Summary and key features
Skin resurfacing and tightening procedures are widely sought after, safe, and effective.
Review of skin resurfacing technologies, including lasers, light and energy devices, chemical peels, microneedling, and plasma.
Appropriate patient selection and setting realistic expectations are paramount to optimizing outcomes and minimizing complications.
Introduction
For centuries, individuals have sought to achieve and maintain a youthful appearance. According to a recent survey by the American Society of Dermatologic Surgery (ASDS), primary cosmetic concerns include: static and dynamic facial lines, or rhytides, submental fullness, photoaging, and dyschromia. Treatments that tighten skin, or smooth wrinkles, are among the most popular procedures performed amongst these patients. Patients report opting to undergo these treatments to feel more confident, appear more attractive, and restore a youthful appearance.
Laser resurfacing is a safe, effective procedure most commonly performed for the treatment of photoaging, including fine lines, dyschromia, and skin tightening.
History
Lasers are the most commonly used devices to achieve rejuvenation and are key to the dermatologic surgeon’s armamentarium. These technologies have been developed around the understanding of the principle of selective photothermolysis. More specifically, lasers of specific wavelengths and pulse durations deliver energy that is selectively absorbed by chromophores in the skin (i.e., melanin, hemoglobin, and water).
Early devices primarily targeted hemoglobin as the chromophore to initiate skin rejuvenation. Water is the target chromophore for many ablative and nonablative resurfacing devices; laser energy results in thermal heating, wound healing, and collagen formation. A wavelength preferentially absorbed by water, emitted by carbon dioxide lasers (10,600 nm), allowed these devices to quickly become the mainstay in the early years of skin resurfacing. CO 2 lasers provide potentially remarkable clinical outcomes, but are accompanied by prolonged recovery periods and a higher risk of complications.
The 2940 nm Er:YAG, with a greater absorption coefficient as compared to CO 2 , offers excellent outcomes by selectively targeting the epidermis while decreasing the side-effect profile. However, due to more superficial photothermolysis, Er:YAG lasers are less effective than CO 2 lasers in providing hemostasis and coagulation. Furthermore, they may be a poor choice in cases where deep dermal remodeling is required.
Ablative, continuous wave devices proved themselves to be effective, but their associated long downtimes and side-effect profiles prompted the research and development of nonablative resurfacing devices. While nonablative devices afforded better side-effect profiles and recovery, as well as the opportunity to treat individuals of darker skin types and nonfacial areas, the clinical outcomes initially noted were less impressive.
The theory of fractional photothermolysis, in which lasers create a pattern of evenly spaced zones of alternating treated nonablative injury and untreated areas soon followed. This was revolutionary: prior to this treatment pattern, ablative and nonablative devices targeted the entire field within their incident beam profiles. Many fractional devices of both ablative and nonablative wavelengths are currently available, offering superior patient experiences as compared to their traditional unfractionated predecessors. An additional benefit is an improved side-effect profile over traditional ablative devices. Fractional lasers have become the gold standard in laser skin resurfacing and tightening.
More recently, energy devices using longer wavelengths for deeper penetration have been explored to achieve skin tightening. A few of these technologies, developed using radiofrequency and ultrasound, bypass the epidermis and papillary dermis, elevate local temperature, induce collagen contraction, and thereby stimulate neocollagenesis. , Microneedling, with and without radiofrequency, has also been shown to have benefits in skin resurfacing and tightening. Additional tightening devices, such as cold plasma, create excited-state ionized gas that delivers superficially focused energy to the skin and stimulates neocollagenesis.
Chemical peels have been used for rejuvenation purposes since Ancient Egyptian times. Ferdinand Hebra, a Viennese dermatologist, used various exfoliative agents, such as croton oil, to treat ephelides and melasma in the mid- to late 1800s. Phenol, trichloroacetic acid, salicylic acid, and resorcinol peels were extensively described in the late 1880s. Many of these agents are still used with varying concentrations, application techniques, and protocols to achieve desired cosmetic results.
