In this chapter, we will lay out the rationale for screening mammograms to start at age 40 and continued annually until age 70, at which time biannual imaging should be performed until life expectancy is less than 5 years, or a patient refuses intervention of any kind. Exceptions for high-risk patients are addressed later in the chapter. We will also list the current guidelines and recommendations set forth by our leading societies
Overview
In the United States, the 5-year survival rates for women with breast cancer have improved from 75% in 1975–1977 to 90% in 2003–2009. The risk of distant or metastatic disease and death increases with both tumor size and number of axillary lymph nodes involved. Although mammography is not a perfect test and may be particularly insensitive at detecting breast cancer among selected groups of patients, such as those with very dense breasts, extensive scaring from previous interventions (such as surgery and radiation), or those with a subtype of malignancy that is often harder to detect on imaging such as invasive lobular carcinoma, it remains effective at finding smaller tumors before they are palpable. When measuring the benefit of an intervention, as when measuring the harm, survival should not be the only measure of efficacy. After tumor size and lymph node involvement, survival is strongly influenced by tumor-related factors such as hormone receptor and human epidermal growth factor receptor 2, (HER-2) status, and grade. Screening mammography is effective at finding more (not all) cancers earlier, before they are palpable, and thereby reducing the number of women with cancers of advanced size and stage. Finding cancers at an earlier stage allows for better outcomes, more lives saved, and potential for both less extensive surgery and either no or potentially less extensive chemotherapy. Thus, mammography meets the criteria of an effective screening test: (1) detects disease at a stage when an intervention can make a difference, and (2) is affordable, accessible, and does not cause more harm than good.
Imaging in Women 40–70 Years of Age
Breast cancer is common, affecting about 1 in 8 women (12.5%) with more than 260,000 new cases per year in the United States. As of January 2018, there were more than 3.4 million women either with a history of breast cancer or being treated for breast cancer in the United States alone. Less than 1% of breast cancers develop in men. Not including benign breast biopsies and cosmetic breast surgery, there are more than a half-million breast cancer-related surgeries performed per year in the United States. In spite of all this breast cancer surgery, breast imaging recommendations remain controversial, with the United States Preventive Services Task Force (USPSTF) recommendations differing, in varying degrees, from most of our other guiding bodies: American College of Radiology (ACR), American Cancer Society (ACS), and American Society of Breast Surgeons (ASBrS)/Society of Surgical Oncology (SSO).
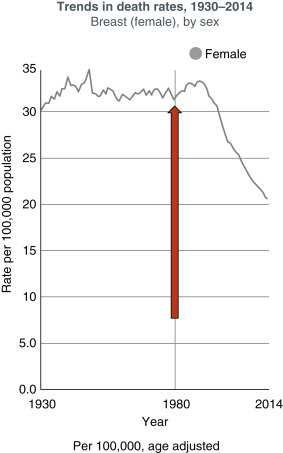
In part, the controversy arises secondary to the fact that breast cancer is not only common, it is potentially deadly but not uniformly so. Breast cancer represents about 20% of all cancers (men and women) and is the second most common cause of cancer death among women overall. This number continues to improve in women over 50, with breast cancer deaths having dropped by approximately 37% between 1989–2015 in this population ( Table 19.1 , with annex). Breast cancer screening guidelines from the various cancer organizations are listed in tables 19.2-19.4 . However, in women under 50, the death rate has remained steady since 2007. Data has also shown that younger women are more likely to develop more aggressive malignancies (HER2-positive and hormone receptor-negative) with higher risk of both distant and local recurrence.
| Population | Recommendation | Grade (What’s This?) |
|---|---|---|
| Women aged 50—74 years | The USPSTF recommends biennial screening mammography for women aged 50—74 years. | B |
| Women aged 40—49 years | The decision to start screening mammography in women prior to age 50 years should be an individual one. Women who place a higher value on the potential benefit than the potential harms may choose to begin biennial screening between the ages of 40 and 49 years.
