Introduction
Breast conservation therapy (BCT) has become the mainstay in surgical breast oncology practice and is now a routine technique for the treatment of early-stage cancers. Improvements in diagnostic technology and mammographic screening as well as increased use of preoperative local and systemic therapies have extended the indications for BCT, with reported rates of 58% in the UK and 60–75% in the United States. Although BCT has enabled a less extensive tissue resection consisting of lumpectomy with tumor-free margins followed by radiation therapy, major contour irregularities have been observed following these procedures. Poor cosmetic results of BCT have been reported in 5–40% of patients. The surgical dead space created from the lumpectomy defect with added postoperative radiation effects may sometimes lead to substantial distortions in breast shape and size as well as nipple position. The management of breast deformities secondary to BCT in such cases can pose considerable difficulties, particularly when operating in a radiated field with poor tissue compliance. Several oncoplastic breast surgery techniques were introduced in an attempt to optimize the balance between the risk of local recurrence and the cosmetic outcome in BCT. The combined plastic surgery techniques of tissue replacement or tissue rearrangement involve a wider local excision while achieving enhanced breast shape and symmetry, and reduced surgical dead space.
Patients with small volume breast and relative large lumpectomy volume are at risk of developing severe breast deformity and breast asymmetry following BCT, thus presenting a unique surgical challenge. Regional flaps can be used to replace the volume loss in small-breasted patients, but many of them are reluctant to undergo this procedure due to additional scarring and morbidity, leading them to forgo oncoplastic reconstruction altogether or to undergo mastectomy and immediate reconstruction. The use of a prosthetic device for volume replacement in small breasts may seem appealing, but it has been largely rejected on the basis of studies that cited high complication rates following radiation therapy. One such study showed that subcutaneous implant placement in the immediate setting led to high incidences of capsular contracture and other complications. Nevertheless, there is reason to believe that with increasing surgical expertise and improved radiation delivery methods, implant-based procedures in patients planned for radiation therapy might have a better outcome compared with earlier experience. Judicious selection of the radiotherapy technique can reportedly help to improve the dose distribution and cause fewer radiation-induced side effects. Recent studies have advocated immediate implant-based reconstruction for patients receiving post-mastectomy radiotherapy, especially those who may not be candidates for autologous reconstruction. Moreover, patients with previous breast augmentation who later undergo BCT were reported to have good to excellent outcomes following their radiation treatment.
With growing experience and refinement in breast tissue rearrangement techniques, together with implant-based reconstruction and modern radiation therapy methods, more consistent results may be offered to breast cancer patients with small volume breasts who are considering BCT by means of the oncoplastic biplanar breast augmentation technique. This technique consists of immediate local glandular tissue rearrangement after a lumpectomy procedure and the use of bilateral subpectoral breast augmentation of different size and projection implants to compensate for the lumpectomy-caused volume loss. The technique aims to achieve immediate correction of shape and volume before radiotherapy without the added morbidity associated with the use of autologous flaps or delayed BCT reconstructions.
Patient Selection
Patient selection is processed through the multidisciplinary breast team, after reviewing all relevant breast imaging studies and after planning the surgical scars and resection area based on tumor size and location. It is essential to ensure that all patients are motivated to enhance their breasts, and that they understand that the possible effects of radiation therapy on the implant range from negligible to severe capsular contracture and breast deformity. Currently, we have no way to predict which patient will do well after radiation.
Indications and Contraindications
Indications for the oncoplastic biplanar breast augmentation technique include patients scheduled for BCT who have small and non-ptotic breasts (bra cup A–B), with relatively large tumors that could not be addressed by local tissue rearrangement alone. Tumor size should be smaller than 25% of the total breast volume. Preferences for tumor location include the upper pole of the breast, above a horizontal line at the lower areolar position. Lower-positioned tumors, especially near the inframammary fold area, are close to the pocket of the implant, thus making it difficult to dissect separate tumor implant pockets. For these selected cases of lower-pole breast tumors, an acellular dermal matrix (ADM) graft can be used to reinforce the lower pole of the breast and improve the separation between the implant and the lumpectomy pockets.
Patients with previous breast augmentation are also candidates for this technique. The implant on the affected side is exchanged for a larger one in order to compensate for the lumpectomy volume loss. Implants in a previous subglandular position are exchanged for a subpectoral dual plane pocket.
Patients with tumor involvement of the nipple–areolar complex (NAC), distant metastasis, or tumors growing into the chest wall or skin (oncologic stage T4) are not candidates for this technique.