There continues to be research, development, and introduction of new technologies and devices that resurface the skin, including ultrasound, radiofrequency, microneedling, and cold plasma.
Patient selection
An in-depth discussion of the cosmetic evaluation of a patient is outside the scope of this chapter; continued development and improvement of this skillset are of paramount importance. A consultation is essential for appropriate patient selection, playing a key role in performing successful cosmetic procedures. Patient conversations and experiences will differ, as some individuals present with specific concerns, whereas others have general complaints. It is critical to identify and explore the patient’s expectations while considering the potential risks, benefits, and alternatives of the procedures discussed. In addition to a thorough medical, surgical, medication, and allergy history, procedure-related topics to discuss include downtime, number of treatments anticipated, and expected outcomes. When possible, it is prudent to provide patients with photographs of prior results and/or testimonials to improve their understanding of anticipated results.
Ensuring appropriate patient selection is crucial and can be achieved through comprehensive communication about the procedure and establishing realistic expectations.
Treatment cannot be performed by using a “cookbook” or guide with settings and indications. One must understand clinical endpoints and gain experience through device use.
Preoperative assessment
Performing a thorough assessment prior to the cosmetic treatment encounter minimizes the risk of complications. Start by eliciting a complete medical/surgical history, including any past and/or interim history of cosmetic procedures. The history should help elucidate what procedures a patient has had, including specific devices and when they were performed. The history of certain procedures may preclude or serve as a contraindication to future ones. Furthermore, it is prudent to tailor the consultation based on the patient’s experience with previous cosmetic procedures, including adverse events, unintended outcomes, or complications. A history of recurrent cosmetic procedures or excess concern for flaws that are out of proportion to one’s physical appearance and cause significant distress or impairment in functioning should prompt one to consider body dysmorphic disorder in addition to other underlying psychosocial conditions.
A thorough review of the patient’s medical history should be completed regarding: infectious diseases (hepatitis B/C, herpes simplex virus [HSV], and human immunodeficiency virus [HIV]), history of keloids or aberrant wound healing, history of radiation therapy, skin cancer, immunocompromised states, recent surgery, and postoperative wound infections. If the patient admits to one or more of the above, consider postponing or avoiding the procedure, depending on the concern and timing. Common infectious disease concerns include patients with a history of HSV infection; they should be given viral prophylaxis. If there is concern for bacterial infection, antibacterial prophylaxis should be administered. Prophylactic regimens vary in therapeutic agent, application, and dosing depending on the physician experience. Author RT prefers to use 500 mg of valacyclovir twice a day, starting the day before the procedure continuing for 5 days. Since ablative resurfacing lasers may interfere with the skin barrier function, it is often prudent to start the patient on an antibiotics prophylactically. Cephalexin 500 mg PO BID for 5 days or Doxycycline monohydrate 100 mg PO BID for 5 days are the favored regimens used by the author HK. In acne prone individuals Doxycycline may be continued for 90 days.
Relative and absolute contraindications for the various devices depend greatly on the mechanism of action. Herein we discuss a few noteworthy relative contraindications. A personal history of photosensitizing disorders or isotropic conditions such as systemic lupus and discoid lupus are relative contraindications to laser and light-based devices. Pregnancy status of all female patients must be known and documented. Recent evidence limited to case series/reports indicate that cutaneous laser treatment is safe for both mother and fetus. However, it is the collective opinion of the authors that elective procedures should not be performed during pregnancy. Breastfeeding is not a contraindication to laser treatments provided the topical lidocaine is applied on a small surface area such as the face.
Once the patient elects to proceed with a given treatment, it is critical to discuss key elements pertaining to the procedure. Foremost, an informed consent approved by the risk management/legal team, containing discussion of the risks, benefits, and alternatives, must be in place. The consent should be completed prior to medicating or treating the patient.
