General concept
Facial rejuvenation procedures have increased over the past decade, which has brought increased attention to the anatomy of the face. This renewed focus on understanding facial anatomy with its intrinsic architecture of traversing nerves, vascular supply, and soft tissue arrangement has advanced clinical intervention and continues to provide guidelines for safe practice. While standard anatomical descriptions may provide a basis for understanding facial anatomy, introduction of newer concepts and attention to structures once overlooked has shifted the paradigm to a focus on clinical relevance. An increasing number of new concepts and structures have been directly integrated into current practice and used to support as well as confirm current therapeutic strategies. Thus, anatomy and anatomic research contribute significantly to patient health and can be regarded as one of the fundamental pillars of surgical and non-surgical interventions.
The major concept of layered arrangement of facial structures has progressed most in the last decade and continues to have the greatest influence in the new era of facial rejuvenation. This concept is based on the fact that facial structures are arranged in layers with structures being either incorporated inside a respective layer or being located between specific layers. This novel concept introduced the third dimension into facial treatments and has transformed the way facial anatomy is understood: from two-dimensional to three-dimensional. Understanding and accepting that the face is arranged in layers (comparable to the layers of an onion) provides guidance to any facial procedure because it allows practitioners to locate structures according to their depth, rather than solely based on their neighboring structures.
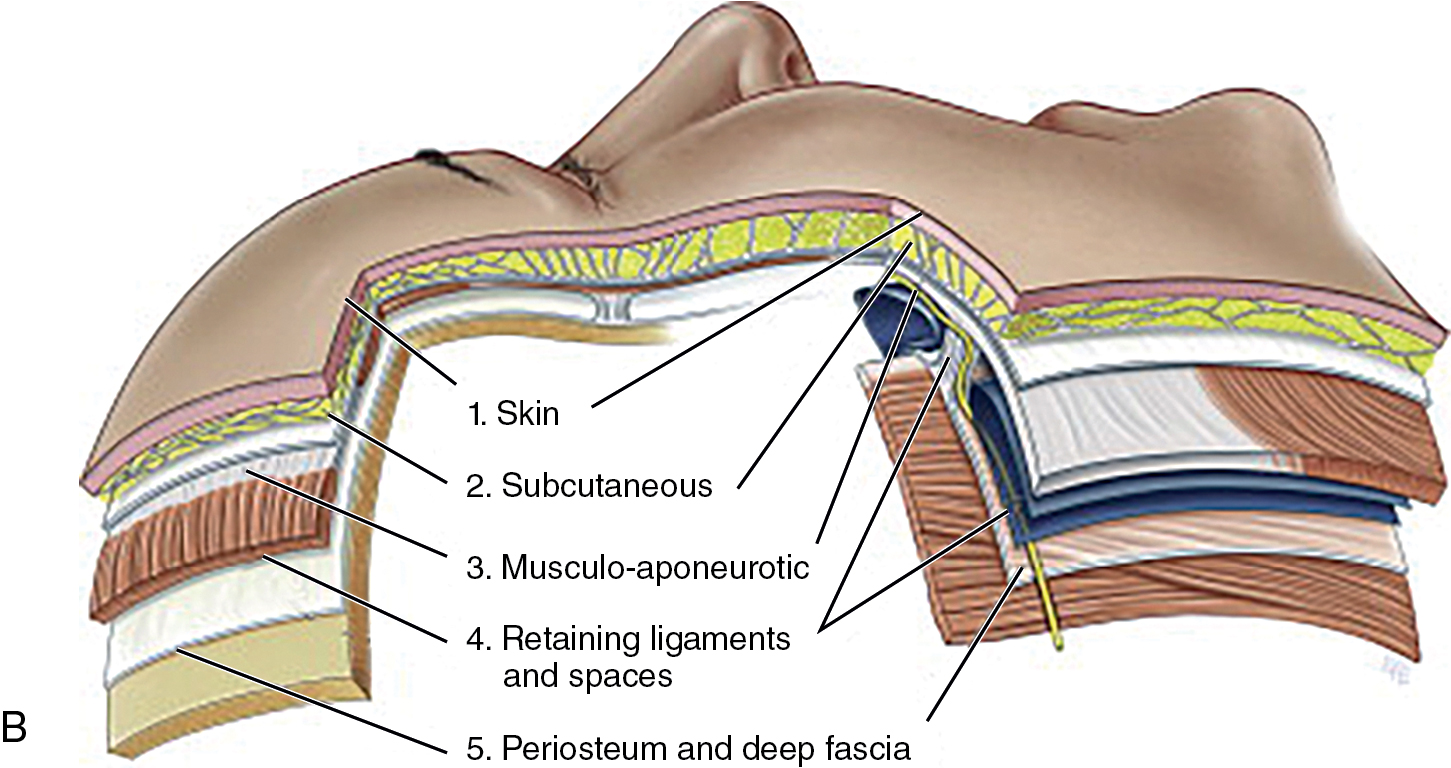
The layers of the face can be identified from superficial to deep: skin (epidermis and dermis), superficial (subdermal or subcutaneous) fat, superficial fascia, deep fat, and deep fascia. This five-layered concept is generally applicable, but there are special sites where this does not apply ( Fig. 1.1 ). For example, in the temple, there are a total of 10 layers, whereas, in the tear