnasal dorsum for defects too large to be easily closed in a side-to-side fashion (Sections 4.6 and 5.2). In these instances, it may be preferable to consider a repair that borrows tissue laxity bilaterally, in essence sharing donor sites symmetrically. Although a rhombic or bilobed transposition flap may be able to repair a defect on the midnasal dorsum, it borrows tissue from just one side of the nose. The result may be nasal asymmetry when the patient is viewed from the front because tissue from only one side is borrowed. With a bilateral repair, tissue is borrowed from both sides, creating a slightly thinner but symmetrical nose.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