An extensive review of all medications, including over-the-counter vitamins and supplements is highly recommended. On the medication list, the greatest concern are anticoagulants and immunosuppressive medications that confer inherent treatment risks. Over-the-counter supplements and vitamins can contribute to bleeding risk and contain adulterants with unknown side effects. Substances that increase bleeding risk should be avoided, if not medically necessary, at least 1 week prior to the procedure. Examples of these substances include aspirin, ibuprofen, vitamin E, alcohol, fish oil, garlic, ginko, warfarin, and turmeric. If the patient chooses to remain on these medications/supplements, it is important to counsel patients on the risk of increased bleeding, bruising, and poor wound healing.
All patients should be asked about their history of isotretinoin use within the preceding 6 months, as this is a relative contraindication to fully ablative laser rejuvenation. However, a recent review suggests this may not be necessary for less-invasive resurfacing or tightening modalities (e.g., nonablative). Based on a study by Kim et al, patients undergoing fractional ablative CO 2 resurfacing can be prescribed a low-dose isotretinoin of less than 0.5 mg/kg/day to be taken preoperatively to avoid acne recurrence during the re-epithelialization period following the laser resurfacing. Author EL has performed ablative, nonaggressive, CO 2 fractional resurfacing on patients taking low dose accutane (less than 0.5 mg/kg) since 2006 without any complications.
Alcohol and tobacco use should ideally be ceased prior to the procedure. Firm, evidence-based guidelines are nonexistent on an exact timeframe for substance avoidance. Anecdotally, alcohol is avoided 2 days before and 2 days after the procedure to minimize bleeding/bruising risk. Smoking is avoided for 6 weeks before and 6 weeks after the procedure to optimize wound healing. Beyond social history, it is recommended to assess and document known food and drug allergies to prevent undesired effects.
A physical examination of the area is a vital component of the preoperative assessment. Determination of the patient’s Fitzpatrick phototype should be a part of the skin examination, as well as making note of active skin infection or inflammation in the area of treatment. Presence of these conditions is considered a relative or an absolute contraindication to treatment.
Skin of color patients are at a higher risk of experiencing complications from cosmetic procedures (i.e., lasers, energy-based devices, and chemical peels). It is postulated that these complications occur due to direct melanosome disruption as well as indirect injury, such as postinflammatory pigment alteration. Patients may benefit from having a pre-treatment test spot performed to optimize parameters while minimizing the risks of potential side effects.
Evaluation for asymmetries, scarring, and other obvious lesions should be completed and noted prior to treatment. Before and after the procedure, photographs should be obtained, and relevant findings must be shown to the patient. Other important factors prior to treatment, when relevant, include: sebaceous gland content, hair content/quality, the presence of dynamic/static rhytides, as well as skin laxity. When resurfacing or skin tightening procedures are undertaken in the periorbital and perioral regions, it is essential to document the presence of lid lag, ectropion, or eclabium.
Two to 6 weeks prior to treatment, suggested topical skin care regimens may be initiated and established to optimize treatment results. When appropriate, for patients at greater risk for dyspigmentation, the application of topical hydroquinone, Kojic Acid, non-hydroquinone lightening agents, and retinol products have been proposed. Although hydroquinone is widely used to prevent dyschromia, it has not definitively demonstrated efficacy in controlled trials. Pregnant or breastfeeding patients should avoid using hydroquinone. Sunscreen use, sun protective behaviors, and sun avoidance must be emphasized to reduce treatment-related dyspigmentation.
Dr. khorasani’s compounded bleaching cream for patients prone to post inflammatory hyperpigmentation:
Ingredients:
Hydroquinone 6%
Kojic Acid 6%
Vitamin C 2%
Vitamin E 2%
Green Tea Extract 2%
Hydrocortisone 0.5%
Instructions for use:
Start using 4 weeks prior to your laser
Start every other night the first week
Always apply prescribed serum and moisturizer before applying the bleaching cream
Use pea size amount
Always use sunscreen even if always indoors
Arnica is an over-the-counter oral and topical supplement that may reduce swelling and erythema. Topical formulations have been shown to decrease post-procedure bruising, but the evidence is mixed.