trough, there are only three layers. Another important factor to consider is that the superficial and deep fat layers are reduced in thickness with aging and in those undergoing repeated facelifting procedures. Precise knowledge about the areas targeted, the number of layers present, and their respective thickness, will facilitate the information needed to locate anatomical structures and thereby increase patient safety and efficacy of the procedural outcome.
Anatomy relevant for (midfacial) facelift procedures
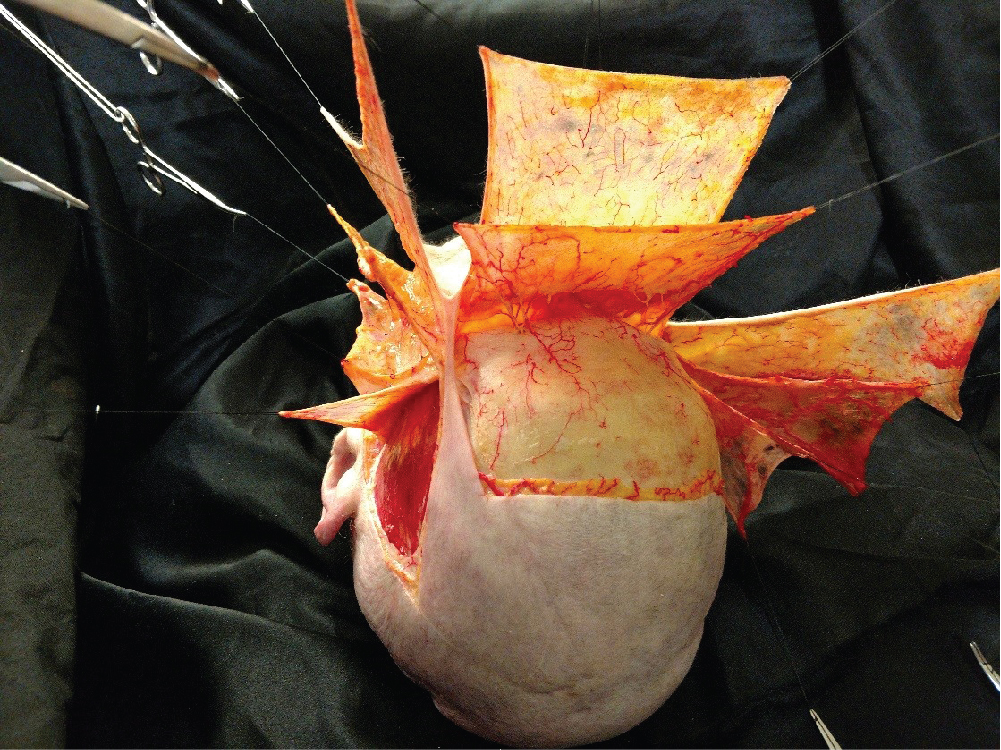
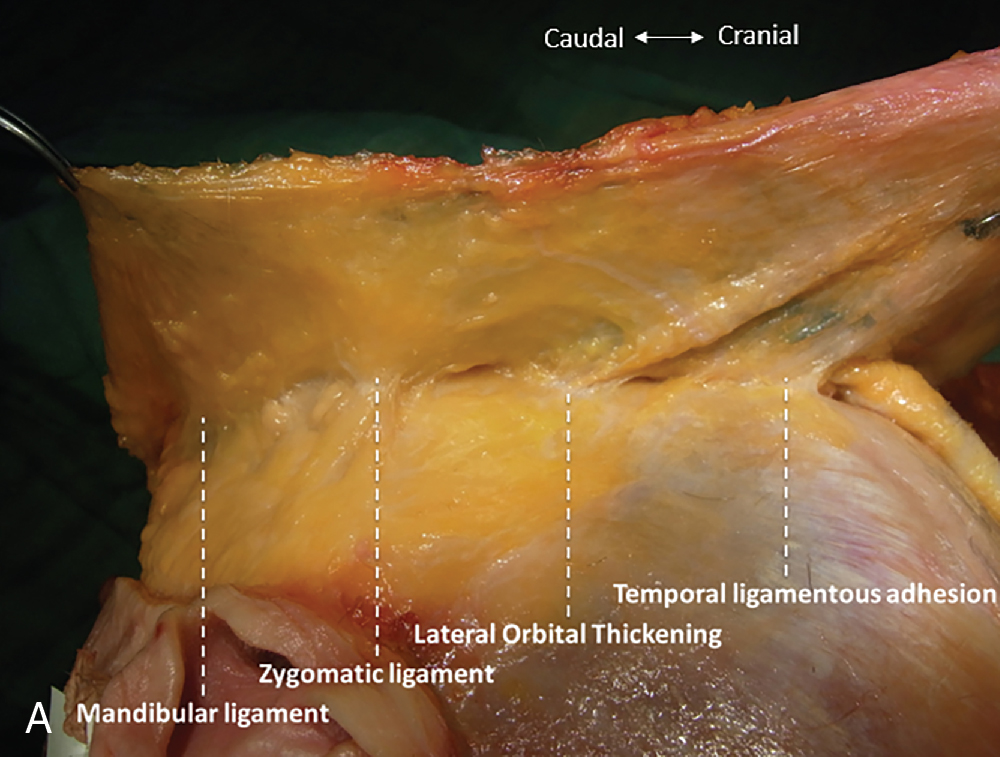
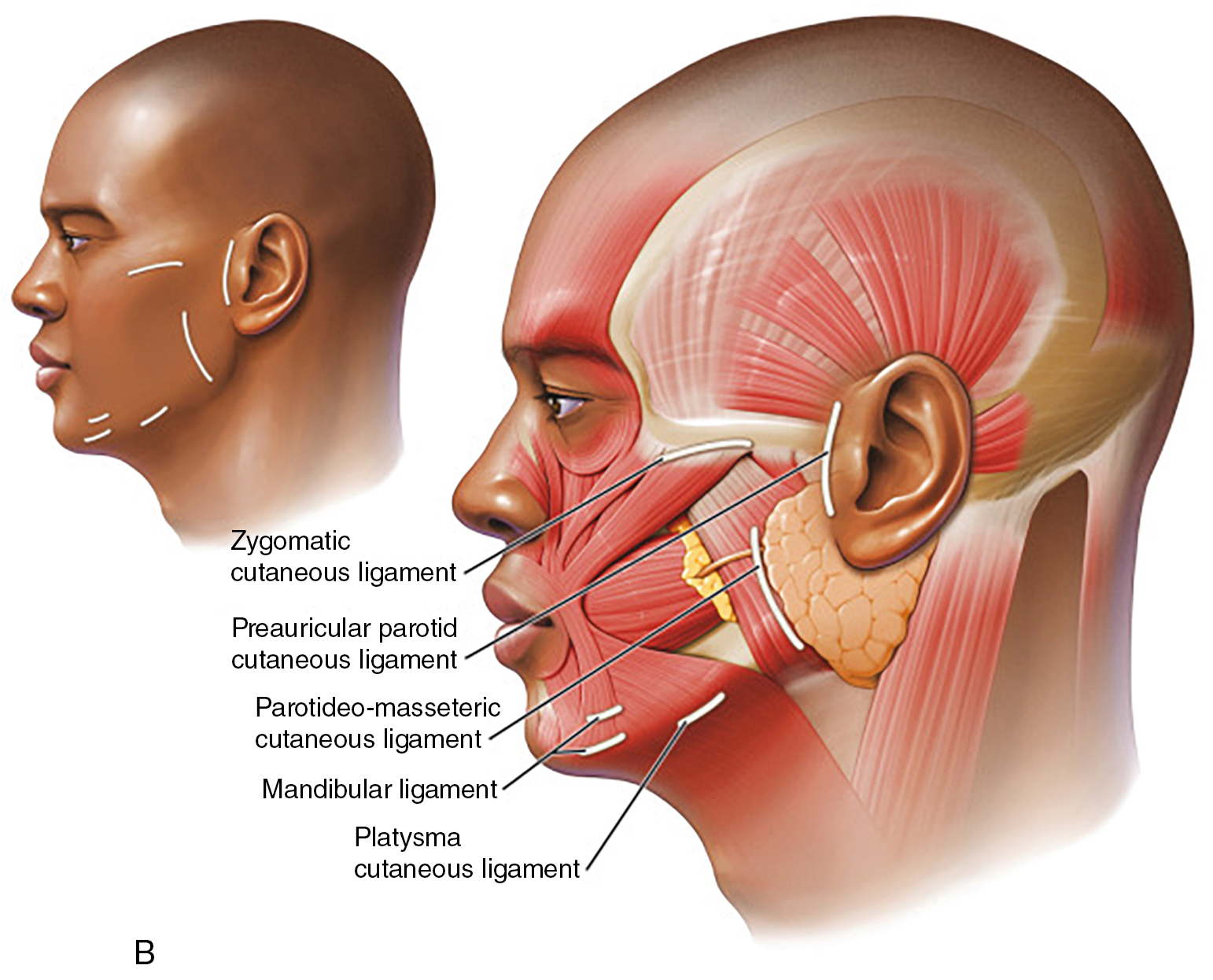
The anatomy of the midface is complex and has to be viewed in the light of two separate areas. These areas are the medial and the lateral midface. The boundary between those two areas is referred to as the line of ligaments (see Fig. 1.2 A). This concept was recently re-discovered when studying facial ligaments. Ligaments are classically defined as a fibrous connective tissue joining two bony structures. This line of ligaments is unique in that it forms a line that connects the bony structures and extends through the overlying soft tissues into the skin, thereby anchoring it and supporting it. The most important facial ligaments are located in an imaginary vertical line starting from the temple (temporal ligamentous adhesion), connecting to the lateral orbital rim (lateral orbital thickening), connecting to the zygomatic arch (zygomatic ligament = McGregor’s patch) and extending until the mandible (mandibular ligament) (see Fig. 1.2A–1.2C ).
These true osteo-cutaneous connections are located along this vertical line and this line separates the medial from the lateral midface. The deep facial fat compartments are located in the medial midface. The lateral midface contains the masseter muscle, the parotid gland and duct, and the buccal fat pad, which is hidden deep, between the buccinator and masseter muscles. This separation explains why most facelifting procedures have their greatest effect when treating the jowls and the labiomandibular sulcus (located in the lateral face) but have limited effects when targeting the nasolabial sulcus (located in the medial midface).
