Introduction
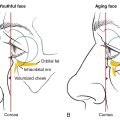
As patients age, ultraviolet (UV) exposure accumulates, and gravity wreaks havoc. Sagging and a wrinkled neck is a common byproduct of this prolonged exposure and causes a great deal of physical and emotional distress to patients. The neck is often an area of concern as the skin is naturally very thin, causing a tendency to sag and wrinkle. Patients are often bothered by dyschromia, fine wrinkling, submental fullness, excessive skin, platysmal banding, jowling, and the ptotic salivary glands.
When discussing neck rejuvenation, it is important to highlight the characteristics of an ideal neck. A youthful neck has: a homogenous and smooth texture without horizontal or vertical lines, a cervicomental angle between 105 and 120 degrees, and a defined jawline.
A neck lift is one of the main procedures done to restore a youthful neck. In the author’s clinical practice, the neck lift is a common cosmetic procedure that does not require general anesthesia, extensive post-operative care, or significant downtime. Oftentimes, patients seek cosmetic surgery for both their face and neck. In these instances, the author will frequently discuss the benefit of combining a fractional carbon dioxide (CO 2 ) laser with the neck lift to enhance cosmetic outcomes ( Figs. 8.1 and 8.2 ). Fractional CO 2 laser resurfacing combined with a neck lift replaces the need for a full facelift in most cases. The CO 2 laser has the ability to tighten the jowls and lower face, working synergistically with the tightening that comes with the neck lift. Patients always want to look natural, and these two procedures ensure that they will.


The purposes of this chapter are to outline the preoperative, perioperative, and postoperative neck lift procedure and to detail the benefits of combining noninvasive and invasive surgical procedures, specifically full-face CO 2 with neck lift. This chapter will also describe how to achieve facial and neck rejuvenation in a safe, effective, and time efficient manner, discussing potential complications, emphasizing that with the appropriate surgical techniques, complications are rare and nearly nonexistent.
Modified surgical neck lift
In this chapter, the authors preferred method is discussed. For traditional corset platysmaplasty, please refer to Chapter 7 .
Discussion prior to the procedure : Includes the limitation of neck tightening behind the ear, post-operative potential bruising and swelling, and the importance of wearing the pressure garment for 1 week 24/7 and then only nightly for 1 month.
Pre-operative medications : Antibiotics starting 1 day prior to the neck lift, continuing for a total of 5-7 days. Author EL uses a perioperative antibiotic given 1 hour prior to the surgery and for a total of 7 days. The antibiotic of choice varies between Doxycycline 100 mg PO BID or Cefdinir 300 mg PO BID for 7 days.
Intra-operative medications : Ativan sublingual and Demerol 25 to 75 mg/Vistaril 25 to 50 mg IM.
Vistaril (Hydroxyzine HCl) reduces salivary secretion, has antiemetic properties, and enhances the effects of Demerol (meperidine HCl). When administered together, Vistaril and Demerol become more effective in anxiety relief and pain management without increasing the risk of respiratory depression caused by Demerol.
Skin Preparation : Hibiclens of the entire neck, ear, and post-auricular area.
To prevent potential ototoxicity associated with prolonged contact of Hibiclens (chlorhexidine) with the inner ear, it is important to take precautions. One recommended method, as suggested by Author EL, is to use sterile cotton balls to plug the ear canal during the procedure. This not only reduces the risk of autotoxicity but also helps prevent the uncomfortable sensation of a blocked or “underwater” feeling that can occur when blood enters the ear canal and dries. Remember to remove the ear plugs once the surgery is completed.
Local anesthesia : Local anesthesia is used to numb the post-auricular area. This allows for diffuse injection of 500 mL of tumescent anesthesia into the entire neck, starting from the anesthetized post auricular region. It is imperative to completely anesthetize the post-auricular hairline, as this is the location of incision and dissection. Additional nerve blocks to the superior orbital, infraorbital, and mental nerves are placed, followed by tumescent anesthesia to the face as well. Anesthetizing pre-auricularly is done if the patient is undergoing full face CO 2 laser resurfacing as well as a neck lift.
Sutures selection : 3-0 Vicryl for plication. 3-0 Vicryl for flap to skin approximation and decreasing tension across the wound. 5-0 gut or fast absorbing gut for the epidermal closure.
Instruments needed : Scalpel handle, Adson forceps without teeth, skin hooks, tenotomy scissors, larger facelift scissors and Webster needle holder. Birther Hyfercator for hemostasis (although it is rarely used with good tumescent anesthesia) ( Fig. 8.3 ).

Incisions : Start at the inferior earlobe with a Burow’s triangle below the earlobe. The incision is placed near the post-auricular sulcus, about 3 mm on the ear/cartilage side of the post-auricular sulcus, close to where the hair line meets the ear. The incision is best placed below where the hairline is close to the ear but not too low where the incision could be visible. Lower post-auricular incision may allow for more skin removal because of a more vascular flap without a small corner where the hairline meets the ear. The incision is carried about 2 mm behind the post-auricular hairline with a bevel so that hair grows over the incision scar. The beveled hairline incision is placed down across from the lower ear or earlobe.
Dissection : A small tenotomy scissor is used to carefully dissect the post-auricular flap from the adherent fascia and away from the incision. After the adherent fascia is separated from the adherent flap, a larger facelift scissor can be used to separate the lower neck from the underlying tissue. The neck is thus completely released to allow for maximum skin excision at the incision lines. Rarely hemostasis will need to be achieved with a Birther Hyfrecator.
