Introduction
Oncoplastic breast surgery has become a common option for women with breast cancer and is currently being performed throughout the world on a regular basis. This operation has provided women with the best of oncologic and reconstructive options in that they can achieve oncologic safety and efficacy, retain the majority of their breast, and retain a natural breast appearance. In many parts of the world, breast surgeons and plastic surgeons perform oncoplastic breast surgery as a team and work together to optimize surgical outcomes. Breast and plastic surgeons each have a unique perspective on oncoplastic surgery and how to perform it. Many breast surgeons have expanded their scope of practice and now perform simple reconstructive procedures in addition to ablative procedures. Plastic surgeons continue to be an integral component of the oncoplastic team in that they can provide expertise in both simple and complex situations. This chapter will provide a plastic surgeon’s perspective on oncoplastic breast surgery.
Role of Plastic Surgery
Plastic surgeons have a long-standing interest in reconstructive breast surgery and have been at the forefront of reconstructive innovation. The role of the plastic surgeon is to provide expertise in the management of complex defects of the breast following partial mastectomy and not just to close a defect. Plastic surgeons are able to incorporate principles and concepts to reshape and contour the breast in a predictable and reproducible manner. Oftentimes, this is relatively straightforward and may not require complex maneuvers; however, there are times when a defect may be larger than usual relative to the volume of the breast or it may be in a location that will be difficult to reconstruct.
There are many surgeons who feel that plastic surgery comprises a collection of techniques that can be performed by anyone. Being able to perform a particular procedure can be learned, but understanding the principles and concepts that dictate the optimal operation requires training and specialization. Fellowship programs now exist that combine the oncologic and plastic surgical principles to optimally care for these patients. Plastic surgeons have an intricate understanding of blood supply and tissue perfusion and are able to use local parenchymal flaps and, in more complex cases, remote adipocutaneous flaps. Inherent to this is an understanding of tissue tension, perfusion analysis, appropriate suturing techniques, the use of drains, and a working knowledge of breast aesthetics and how to achieve them.
It is clearly appreciated that not every partial mastectomy defect will require the assistance of a trained plastic surgeon. Defects that are relatively small may be easy to close without the assistance of a trained plastic surgeon and result in minimal to no breast distortion. There are a number of techniques and approaches that have been described to facilitate these reconstructive maneuvers, and if breast surgeons can perform them safely and effectively, then they should do so. One of the principles that plastic surgeons adhere to is that the performance of a particular operation should be based on the ability to take care of any complications that may arise following that operation. In the case of oncoplastic surgery, this includes, but is not limited to, delayed healing, fat necrosis, skin necrosis, nipple–areolar necrosis, infection, bleeding, seroma, asymmetry, and complex scarring. The role of the plastic surgeon should not solely be to manage complications but rather to perform operations that will minimize the risk of complications.
In the specialized field of oncoplastic breast surgery, there are currently three pathways for plastic and breast surgeons to collaborate. The first and traditional pathway is for plastic and breast surgeons to work together on all cases. It can be argued that this option will provide patients with optimal outcomes based on the combined expertise with the oncologic and reconstructive management of the patient. The second pathway also involves both the breast and plastic surgeons with specific involvement based on the complexity of the reconstruction. This is the model that exists throughout much of Europe in which the breast surgeon will perform certain reconstructive procedures such as an implant, latissimus dorsi flaps, and reduction mammaplasty, and the plastic surgeon will perform the more complex procedures such as pedicled abdominal flaps or free tissue transfers. The third pathway is the least common in which a sole surgeon provides the oncologic and reconstructive options in all cases. The specialist may be a breast surgeon trained in reconstructive techniques or a plastic surgeon trained in oncologic management.