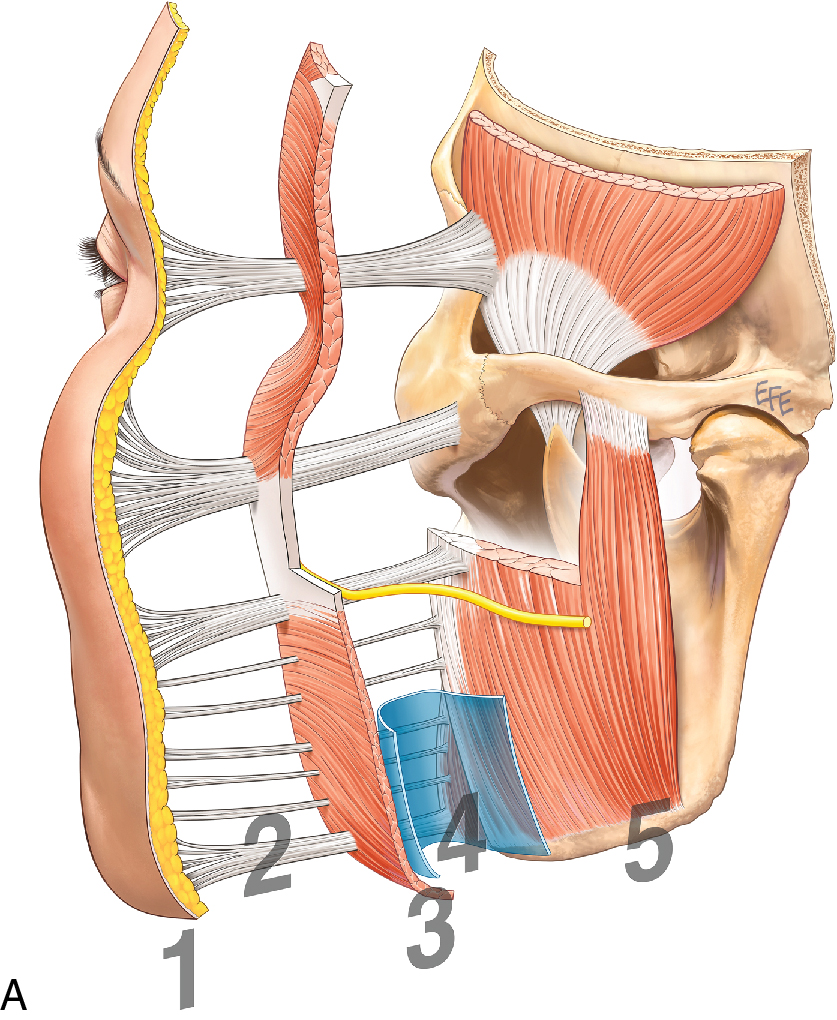
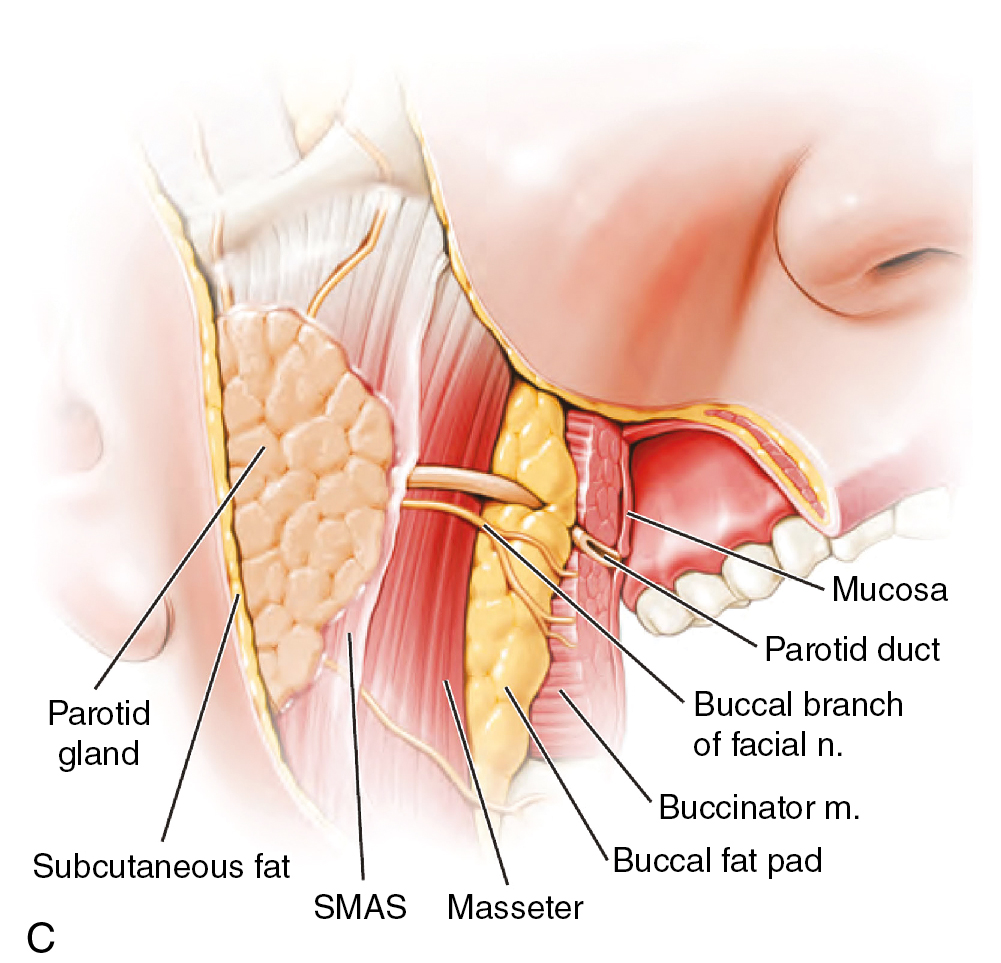
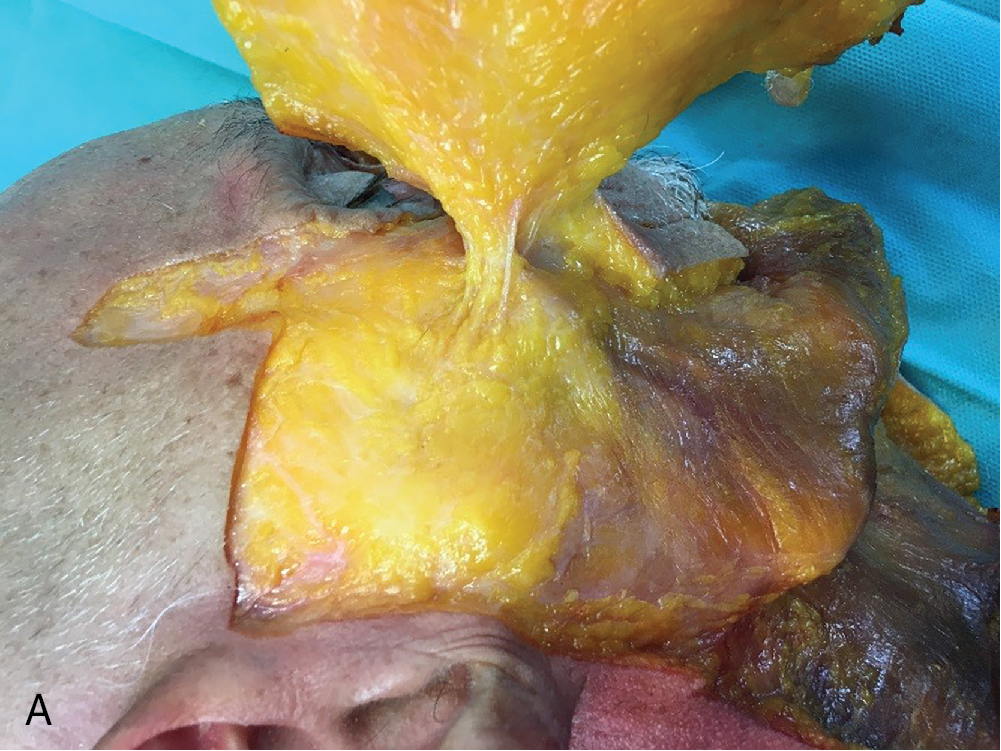
The layers of the lateral midface are as follows: skin, superficial fat, superficial musculo-aponeurotic system (SMAS), deep compartments (pre-masseteric spaces), deep fascia (parotideo-masseteric fascia), masseter muscle, parotid duct, the proper and accessory parotid gland, and buccal fat pad ( Fig. 1.3 A). This layered arrangement changes at the anterior boundary of the masseter muscle, which is still located in the lateral face. Here, the parotideo-masseteric fascia divides into an anterior and a posterior lamina, attaching to the buccinator muscle and a recently identified structure: the facial vein canal (see Fig. 1.3 B). The facial vein canal envelopes the facial/angular vein while traveling from the mandibular crossing to the medial canthus. At the anterior portion of the masseter, the parotid duct pierces the buccinator to drain into the oral cavity (see Fig. 1.3 C).
