Blepharoplasty and brow lift
Patient selection
It is often said that the eyes are the windows to the soul. Surgically “opening these windows,” on appropriate patients, can lead to long-lasting rejuvenation. The eyelid aesthetic unit is very complex and unforgiving, particularly the upper eyelid. The surgeon must distinguish whether it is a ptotic brow that is the sole cause of upper eyelid dermatochalasis, exacerbating it or merely playing a minor role. Failure to assess the brow position and role will lead to a dissatisfied patient since an upper blepharoplasty alone may not meet the patient’s expectations or reduce eyelid “heaviness.” A surgical brow lift, browpexy, or possibly a nonsurgical brow elevation may stabilize the eyebrow (see Chapter 3 ). Similarly, the surgeon needs to assess for lateral hooding which may require extension of the incision on the upper eyelid and or a lateral brow lift. Superior lateral fullness on the upper eyelid could also be caused by a ptotic lacrimal gland that should not be confused with excessive retro-orbicular oculi fat herniation. The former would need to be repaired; the latter would need to be excised.
Patient history for upper eyelid blepharoplasty, lower eyelid blepharoplasty, and brow lift
Medical history is very important and a few specific questions need to be considered. Does the patient have orbital exophthalmos from Graves disease? In patients with Graves disease, blepharoplasty would not be appropriate and may lead to serious complications. In addressing the lower eyelid, will fat removal lead to a tear trough deformity and hollowness? If hollowness is present, fat repositioning procedure may be more appropriate in selected patients (see Chapter 10 ), or potentially fat transfer or correction with injectable fillers. Is a hypertrophic orbicularis oculi creating the lower eyelid bulge as opposed to a fat pad? If that is the case muscle excision needs to be considered and an open transcutaneous approach may be more appropriate as opposed to a transconjunctival approach (see Chapter 5 ). Does the patient have excessive laxity of the tarsal plate? In these patients, a transconjunctival approach with a simultaneous canthopexy or canthoplasty should be considered. Finally, are there fine static rhytides on the lower eyelid that would benefit from laser resurfacing particularly when a skin sparing transconjunctival approach is considered?
In determining a patient’s appropriateness for blepharoplasty and brow lift, the physician must consider both the medical and ophthalmic histories. The past medical history should include a thorough review of prior eye or facial trauma, previous surgeries (eyelid, facial, or vision), postoperative successes or complications of those surgeries, as well as the patient’s expectations for the blepharoplasty or brow lift. It is recommended to delay a blepharoplasty at least 6 months following any refractive surgery (i.e., laser-assisted in situ keratomileusis [LASIK]) in order to allow for the regeneration of the transected corneal nerves responsive for reflex tearing, and therefore decrease the risk of xerophthalmia. It is also recommended to allow a 6-month wash out period for any neuromodulator treatments in order to not alter the anatomy and distort the preoperative physical examination. Authors EL and DS wait 3 months after a neuromodulator is used to allow the brow position to return to its natural position.
When there is a significant participation of the frontalis muscle in the brow elevation, and thus in the lateral upper eyelid lift, author EL advices to inject a neuromodulator two weeks before the planned surgery to eliminate the effect of the frontalis muscle on the natural brow and upper eyelid position in order to best assess the amount of eyelid lift and or brow pexy needed.
Herbal and vitamin supplementation use by patients should be particularly noted. Ginkgo and vitamin E predispose patients to an increased risk of bleeding, while the risk of developing ocular surface disease increases with the use of kava, echinacea, and niacin. Additionally, vitamin A and its derivatives are associated with an increased risk of xerophthalmia and formation for hypertrophic scars. , Another extremely important factor to consider is the patient’s smoking history—it too can lead to exacerbation of dry eyes following the procedure and poor wound healing. , Development of postoperative dry eyes needs to be prevented whenever possible because it carries with it the threat of further ocular damage and increased potential for unfavorable surgical outcomes. Therefore, any pre-existing xerophthalmia should be investigated by a medical ophthalmologist and the baseline dryness ought to be documented.