| C |
| Women aged 75 years or older | The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening mammography in women aged 75 years or older. | I |
| All women | The USPSTF concludes that the current evidence is insufficient to assess the benefits and harms of digital breast tomosynthesis (DBT) as a primary screening method for breast cancer. | I |
| Women with dense breasts | The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of adjunctive screening for breast cancer using breast ultrasonography, magnetic resonance imaging, DBT, or other methods in women identified to have dense breasts on an otherwise negative screening mammogram. | I |
| Grade | Definition | Suggestions for Practice |
|---|---|---|
| A | The USPSTF recommends the service. There is high certainty that the net benefit is substantial. | Offer or provide this Service. |
| B | The USPSTF recommends the Service. There is high certainty that the net benefit is moderate or there is moderate certainty that the net benefit is moderate to substantial. | Offer or provide this Service. |
| C | The USPSTF recommends selectively offering or providing this Service to individual patients based on Professional judgment and patient preferences. There is at least moderate certainty that the net benefit is small. | Offer or provide this Service for selected patients depending on individual circumstances. |
| D | The USPSTF recommends against the Service. There is moderate or high certainty that the Service has no net benefit or that the harms outweigh the benefits. | Discourage the use of this Service. |
| I Statement | The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of the Service. Evidence is lacking, of poor quality, or conflicting, and the balance of benefits and harms cannot be determined. | Read the clinical considerations section of USPSTF Recommendation Statement. If the Service is offered, patients should understand the uncertainty about the balance of benefits and harms. |
| Risk | Age | Recommendation |
|---|---|---|
| Average | 40-44 | Shared decision-making process for women to elect screening |
| Average | 45–54 | Annual screening |
| Average | Over 55 | Biennial screening |
| Elderly | Continued screening as long as life expectancy greater than 10 years |
- •
History of breast cancer
- •
Genetic mutation
- •
History of chest XRT
| Risk | Age | Recommendation |
|---|---|---|
| High Chest radiation before 30 | Age 25 or 8 years after radiation | Annual screening |
| High-genetic based increased risk and their untested 1st degree relatives, those with >20% lifetime risk | 25–30 | Annual mammogram and consider MRI |
| High personal history of breast cancer | Start at diagnosis or 40 whichever comes first | Annual mammogram and if <50 consider MRI |
| High personal history of ADH, ALH | 40 | Annual screening and consider MRI especially if other risk factors are present |
| Average | 40–75 | Annual screening |
| Average | Elderly | Annual screening until life expectancy less than 5–7 years |
| Risk | Age | Recommendation |
|---|---|---|
| Average | 40–44 | Consider screening based on a discussion of risks and benefits |
| Average | 45–54 | Annual screening mammograms |
| Average | 55 and older | Annual or biennial screening for women 55 and older based on a shared decision |
| Average | Older than 75 with life expectancy greater than 10 years | Biannual screening mammogram |
| Asymptomatic Intermediate Risk | 40 and older | Consider use of annual screening mammography for women with greater than an estimated 15% lifetime risk for breast cancer |
| Asymptomatic High Risk | 10 years younger than the 1st degree relative, or 10 years after chest wall XRT, or by age 40, whichever comes first | Recommendations for asymptomatic high-risk women (20–25% or greater estimated lifetime risk) annual mammography and MRI compliant with ACS and NCCN guidelines |
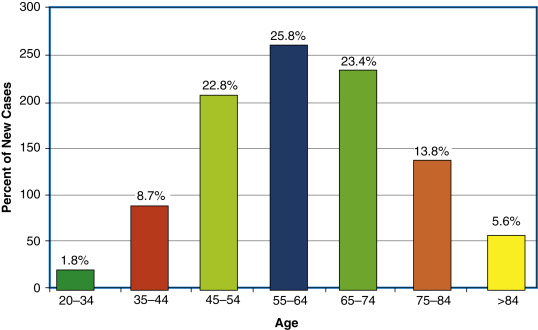
Breast cancer is often thought of as a disease of the elderly, which is not untrue ( Figs. 19.1 and 19.2 ). However, this is a very limited picture of the true impact and distribution of the disease. Breast cancer is most commonly diagnosed in middle-aged women with a broad distribution extending to the young adult and the very old. As stated earlier, the “lifetime” risk of developing breast cancer is 1 in 8 women, with 25.9% of all breast cancers diagnosed between the ages of 55 and 64 with an average age of 62 at diagnosis (see Fig. 19.2 ). However, it is extremely important to note that there is an almost equal distribution 10 years above and below this, with 20.4% of women diagnosed between 45–54 years of age and 24.1% diagnosed between 65–74 years of age. Context remains extremely important as seen in Fig. 19.3 , with lifetime risk seen to be highest in women age 80; however, the age at which a large number of women are diagnosed is 62 (see Fig. 19.3 ). Again, we must note that survival improves with earlier stage at diagnosis; 5 years survival for stage I breast cancer is 98.7% compared with 27% for metastatic disease.
Related posts:
 Indications and Patient Selection for Oncoplastic Breast Surgery
Indications and Patient Selection for Oncoplastic Breast Surgery
 Oncoplastic Breast Surgery and the Effects of Radiation Therapy
Oncoplastic Breast Surgery and the Effects of Radiation Therapy
 Plastic Surgeon’s Approach to Oncoplastic Breast Surgery
Plastic Surgeon’s Approach to Oncoplastic Breast Surgery
 Extreme Oncoplasty
Extreme Oncoplasty
 Volume Displacement and Volume Replacement Techniques
Volume Displacement and Volume Replacement Techniques
 Complications of Oncoplastic Breast Surgery
Complications of Oncoplastic Breast Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