Plication : Adson forceps allows one to determine where 3-0 plication sutures are used to tighten the platysma muscle. The bites of plication tightening sutures over the platysma muscle does not need to be large but may average to about 1 inch. The direction of platysma pull is upward and towards the post-auricular area. Tightening along the jowl/mandibular line may be necessary for those with jowls (  ).
).
Flap/skin removal : A skin hook is used to pull the flap skin upward to the most superior part of the dissected skin postauricularly. A 3-0 Vicryl suture is placed to secure the flap in a position that overrides the site of incision at the post-auricular hairline. Two 3-0 Vicryl sutures are used to secure the flap under a maximum amount of tension. The dog ear inferior to the ear lobe is then excised and the skin is finessed so that the ear lobe could be set down without tension and look natural. For those patients with a loose hanging ear lobe, this will require for part of the ear lobe to heal by secondary intention, so the ear lobe is not completely attached resembling the patient’s earlobe before surgery. Once the ear lobe subcutaneous sutures are placed, attention is given to the inferior hairline incision. One Vicryl suture may be placed at this inferior hairline incision to minimize the dog ear at this location. Redundant flap skin becomes obvious with skin hook pulling and the placed subcutaneous sutures. The redundant flap skin is then trimmed as needed. More subcutaneous sutures are initiated at the inferior hairline location working toward the post- auricular ear. Often more redundant flap skin is excised toward the flap corner. Subcutaneous sutures are continued in the post-auricular sulcus and along the entire incision line so as to minimize flap tension.
Skin closure : If there is minimal tension across the wound, running 5-0 gut or 5-0 fast absorbing gut is used to close the epidermal layer of the skin so that the sutures do not have to be removed, creating less anxiety for the patient.
Management of post-operative pain: Patients will complain of pain in the locations where sutures have been placed. Injecting a long-lasting anesthetic, such as bupivacaine or ropivacaine, at these plication suture points at the time of suturing or before the patient goes home through the flap will decrease most postoperative pain. Patients are sent home with extra-strength Tylenol and ice packs. The pain is almost always controlled by these measures. If it’s not, then the author RM will write a script for an opioid pain medication.
Bandaging and wound instructions : Gauze is placed around the incision lines to absorb any overnight oozing. The pressure garment is placed around the neck, head, and ears. The guard and the pressure garment are removed the next morning allowing the patient to shower.
Follow-up visits: The day following the surgery, the author will visit each patient at their home. At this visit, the author changes the bandages and will inject more bupivacaine if the patient complains of pain. The patient will return to the clinic 1 week following the procedure to ensure they are healing appropriately. All patients are given the author’s cell phone number in case there is an emergency.
Discussion
The initial consultation
Cosmetic surgery must be patient-focused and carried out by a surgeon whom patients trust. The initial consultation is an important aspect of doctor-patient relationship and should focus on a series of open-ended questions on features of the neck that are bothersome to patients and to help them reach their aesthetic goals. The initial consultation should also include a discussion of the procedure, possible risks, and realistic outcomes. The patient is told that their saggy neck will be improved, but that the neck may still not be perfect. When the patient looks down, there still may be loose skin because we are tightening behind the ears and not the mid-lateral neck. To demonstrate what they can expect from the neck lift, we often use the patient’s dorsal hand skin to visualize their level of laxity. The author discusses the non-surgical options with each patient, including newly popular techniques such as neuromodulators, fillers, radiofrequency devices, microfocused ultrasound, and suspension sutures. None of these procedures can compare to the level of skin tightening achieved by a surgical neck lift procedure. While some patients are good candidates for these non-surgical interventions, most patients with a sagging neck will require a neck lift to remove the excess skin that appears with age. Some patients will try a series of these noninvasive procedures before undergoing a neck lift.
Some patients with very mild loose skin on the neck and mild jowls can use topical agents. The author RM has a deoxyribonucleic acid (DNA) regeneration serum that he uses for patients, which contains human epidermal growth factor. Another option is to use radiofrequency devices, which heat the skin to 42°C and stimulate collagen production (e.g., pelleve, vivace, endymed, pollagen, intragen). Further, radiofrequency heating under the skin with devices such as thermi-RF or Ultherapy and Sofwave can also treat mild neck laxity. These creams or devices can be good alternatives to prevent or treat mild skin laxity.
When the patient seeking a neck lift appears to have a full neck, one needs to evaluate the degree of excess submental fat, muscle stretch, and skin laxity that are playing a role in the patient’s presentation. If excess fat is present then liposuction should be considered instead of, or as an adjunct to, surgery. To avoid a phenomenon of a “turkey neck” (hanging loose skin) post liposuction procedure, the skin’s natural tightening could be augmented by other modalities such as the laser assisted liposuction (Smart Lipo) or subdermal skin tightening procedure such as FaceTite and ThermiTight. Sometimes it is hard to predict if a liposuction patient or a radio frequency patient will get enough skin tightening with their chosen procedure. Younger patients will get more skin tightening than older ones. A post-menopausal patient or a male in the sixth and seventh decades of life are less likely to get enough skin tightening with these procedures, including liposuction. Lipolytic injections that dissolve fat are not as predictable, are more expensive, rarely achieve skin tightening, require multiple injections, and can cause swelling, bruising and inflammation. Published work by Khorasani et al illustrated that patients with history of Kybella (deoxycholic acid) may have increased post-operative risk after any surgical neck lifting procedure. The adhesions formed by the injections may obscure the surgical planes, which complicates the dissection process. Furthermore, neovascularization seen after Kybella injection may increase the risk of bleeding in the surgical field, necessitating meticulous hemostasis and placement of surgical drains. Finally, there are some heavy neck patients with a weak chin (recessed chin) that benefit from a chin implant in addition to liposuction ( Fig. 8.4 ).