The effects of cannabidiol (CBD) and tetrahydrocannabinol (THC) use are associated with acute dryness. Whether their use has a negative impact on the postoperative outcomes following a blepharoplasty and/or brow lift are not yet known. Therefore, currently, the authors recommend that patients discontinue the use of both prior to and during the initial healing phase of the surgery (2 weeks before and up to 1 month after).
Patient history also needs to encompass relevant comorbidities. In addition to glaucoma, dry eye disease, and blepharitis, other conditions such as a thyroid disorder, cardiac disease, and rheumatological conditions may all have ophthalmological manifestations. As with most, if not all surgeries, the presence of uncontrolled hypertension, bleeding or clotting disorders, and the use of aspirin or other antiplatelet or anticoagulation agents must be discussed as they are all relative contraindications (see Chapter 14 ).
Lastly, if blepharoplasty or brow lift is being considered for functional abnormality as opposed to aesthetic, additional testing such as corneal topography, visual field, contrast sensitivity, and high-order aberrations (HOAs) needs to be assessed pre- and postoperatively. Furthermore, if both an upper eyelid blepharoplasty and brow lift are being considered, the surgeon should plan a more conservative upper eyelid skin excision in order to ensure the patient will not have difficulty closing their eyes postoperatively, referred to as lagophthalmos.
