Introduction
The desire of many patients to preserve their breasts regardless of the cosmetic outcome has led to a more aggressive use of partial mastectomy, with more extensive local resections being classified in the category of partial mastectomy. As partial mastectomies become more extensive, the risk of suboptimal cosmetic results from such resections is likely to increase. In recent years, the proportion of breast cancer patients treated with partial mastectomy and radiation therapy (XRT) has increased. This approach is referred to as breast conservation therapy (BCT). This trend is due in part to increased mammographic screening, with a corresponding increase in the detection of early breast cancers. It is also due to the increasing use of preoperative chemotherapy in patients with large operable and locally advanced breast cancer, where significant clinical responses can allow for breast-preserving procedures in patients who would otherwise have required a mastectomy. After BCT, 20–30% of patients are reported to have a poor cosmetic result, with deformities of the treated breast. However, poor cosmetic outcomes after BCT are likely to be underestimated in the literature because many patients with poor outcomes are reluctant to seek further surgical treatment.
In this chapter, we present a management algorithm for repair of partial mastectomy defects based on clinically relevant parameters that should allow the clinician to better select the most appropriate patient indications for the various reparative surgical techniques.
Management algorithm for repair of partial mastectomy defects
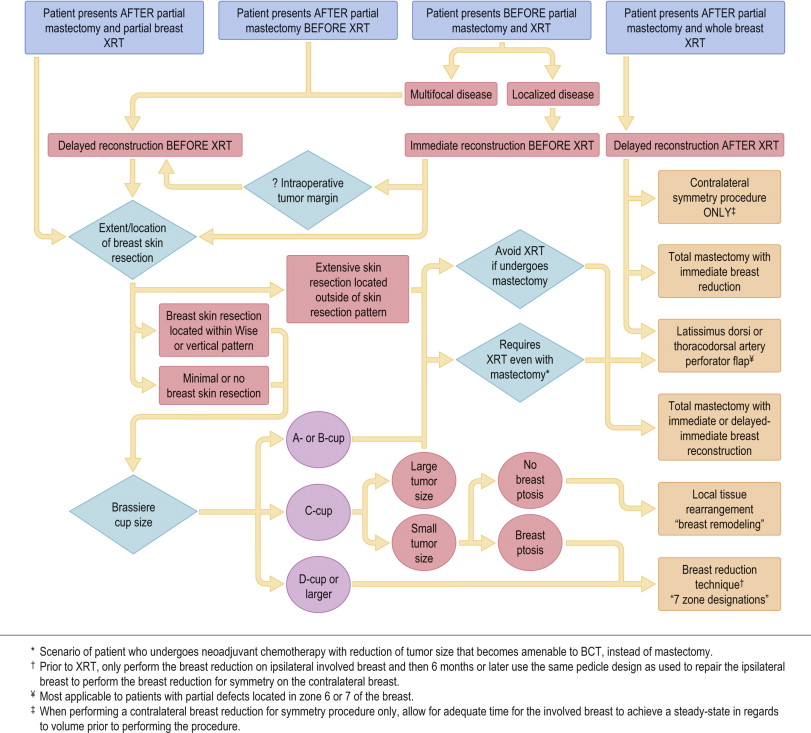
It is well appreciated that most reconstructive breast procedures are based on principles and concepts, not on structured guidelines. The proposed management algorithm presented in Fig. 3.1 has been designed to serve as a guide to assist in the decision-making process for repairing partial mastectomy defects. However, the final decision regarding the optimal approach is ultimately made by the multidisciplinary breast cancer treatment team and the patient.
Importance of timing of repair in relation to XRT
Waiting to repair a large partial mastectomy deformity until completion of whole-breast XRT usually necessitates the complex transfer of a large volume of autologous tissue. Patients who choose BCT often do so to limit the extent of surgery and therefore they are not eager to undergo a major secondary reconstructive procedure. In addition, the difficulties associated with secondary repair within an irradiated surgical field limit the use of the adjacent irradiated breast tissue because of high complication rates. The use of prosthetic devices in this setting has been fraught with increased morbidity and is not usually recommended. With the increasing use of partial breast irradiation as an alternative to whole-breast irradiation, the use of the remaining breast tissue for reconstruction may become a viable option for these patients.