The location of the parotid duct can be determined by drawing a line from upper vermillion border to tragus and another line crossing it from the lateral canthus. The duct is most susceptible to injury where these 2 lines meet.
The SMAS is a 3D network composed of collagen fibers, fat and connective tissue. The initial name of an “aponeurosis” is correct as this fibrous plate connects the platysma muscle to the orbicularis oculi muscle. Its connection to the auricular muscles, which have become rudimentary in humans (no distinct ear movement is needed anymore), is of less importance here. The SMAS is tightly adherent to the parotid fascia proper and to the parotideo-masseteric fascia overlying the parotid gland proper (not accessory). This is one possible explanation for why sub-SMAS procedures carry the risk of deeper access as the correct plane is difficult to identify. In the lateral midface, the SMAS is more substantial, whereas, in the medial midface, the SMAS is thin and infiltrated by the muscles of facial expression.
Medial to the line of ligaments, most of the facial muscles are incorporated in the SMAS and travel together to their points of insertion (orbicularis oris muscle complex or modiolus) as a musculo-aponeurotic unit. This is why when the facelift undermining is extended medially to these ligaments a common misalignment results causing the orbicularis muscle stretching and the lip becoming thinner.
The five main motor branches of the facial nerve (cranial nerve VII) can be found within the parotid gland, at the separation of the superficial and deep portions of the parotid. When exiting the parotid gland, the facial nerve branches are located deep to the parotideo-masseteric fascia. Sub-SMAS facelifting procedures are safe in this area if they do not penetrate the parotideo-masseteric fascia.
Once the anterior margin of the masseter muscle is reached, the facial nerve branches enter the facial vein canal and run inside its roof, superficial to the facial/angular vein. Here, the facial nerve branches exit the facial vein canal and change planes from deep to more superficial. The change in planes is accompanied by fascial adhesions, which have been previously termed as masseteric ligaments, despite their absent connection to the masseter muscle and lack of criteria in order to be termed a ligament. Sub-SMAS facelifting procedures must be performed with caution when passing the anterior margin of the masseter muscle due to the risk of damaging the facial nerve motor branches (see Fig. 1.4 ).
Since most of the mimetic muscles are situated superficially to the facial nerve plane, they receive their nerve supply along their deeper surfaces. To prevent motor branch injury, dissection should be performed along the superficial surface of a mimetic muscle (i.e., superficial to the platysma in the cheek and neck). Typically, facial nerve branches lie deep to the deep fascia until they reach the muscles they innervate. Once they reach the muscles, they penetrate the deep fascia to innervate them along their deep surfaces. The temporal and cervical branches are exceptions to this rule. In the illustration of Fig. 1.3 A and B see the plane of the nerves in relations to the fascial layers. In Fig. 1.4 , the deep fascia has been removed to demonstrate the depth of nerve branches relative to the innervated muscles. The cervical branch usually penetrates the deep fascia laterally, lying within the plane between superficial and deep fascia, just deep to the platysma, before innervating the platysma medially. Similarly, the temporal branch travels in the plane between superficial and deep fascia after it travels superiorly to the zygomatic arch ( Fig. 1.6 A). It is important to note that the temporal branch is positioned cranial to the ligament, and to reach the ligament, from a facelift incision one must cross its pathway. The author EL approaches this ligament, when needed from the lower blepharoplasty incision to reduce the risk of its inadvertent injury.
Releasing the zygomatic ligament (= McGregor’s patch) ( Fig. 1.5 A) or the mandibular ligament (see Fig. 1.5 B) have been shown to provide enhanced lifting opportunities as greater mobility for the overlying soft tissues can be achieved. Transecting the zygomatic ligament can result in substantial bleeding as the ligamentous branch of the transverse facial artery (a branch of the superficial temporal artery) runs inside the ligament. Releasing the mandibular ligament is controversial due to its long dissecting pathway and due to the increased risk of damaging the marginal mandibular branch of the facial nerve. This nerve runs cranial to the ligament and its pathway has to be crossed if the ligament needs to be reached.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