Pain management is an important component of the preoperative assessment. Appropriate expectations should be set, as degrees of discomfort can be expected and will vary on an individual basis and depending on the treatment performed. For example, ablative devices can be expected to have greater downtime than their nonablative counterparts. Various topical anesthetics are used to reduce pain and discomfort for laser resurfacing procedures. Topical anesthesia should be applied 45 to 60 minutes prior to the procedure. If patients are particularly anxious, a short-acting oral benzodiazepine may be appropriate. Because of their muscle relaxing action, benzodiazepines are contraindicated in people with myasthenia gravis, sleep apnea, bronchitis, and COPD. Alternatively, nitrous oxide is a safe and effective analgesic that can be used during the procedure to improve treatment pain perception.
Operational safety is a critical component of the procedure, including fire reduction and eye safety. Flammability risk is reduced by minimizing exposure to alcohol cleansed skin, and avoiding dry gauze or other paper products with ablative lasers ( The author HK, encountered an incident in which the exam table paper caught fire while utilizing the CO 2 laser ). Free-flowing oxygen, such as from a nasal cannula, should be removed, or the outflow should otherwise be protected from the applicator. Specific eyewear related to the laser wavelength is critical for everyone in the room at the time of the procedure. For patients, metal eye shields, including intraocular shields when appropriate, are preferred for maximal protection. This is especially important for resurfacing near or around the eye. Tetracaine anesthetic drops, Aquaphor and/or Tobradex (tobramycin/dexamethasone) ophthalmic ointment are used for shield placement, comfort, and prevention of corneal abrasion. Plastic shields can be used with energy-based devices.
Inhalation of laser-treated skin plumes is an occupational hazard. , Long-term effects can be mitigated by mechanical evacuation (e.g., smoke evacuators), appropriate treatment distance, and by wearing masks (N95). It is imperative to have a smoke evacuator installed in each room. Author HK owns Bovie Smoke Shark II, Bovie Smoke Shark III, and the Buffalo PlumeSafe Turbo Smoke Evacuator and finds the latter to be superior for laser resurfacing . ,
Fractional nonablative resurfacing (see  )
)
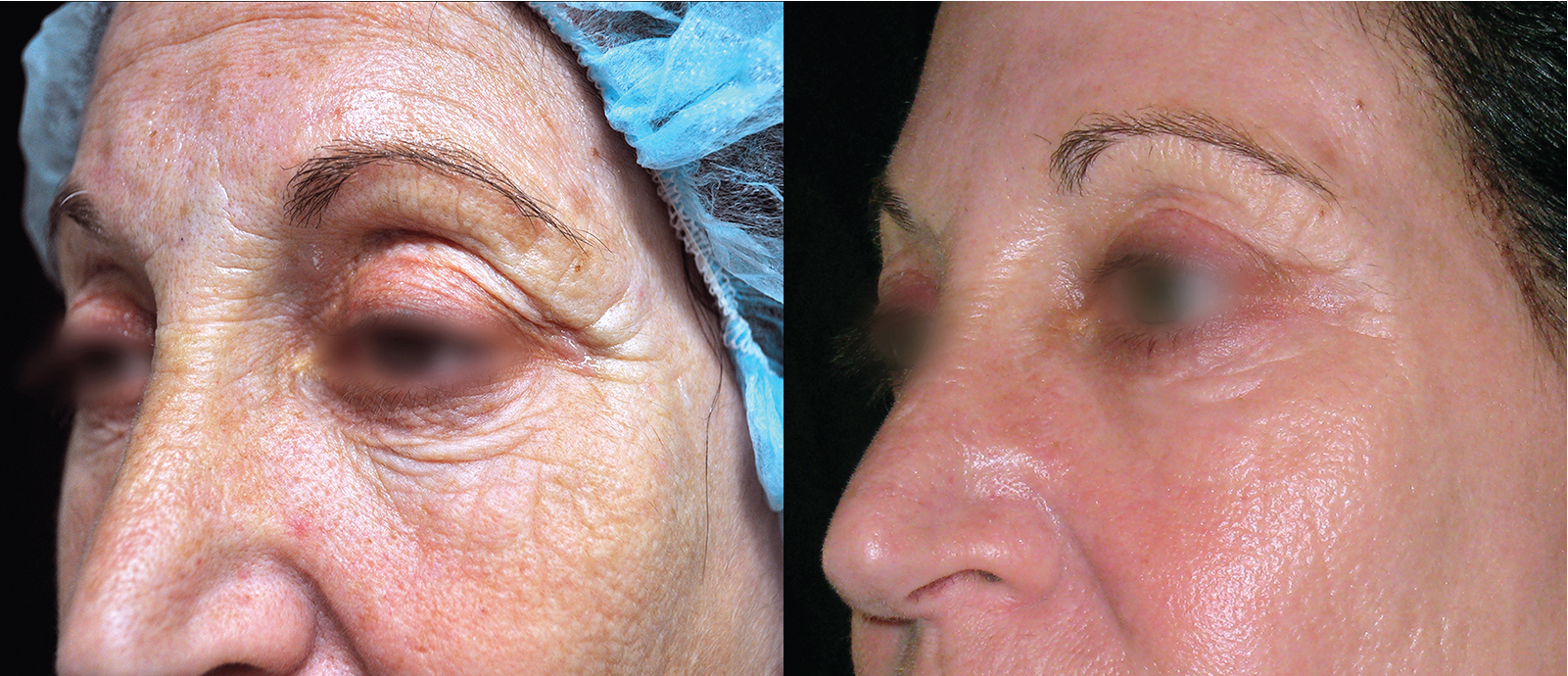
Fractional nonablative lasers are the primary devices used in laser resurfacing today. They offer excellent results with minimal downtime and complications. The first fractional devices, introduced by Manstein et al. in 2004, were nonablative. As with any procedure, proper patient selection is key: the best candidates have mild to moderate photodamage, dyschromia, minimal background tan, and realistic expectations ( Fig. 11.1 ).