Operative Approach ( )
The patient is marked in a manner similar to a breast augmentation procedure, with the addition of the area of the planned lumpectomy. After prepping and draping the supine patient, the breast surgeon performs a wire-guided lumpectomy ( Fig. 12.1A ). The incision of choice is periareolar, with an incision extension if needed. For cases in which the tumor is not centrally located, the surgeon performs a radial or an arched incision over the tumor area. The tumor is removed, marked, weighed, and sent to mammography and pathology. Additional tissue extensions are taken from the tumor bed, and the space is marked with metal hemostatic clips ( Fig. 12.1B ). The lymph node procedure is performed from a separate axillary incision.
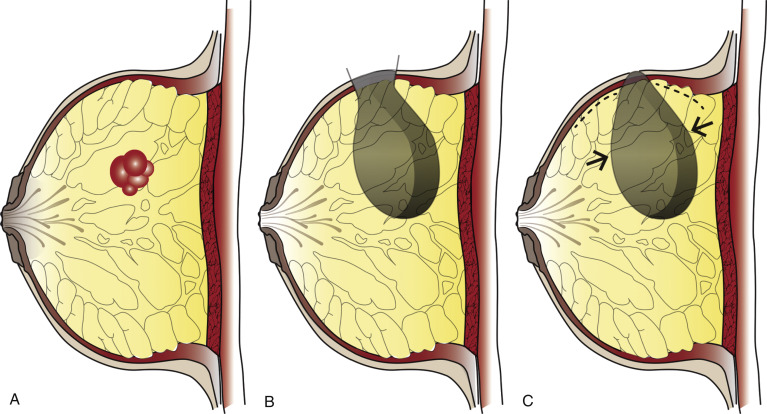
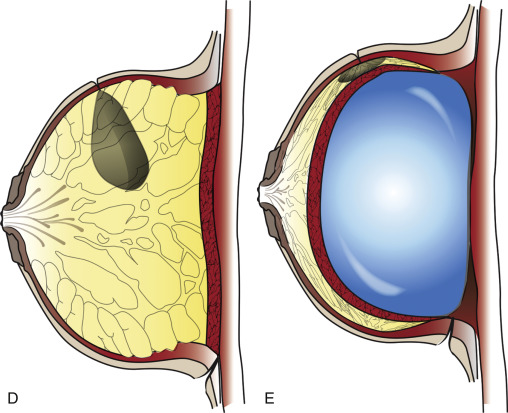
After irrigation and careful hemostasis, the tumor bed is inspected and tissue approximation is performed by local tissue advancement. Further limited undermining of the breast parenchyma or the skin flaps is occasionally necessary before the glandular tissue can be approximated ( Fig. 12.1C ). Care is taken to limit the undermining of the tissue and approximate it with minimal tension to prevent fat necrosis. The skin is sutured ( Fig. 12.1D ), and a new and separate incision is made in the inframammary fold. Then, a new and separate pocket is dissected in the subpectoral plane, taking care that there is no direct connection to the tumor bed. A subpectoral pocket is formed on the contralateral healthy breast as well. Breast implant sizers are inserted, and the larger implant with higher projection is chosen for the breast that underwent lumpectomy to match it to the contralateral breast. The patient is then placed in a seated position for intraoperative assessment of symmetry and for further adjustments. Permanent silicone implants are selected and inserted after irrigation and hemostasis ( Fig. 12.1E ). In cases of previous augmentations, the incision is made in the inframammary scar, old implants are removed, and a new subpectoral pocket is dissected after partial capsulectomy. No drains are used for the breast surgery itself, but a drain is placed in the axilla for patients who had undergone axillary lymph node dissection.
Related posts:
 Indications and Patient Selection for Oncoplastic Breast Surgery
Indications and Patient Selection for Oncoplastic Breast Surgery
 Oncoplastic Breast Surgery and the Effects of Radiation Therapy
Oncoplastic Breast Surgery and the Effects of Radiation Therapy
 Plastic Surgeon’s Approach to Oncoplastic Breast Surgery
Plastic Surgeon’s Approach to Oncoplastic Breast Surgery
 Surveillance and Imaging Following Oncoplastic Breast Surgery
Surveillance and Imaging Following Oncoplastic Breast Surgery
 Volume Displacement and Volume Replacement Techniques
Volume Displacement and Volume Replacement Techniques
 Complications of Oncoplastic Breast Surgery
Complications of Oncoplastic Breast Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