Physical examination of upper eyelid (see  )
)
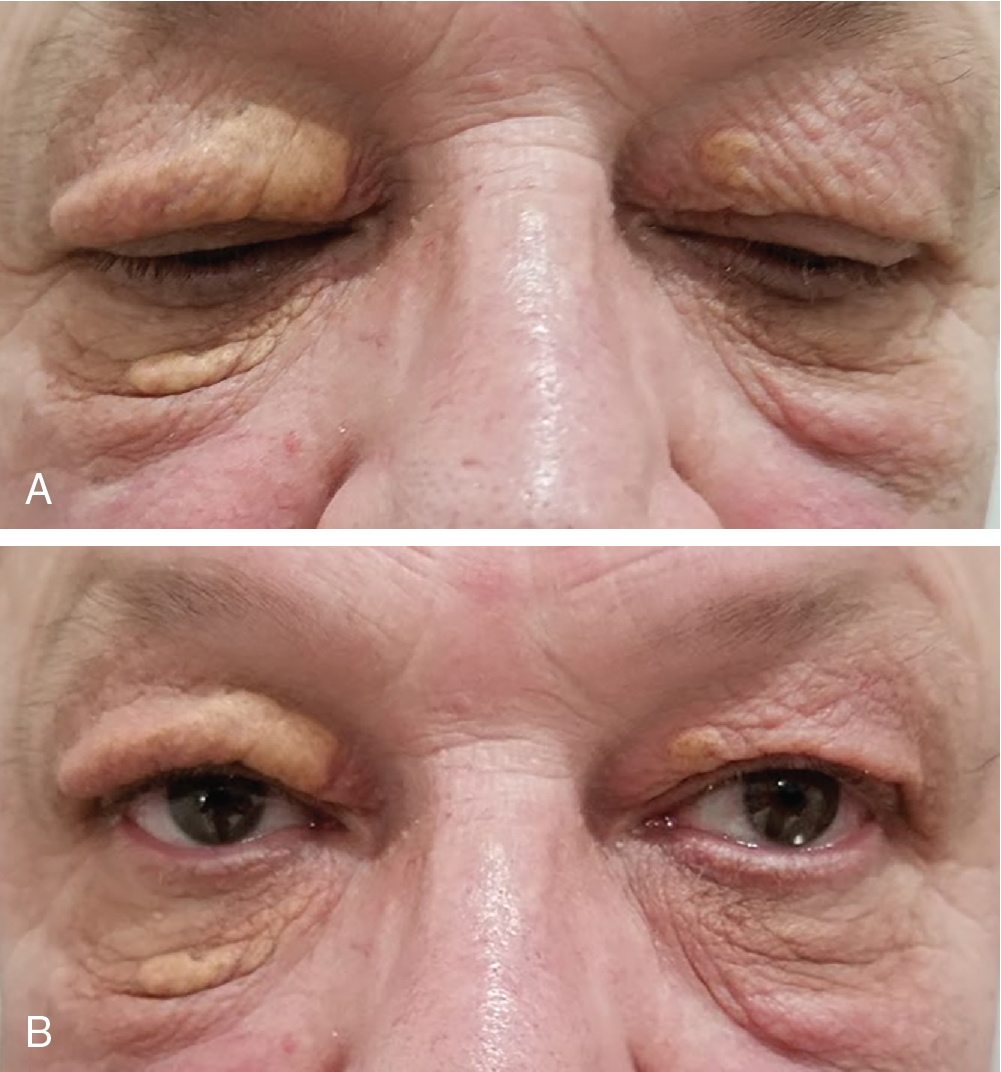
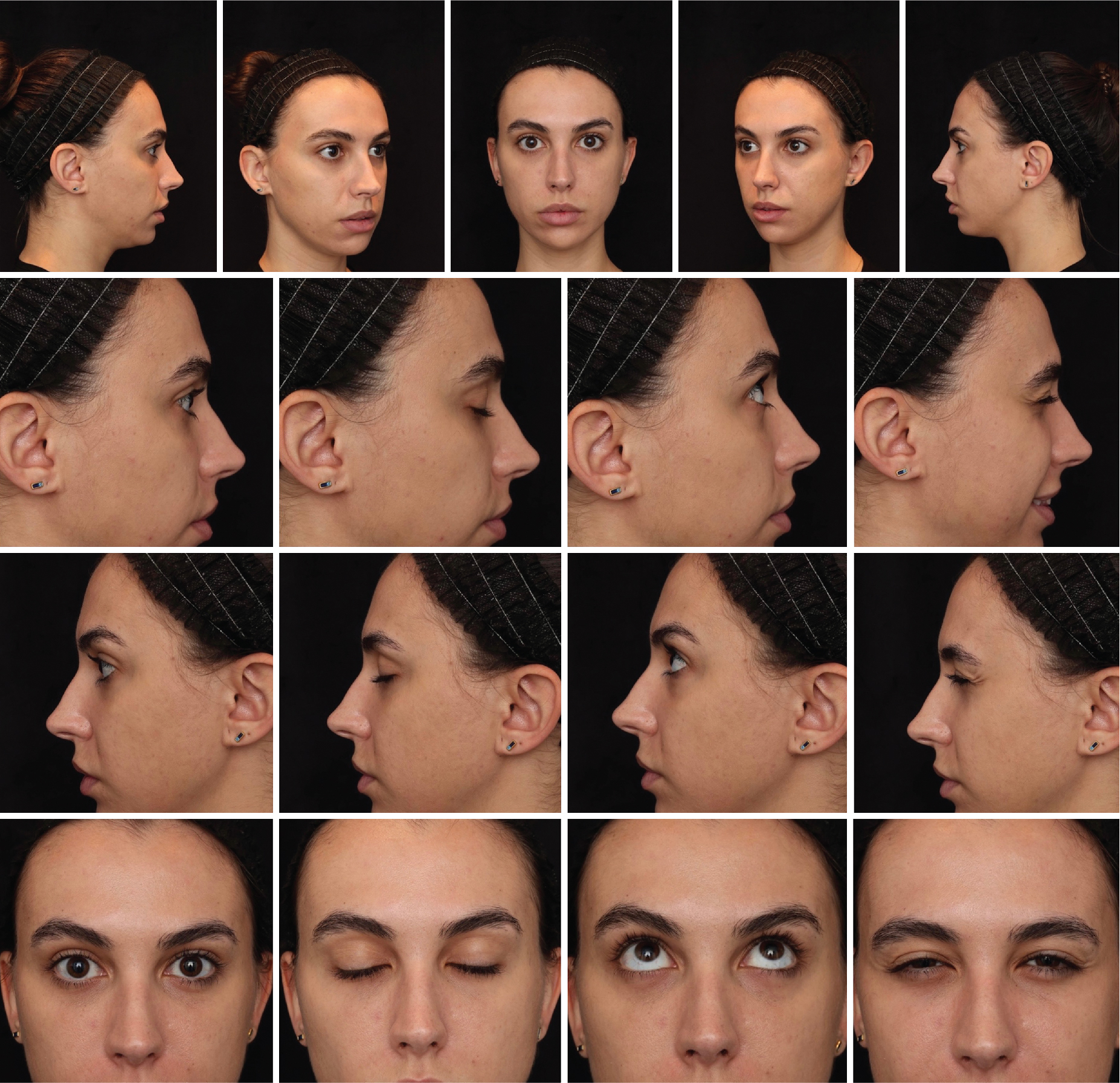
A thorough physical examination of the upper eyelid and brow is imperative prior to performing any upper eyelid blepharoplasty or brow lift. To begin the exam, the physician should place the patient in a 90-degree seated upright position and assess for functional abnormalities (trauma, inflammation, blepharochalasis, dermatochalasis, epiblepharon with lash ptosis, xanthelasma ( Fig. 2.1 ), tumors, amblyopia, strabismus or skin cancers ( Fig. 2.2 ). Vision should be grossly tested and the results compared with a report by an ophthalmologist’s testing of visual acuity. It is important to build a relationship of trust with your referring ophthalmologist. The eyelid skin should be examined for both benign growths such as seborrheic keratoses as well as malignant tumors such as basal cell carcinoma and sebaceous carcinoma. If a suspicious lesion is noted a biopsy must be performed showing benign histology prior to proceeding with an elective cosmetic procedure. Mirrors are a great tool as they assist in both parties identifying the same abnormalities. Both the physician and patient seeing the same problem helps achieve the best outcome and understanding. The old adage “seeing is believing” is quite appropriate