Available nonablative fractional devices have wavelengths ranging from 1320 to 1927 nm (see ). In contrast to their ablative counterparts, nonablative fractional lasers spare the stratum corneum from destruction. Examples of wavelengths used for fractional nonablative resurfacing include 1320 nm Nd:YAG, 1410 nm erbium fiber laser, 1440 nm Nd:YAG, 1440 nm diode, 1450 nm diode, 1540 nm erbium:glass laser, 1550 nm erbium laser, 1927 nm thulium laser, 1927 nm diode laser, and intense pulse light source (515 to 1200 nm). Devices can be used to treat scarring, rhytides, laxity, textural changes, striae distensae, prominent facial pores, dyspigmentation, and sebaceous hyperplasia. These devices target water as their chromophore and are safer to use in Fitzpatrick skin types III to VI. Nonetheless, pushing the limits beyond safe clinical endpoints for enhanced results, increases the risk of more temporary (pain, edema, and erythema) and permanent side effects (scarring, dyspigmentation). These risks are more pronounced amongst skin of color patients and in patients with tanned background skin, highlighting the importance of periprocedural photoprotection and meticulous patient selection. Side effects can be minimized by decreasing treatment density, decreasing the number of passes per treatment, increasing cooling between passes, and increasing intervals between treatments. All devices include epidermal cooling as part of the procedure in the form of cryogen sprays or cooling hand pieces to ensure preservation of the epidermis during treatment. No form of cooling has been demonstrated to be superior to another.
Fractional ablative resurfacing (see  )
)
Fractional ablative lasers were developed due to inherent risks and prolonged downtime that may persist with fully ablative continuous devices. Fractional devices cause columns of thermal injury, known as microthermal zones (MTZs), that are equally interspersed between normal, untreated skin. The amount of intact epidermis can be altered depending on the laser treatment settings. The side-effect profile is minimal compared with fully ablative devices, while significant clinical efficacy is retained. Furthermore, devices may be used on low-follicle-count areas such as the chest, back, and arms/legs. It is advisable to reduce the energy by 20% when treating the neck, lateral cheek and the preauricular area as these locations are prone to development of hypertrophic scars. Similarly, it is advisable to lower the energy by 30%-40% when treating locations of the body below the neck . The author HK rarely uses ablative lasers below the neck.