Breast reconstruction and oncoplastic surgery have evolved over the years to the point that they are regarded as oncologically safe and aesthetically advantageous. Surgeons now practice in an era of high patient expectations where many patients will desire to have their appearance enhanced following surgery. This is why the role of trained plastic surgeons is so important when it comes to oncoplastic procedures of the breast. Studies have confirmed the ability of plastic surgeons to create ideal breast proportions based on case complexity and the optimization of operative techniques. In a recent survey of membership from the American Society of Plastic Surgeons and the American Society of Breast Surgeons, 70% of breast surgeons felt that partial breast reconstruction following lumpectomy compromised a good portion of their practice, whereas 50% of plastic surgeons felt that their ability to perform oncoplastic surgery was limited due to a lack of referrals. Interestingly, both societies opined that complex partial breast reconstruction was best performed using the team approach. Benefits of the team approach included being able to take wider margins and enhanced aesthetics.
Based on this survey, it is important for plastic surgeons who have an interest in oncoplastic breast surgery to make their referring breast surgeons aware of their interest and desire to collaborate. Many breast surgeons become frustrated with their plastic surgery colleagues because they are often not available or are busy doing other operations. Coordinating the two schedules can sometimes be a challenge, but plastic surgeons should make every effort to facilitate a good relationship with breast surgeons and have designated blocks for these operations. Failure to do so will result in a reduction in referrals and the gradual erosion of our ability to stay active in breast reconstruction. Plastic surgeons have advanced the field of breast reconstruction and have been performing high-level aesthetic and reconstructive breast surgery for decades. It would be a shame for the specialty of plastic surgery to become obsolete in the oncoplastic care of breast cancer patients.
Vascular Anatomy
When considering oncoplastic surgery, a thorough understanding of the vascular anatomy of the breast is critical. The primary blood supply to the breast is derived from the perforating branches of the internal mammary and lateral thoracic vascular systems. These perforators will traverse through the breast to form an anastomotic cluster around the periareolar region and provide vascularity to the nipple–areolar complex (NAC). It is important to realize that the vascularity to the parenchyma and the skin are distinct and can be compartmentalized. Another dominant source of blood supply is via the intercostal perforators. Studies have demonstrated that the second, third, and fourth perforating branches of the intercostal system course within the horizontal ligament of the breast toward the nipple. The remainder of the vascular supply to the breast is derived from the thoracoacromial and superficial thoracic arteries. This knowledge is important when designing parenchymal flaps and in maintaining the perfusion to the skin and NAC.
Patient Selection
When a patient with breast cancer is referred for reconstructive options, more often than not, the breast surgeon has reviewed the oncologic options with the patient and mentioned some of the reconstructive options. During the initial consultation, a thorough history and physical examination is performed. An assessment of comorbidities is completed with an emphasis on cardiac disease, pulmonary disease, tobacco use, and diabetes mellitus. Poorly controlled diabetes and active tobacco use are indicative of poor wound healing following oncoplastic surgery. Cardiac and pulmonary disease are also important given that these procedures are usually performed under general anesthesia, and good health will promote safe surgery.
Understanding patient expectations is a critical component of all breast surgery and especially oncoplastic breast surgery. It is important to appreciate how a patient feels about her breasts before the diagnosis of breast cancer and what she would like modified. This may pertain to breast volume, shape, symmetry, contour, nipple position, or diameter of the NAC. It is important to explain that oncoplastic breast surgery is performed more often on women with mammary hypertrophy; however, women with normal or small volume breasts can also have oncoplastic procedures. Studies evaluating complications, recurrence, and patient satisfaction following breast conservation, oncoplastic reduction mammaplasty, and oncoplastic flap reconstruction have demonstrated increased satisfaction and fewer recurrences and complications with oncoplastic procedures compared with breast conservation alone.
Technique Consideration
When considering the options for oncoplastic surgery, it is important to recognize that there are two fundamental strategies that include volume displacement and volume replacement. These are typically performed independently but can be performed together. Volume displacement techniques include reduction mammaplasty, mastopexy, and adjacent tissue rearrangement. Volume replacement includes the use of remote flaps such as a thoracodorsal artery perforator or a latissimus dorsi flap as well as the use of implants in select cases. Volume replacement techniques are the most common form of oncoplastic reconstruction with reduction mammaplasty being the workhorse. These operations can be performed immediately following the partial mastectomy or on a staged bases following confirmation of clear pathological margins.