here. Preoperative photographs are also part of the armamentarium and allow both patient and the physician to see many abnormalities in a still shot ( Fig. 2.3 ). When taking photos, the authors recommend the following directions: preoperative photos should be taken head-on and at 45-degree and 90-degree angles on both sides of the face, the patient should look upright, down, left, and right. Prior to any of the above surgical procedures, thorough testing of facial nerve function should be performed. The patient should be asked to raise their eyebrows (which results in forehead creases), close their eyes and resist opening by the physician, puff out their cheeks, and then have the patient smile while revealing their teeth. Although taste of the anterior 2⁄3 of the tongue and hyperacusis is a function of the facial nerve as well, it is rarely tested. Palpebral oculogyric reflex, or the Bell phenomenon, is an upward and outward movement of the patient’s globe when they try to close their eyes. This is a natural reflex but becomes more noticeable with a weakened orbicularis oculi muscle. Additionally, the globe position, measured by the distance from the lateral orbital rim to the corneal apex using an exophthalmometer, visual field and visual acuity tests should all be considered.

The brow and the upper eyelid are considered a cosmetic unit. Modification in one will affect the other. For example, following an upper eyelid blepharoplasty for a functional impairment (like dermatochalasis) a patient may sustain a brow ptosis.
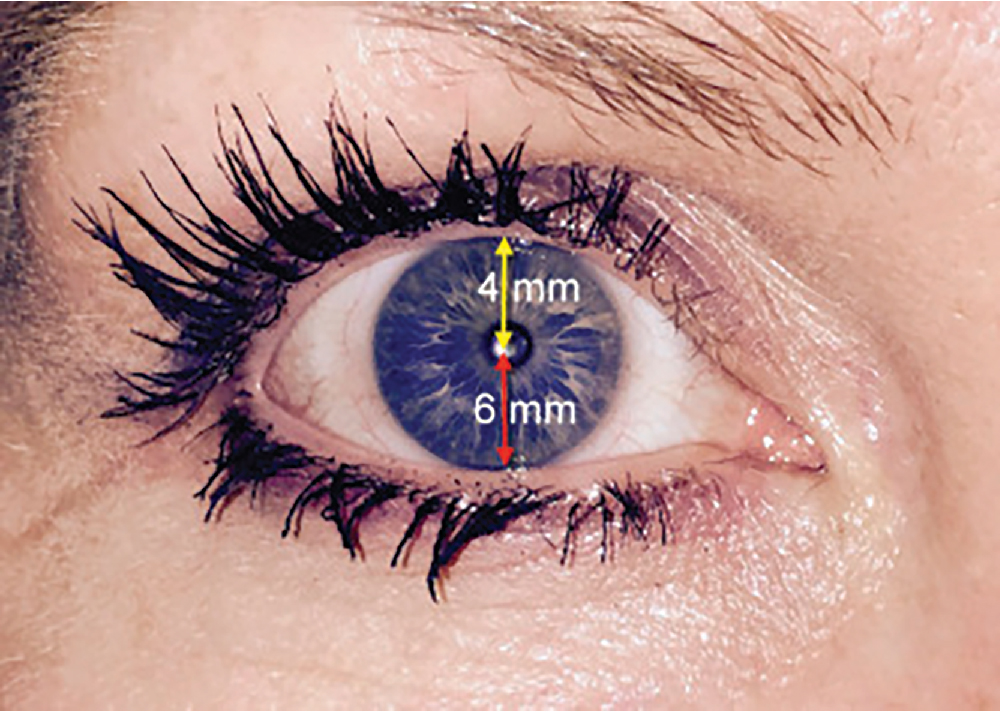
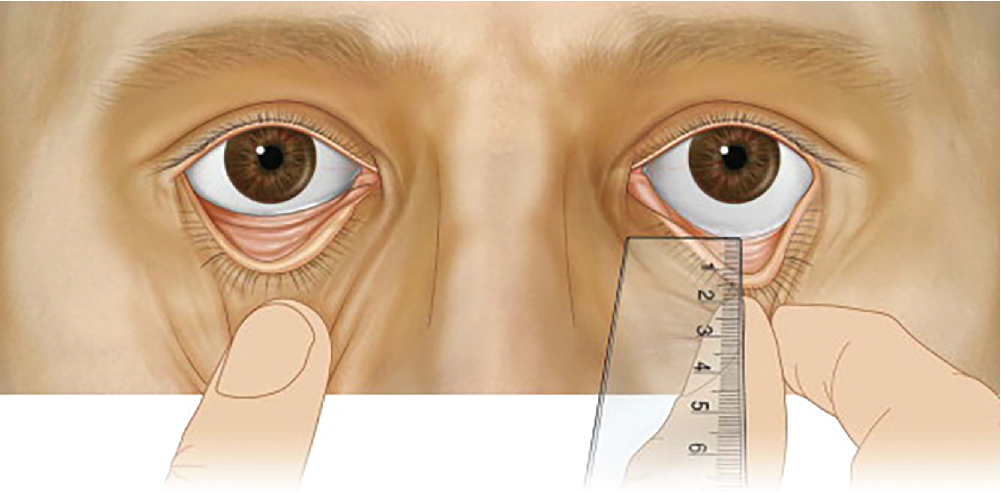
A thorough understanding of facial and eyelid anatomy is imperative. To assess upper eyelid position, the examiner should be eye level with the patient and measure the margin reflex distance-1 (MRD-1). With the patient’s gaze in primary position, the MRD-1 is obtained by measuring the distance, in millimeters, from the corneal light reflex to the central upper eyelid margin. The average MRD-1 varies among ethnicities, with Caucasians having the highest estimated mean of 5.1 mm. The remaining documented means are: African Americans 4.5 mm, Latinos 4.4 mm, and Asians 3.8 mm. MRD-1 is essential for diagnosing blepharoptosis and ptosis of the levator muscle (an abnormal low-lying upper eyelid margin while the eye is in primary gaze), defined by an MRD-1 measurement less than 2.5 mm or the upper lid margin vertically covering greater than 2 mm of the superior limbus. MRD-2 is essential for diagnosing lower lid retraction, which is defined as having an MRD-2 of greater than 6 mm. MRD-2 is obtained by measuring the distance, in millimeters, from the corneal light reflex to the central lower eyelid margin while the patient’s gaze is in primary position ( Fig. 2.4 ). The sum of MRD-1 and MRD-2 is referred to as the palpebral fissure.