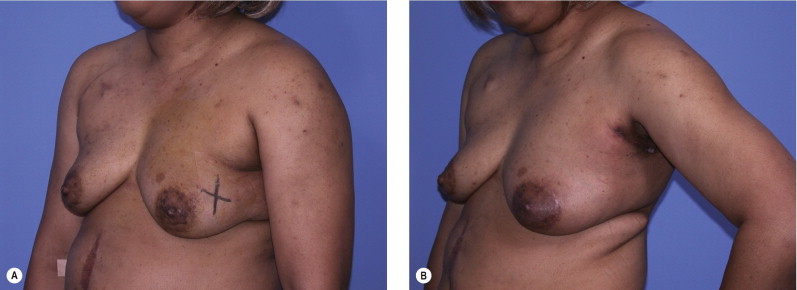
Delayed reconstruction after XRT usually requires a latissimus dorsi or thoracodorsal artery perforator flap; however, use of these flaps may increase the likelihood of arm lymphedema and may leave the patient without an autologous tissue option if further reconstruction is required in the future. At the MD Anderson Cancer Center, the role of local pedicle flaps in the repair of partial mastectomy defects has been changing. Although these flaps are still the most commonly used flaps for delayed repairs after XRT, they are now being used more frequently for immediate repairs before XRT (after confirmation of negative tumor margins). These flaps have been demonstrated to be useful in small and moderate-volume breasts and in patients who present with locally advanced breast cancer that will require XRT, whether they undergo a partial mastectomy (i.e., become eligible for BCT after neoadjuvant chemotherapy) or total mastectomy ( Fig. 3.2 ).
In some patients who have completed XRT, a contralateral breast reduction alone, without repair of the involved breast, will improve breast symmetry. The advantage of this strategy is that the radiated breast is not operated on, thus eliminating the possibility for additional morbidity. The extent of the surgical procedure is limited and reasonable breast symmetry can be achieved.
In the case of a severe breast deformity following BCT, the option of a completion mastectomy with total reconstruction is considered. The cosmetic outcomes of total breast reconstruction after BCT are less than optimal, primarily because of the relative inelasticity of the irradiated breast skin envelope and the increased risk of mastectomy skin flap necrosis.
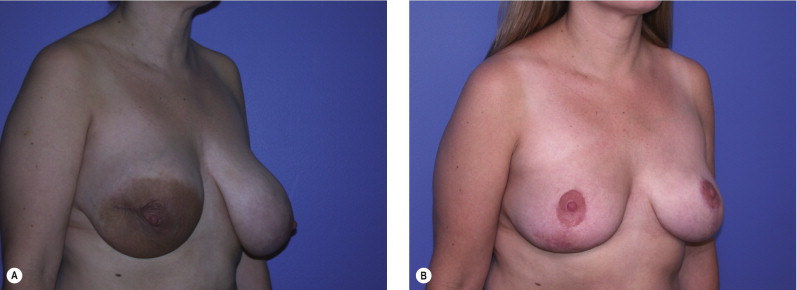
At the MD Anderson Cancer Center, the most frequently used technique for repairing the partial mastectomy defect is to use local breast tissue. This is primarily because of the simplicity of these approaches and also because these techniques using local tissue will usually maintain the color and texture of the breast. If, however, an unexpected deformity results after partial mastectomy ( Fig. 3.3 ) or the tumor margin status is unclear at the time of the partial mastectomy, consideration should still be given to performing the repair prior to XRT. In these circumstances, we prefer to use the remaining breast tissue for local reconstruction.
Related posts:
 Reduction Mammaplasty and Oncoplastic Surgery
Reduction Mammaplasty and Oncoplastic Surgery
 Timing and Key Considerations in Reconstruction for Breast-Conserving Therapy
Timing and Key Considerations in Reconstruction for Breast-Conserving Therapy
 Breast Augmentation Technique (Biplanar) for Oncoplasty
Breast Augmentation Technique (Biplanar) for Oncoplasty
 Surveillance and Imaging Following Oncoplastic Breast Surgery
Surveillance and Imaging Following Oncoplastic Breast Surgery
 Volume Displacement and Volume Replacement Techniques
Volume Displacement and Volume Replacement Techniques
 Complications of Oncoplastic Breast Surgery
Complications of Oncoplastic Breast Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