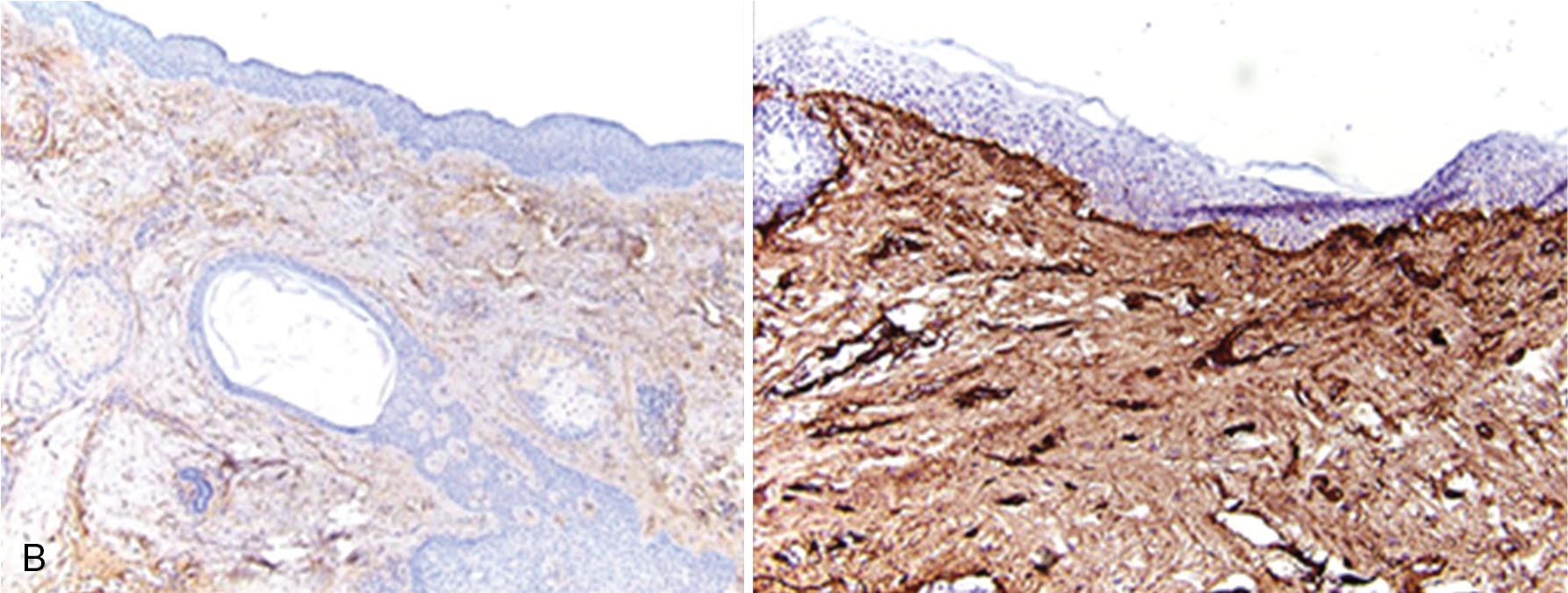
Fractional ablative devices include the 10,600 nm fractional CO 2 laser, 2940 nm fractional Er:YAG, and 2790 nm YSGG laser. Histologically, MTZ zones are surrounded by eschar and thermal coagulation to depths of up to 1.5 mm. Epithelialization is achieved in a short time frame of only 2 days, which is much lower than their unfractionated counterparts ( Figs. 11.2 and 11.3 ). Fractional ablative devices have demonstrated efficacy in treating scars, rhytides, photodamage, dermatochalasis, solar elastosis, lentigines, and even repigmentation of hypopigmented scars secondary to treatment with fully ablative devices.