The classic candidate for oncoplastic breast surgery is the patient with mammary hypertrophy because the breast cancer and adjacent parenchyma can be removed and easily reconstructed without resulting in a complex deformity. These patients are usually reconstructed using techniques of adjacent tissue rearrangement that includes reduction mammaplasty, mastopexy, or parenchymal undermining and advancement. Performance of these operations requires a thorough understanding of the vascular anatomy of the breast.
Reduction Mammaplasty with Parenchymal Flaps
In women with mammary hypertrophy, reduction mammaplasty coupled with parenchymal flaps to fill the partial mastectomy defect is the most common variant of oncoplastic reconstruction. It is important to recognize that an oncoplastic reduction mammaplasty is very different from a standard reduction mammaplasty. With a standard reduction mammaplasty, the skin and parenchyma are usually excised in a symmetric and balanced method, and the NAC is transposed on a vascularized pedicle. With an oncoplastic reduction, a partial mastectomy defect is created that will need to be filled with a parenchymal flap that is sometimes different from the parenchymal flap used to transpose the NAC. Many patients will choose to have the oncoplastic procedure coupled with a contralateral reduction mammaplasty. In these situations, it is common to perform a completely different operation on the cancerous and noncancerous breast; however, the goal is to achieve final volume and contour symmetry.
Creation of parenchymal flaps can be challenging and requires an understanding of the anatomy and tissue perfusion. It is especially important to recognize that the vascularity to the parenchyma and skin are distinctly different and that multiple variations are possible. The location and size of the defect will dictate the location and size of the parenchymal flap. The orientation of the parenchymal flap typically depends upon the location of the defect. In general, parenchymal flaps are oriented opposite to the defect such that a superior breast defect would be typically reconstructed with an inferiorly based flap. Detaching the distal segment of the parenchymal flap from the chest wall to adequately rotate it and fill the defect without tension facilitates mobilization. It is important to constantly assess the perfusion to the parenchymal flap to maintain its vascularity; thus, it is critical to minimize the extent of detachment. Perfusion can be assessed clinically by noting arterial and venous bleeding from the distal edges and, if questionable, by using fluorescent angiography.
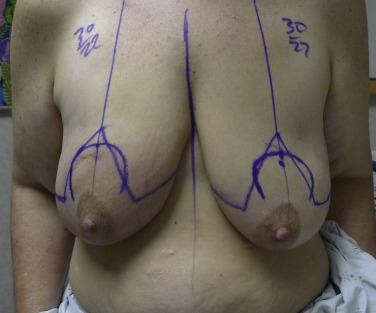
Once the flap has been adequately mobilized, it is inset into the breast defect and sutured in place. The perimeter of the chest wall defect is tagged with surgical clips or staples to facilitate identification of the tumor bed for the radiation oncologist. Once complete, the next step is to decide how much additional breast skin and parenchyma needs to be excised to create a natural breast contour. This will depend upon the skin pattern utilized. It is advised to keep the cancer side approximately 10% larger than the contralateral because of radiation-related shrinkage of the breast over time. Closed suction drains are routinely placed in these cases because of the flap mobilization and to maintain negative pressure in the space to promote flap adherence. Figs. 6.1–6.5 illustrate a patient having a right oncoplastic reduction mammaplasty and an immediate contralateral reduction mammaplasty for symmetry.
Related posts:
 Indications and Patient Selection for Oncoplastic Breast Surgery
Indications and Patient Selection for Oncoplastic Breast Surgery
 Oncoplastic Breast Surgery and the Effects of Radiation Therapy
Oncoplastic Breast Surgery and the Effects of Radiation Therapy
 Breast Augmentation Technique (Biplanar) for Oncoplasty
Breast Augmentation Technique (Biplanar) for Oncoplasty
 Surveillance and Imaging Following Oncoplastic Breast Surgery
Surveillance and Imaging Following Oncoplastic Breast Surgery
 Volume Displacement and Volume Replacement Techniques
Volume Displacement and Volume Replacement Techniques
 Complications of Oncoplastic Breast Surgery
Complications of Oncoplastic Breast Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