For all ablative procedures (fully and fractionated ablative), antibacterial and antiviral prophylaxis should be considered in at risk patients. It is also advisable to start a skin care regimen a few weeks prior to the procedure to enhance recovery and speed up the resolution of postoperative erythema (please refer to Dr. Khorasani’s pre and post-operative instructions in the appendix). Topical numbing or nerve blocks can be offered to maximize comfort. The fractional device protocol varies based on the specific device. An over simplified version of treatment is to perform multiple passes, in a cosmetic subunit, that results in the desired endpoint of edema, pinpoint bleeding, or crusting. Highest settings are used around the mouth, nose and glabella (T-zone), the energy is then reduced by 10% around the eyelid and an additional 10% reduction when treating the lateral cheek.
Immediately post-procedure, an emollient is applied, usually plain petrolatum. In order to reduce bruising and edema, ice packs are applied to the treatment area. Crusting may resolve over many days, and bland emollients are used to reduce the edematous appearance and promote wound healing. Patients are instructed to perform vinegar/water solution soaks. This solution is used to promote healing, exfoliation, and avoid infection. All patients should follow the above postoperative instructions in addition to strict photoprotection.

Ablative resurfacing
Dermatologic use of lasers for resurfacing started in the 1980s with ablative CO 2 lasers at wavelengths of 10,600 nm, with a target chromophore of water. These devices worked by heating the tissue, causing continuous ablation to the entire epidermis and superficial dermis, creating a dermal wound healing response with new collagen formation. The desired photorejuvenation was noted after the wound healing process and re-epithelialization were complete, which took weeks and months in some cases. Skin tightening is also noted through heat-induced collagen shrinkage and neocollagenesis. The ablative 2940 nm Er:YAG laser was later developed also targeting water as its chromophore. Fully ablative devices are very effective in treating dyspigmentation, vascular changes, rhytides, elastosis, laxity, and scars. However, these lasers frequently have prolonged recovery times and complications that are best avoided. Complications include scarring, prolonged erythema delayed-onset hypopigmentation, hyperpigmentation, acneiform eruptions, eczematous dermatitis, and infections of viral, bacterial, or fungal origin. Extreme caution should be exercised in treatment of the neck, chest, and hands because they have fewer follicular bulb-derived stem cells. These reservoirs provide re-epithelialization and therefore areas with fewer follicles are at higher risk of complications. Caution should be taken when treating skin of color as risk of post inflammatory hyperpigmentation is increased.
Fractional picosecond devices
Picosecond lasers, designed to target pigmentation combined with a “fractional” handpiece (diffractive lens array, DLA; holographic beam splitter), have been successfully employed in skin resurfacing and tightening. They represent the latest addition to our armamentarium of resurfacing methods. Fractional picosecond devices that have been studied for scarring, texture, and tightening include 755 nm alexandrite picosecond laser with DLA (see Fig. 11.4 ) and 532 nm/1064 nm picosecond laser with a holographic beam splitter. Devices demonstrate significant improvement in dyspigmentation, rhytides, texture, tightening, and acne scarring, including the rolling, boxcar, and ice pick subtypes. This combination has allowed for safe and effective treatment of all skin phototypes and permits off the face treatment such as the neck and extremities.
Energy delivered by picosecond devices results in focal injury limited to vacuoles within the stratum spinosum and sparing other areas; this is in stark contrast to the injury pattern seen in fractional devices, which includes the epidermis and dermis. Picosecond energy-induced areas of laser-induced optical breakdown (LIOB) are likely due to the absorption of picosecond light by melanin, resulting in the local formation of plasma. LIOB possibly results in direct stimulation of epidermal repair, resulting in the formation of mucin, collagen, and elastic scaffolding. , , These histologic changes correlate with the clinical improvement noted with these devices in acne scarring, rhytides, dyspigmentation, texture, and photoaging.

Most patients tolerate fractional picosecond laser resurfacing without adverse effects. Pain tends to be minimal, and there is a transient duration of edema and erythema that subsides within hours. Patients can return to regular activities, with minimal interruptions, on the same day if desired. Cooling gel or ice packs may be used to minimize redness and swelling. Sunblock use must be emphasized to prevent treatment-associated dyspigmentation. Blistering and crusting should not occur unless the epidermis is unexpectedly damaged. Postoperative scarring is rare but can occur in the setting of postoperative infection or improper device settings. We recommend utilizing gentle cleansers and emollients immediately post procedure. Similar to other low energy devices, such as non-ablative fractional lasers, this laser often has to be repeated 4-6 times every 4 weeks for optimal efficacy. This interval is generally prolonged when treating areas outside of the face and for individuals of skin of color.
Ablative and nonablative fractional laser resurfacing modalities can be used to achieve skin resurfacing, rejuvenation, and tightening. Results and downtime vary.
Laser and device settings should never be akin to a cookbook. Instead of using established clinical endpoints, you can provide safe and effective patient outcomes.
Energy-based devices
Radiofrequency and microneedling (see  )
)
A push for improved results, greater skin tightening, and minimal downtime has led to the development of radiofrequency and ultrasound resurfacing devices. They are U.S. Food and Drug Administration (FDA)-approved for rhytides around the eyes, on the face, neck, and chest. FDA approval has also been granted for lifting of the neck, chin, décolleté, and brows. Dermal heating-induced collagen remodeling with energy-based devices results in improved skin texture, wrinkle reduction, collagen production, and laxity.
Radio frequency (RF) devices deliver energy to the dermis, and the resultant resistance causes bulk heating in the desired layer that leads to tightening. Early devices used noninvasive monopolar radiofrequency to create a homogeneous field of heating in the dermis and subcutaneous tissue while simultaneously cooling the epidermis. Clinical efficacy studies on radiofrequency devices demonstrated skin tightening around the forehead, temple, eyes, cheeks, jawline, abdomen, and thighs. Treatments are well tolerated, and the most common side effects are edema and erythema, which typically subside within days to weeks. If the technique is performed improperly, without adequate epidermal cooling, burns and post-inflammatory pigment alteration can occur.
Bipolar radiofrequency devices, with insulated or noninsulated microneedles, deliver energy to the dermis while sparing the overlying epidermis. However, the physical act of microneedle insertion can elicit erythema and dyspigmentation.
Skin tightening energy devices can provide remarkable results, but as with laser procedures, patient selection is important. Ideal candidates are younger, with mild to moderate laxity and mild amounts of facial adipose tissue. Optimal results are achieved, within reason, when treatment is done at higher fluences, with greater surface area, amongst younger patients. It is generally not recommended to use RF devices on severely lax skin due to the limitations of the device. All skin types can be safely and effectively treated as the appropriate use of these devices results in dermal placement of heat. There are only a few contraindications, including patients who are pregnant or have an implanted electrical device (i.e., pacemakers, or defibrillators).
RF skin tightening evaluation includes analyzing the patient’s physical features to identify areas that may benefit from treatment. Patients should be asked about a history of poor wound healing, smoking status, and the presence of a collagen disorder. All of these aforementioned factors render patients poor candidates due to impaired collagenesis after treatment. Patients with minimal facial fat should be cautious if proceeding with treatment, as tightening will likely result in an even more aged appearance. Another factor, noted anecdotally by editor EL, is the reduction of fat or uneven hollowing in certain areas after repeated treatments (it can happen as early as following the second RF session), which he believes is dependent on the depth of heat penetration of the microneedles used to deliver the RF.
Device settings can be calibrated to the desired clinical endpoint and the patient’s comfort. Before the procedure, a topical anesthetic should be applied to maximize patient comfort. Decreasing device settings such as: energy, density, and, treatment time will increase patient comfort, at the expense of requiring more treatments. Energy is delivered at depths ranging from 0.5 to 3.5 mm in the head and neck region and 2 to 7 mm in the body region, depending on the area treated and patient comfort, sparing the epidermis. Multiple areas, including the face and body (such as abdomen and buttocks), can be treated. Treatment is then performed to a clinical endpoint of pinpoint bleeding.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