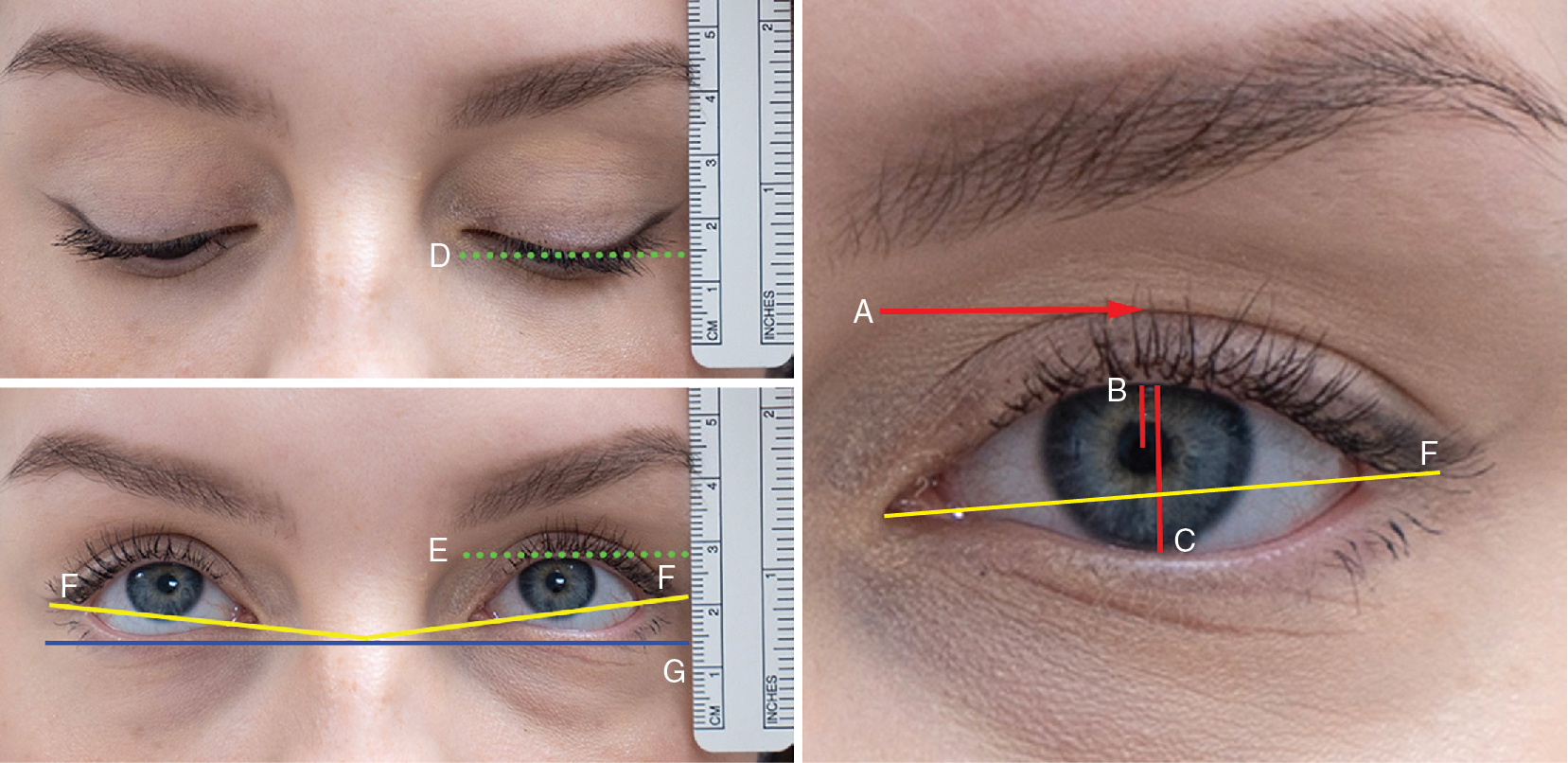
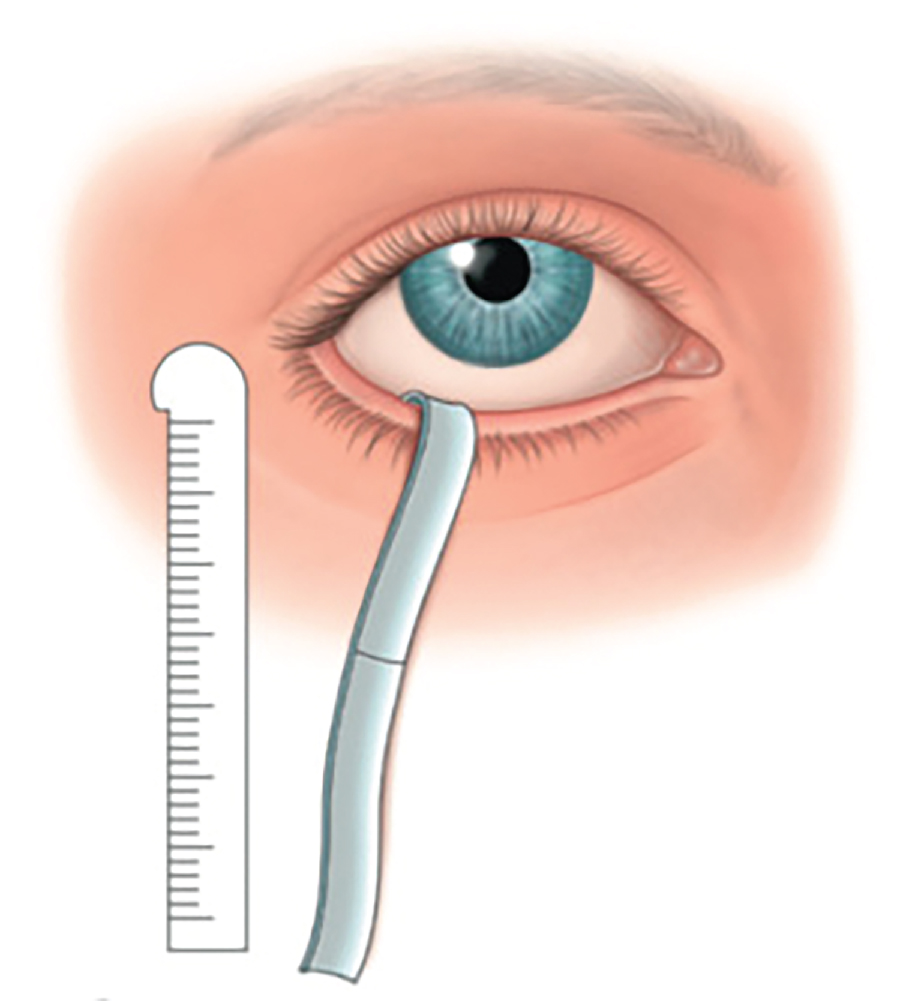
Upper eyelid excursion should be assessed in order to determine if there is a dehiscence of the elevator muscles or aponeurosis. It is measured ( Fig. 2.5 ) by the distance of the upper eyelid margin from a downward to an upward gaze. The normal value is greater than 12 mm. The medial and central fat pads also need to be assessed and graded 0-3 (0–hollowness representing the absence of fat pad; 1, 2 and 3 represent mild, moderate and severe fat pad herniation, respectively) as well as the nature of the lacrimal gland. As discussed earlier, baseline dry eyes should be assessed since most eyelid procedures may temporarily exacerbate this condition. The Schirmer Test, which has two variations ( Fig. 2.6 ), is often used to evaluate tear production. Each test is performed by placing a strip of filter paper to the conjunctival surface of the lower eyelid and measuring the amount of moisture after 5 minutes. In Schirmer I test, an anesthetic is used thereby measuring baseline secretion. Whereas in the Schirmer II test, no anesthetic is used, measuring baseline and reflex secretion. A normal Schirmer’s test reveals a normal wetting range from 15 to 30 mm. When the wetting of the filter paper is less than 10 mm after 5 minutes, this is considered an abnormal Schirmer’s test.
Physical examination of the brow (see  )
)
In women, an arched brow is considered aesthetic as opposed to a horizontal brow shape which is considered more aesthetic in male patients. Traditionally, in women, the brow arches 2 to 3 mm above the superior aspect of the orbital rim in order to provide a more open and youthful aesthetic eye complex. In men, the brow is flatter and generally lies on the orbital rim. To allow proper evaluation of the upper eyelid and brow position, while examining the brow and upper eyelid it is imperative that the patient relax the frontalis muscle. It is well-documented that when one muscle is lagging, others will try to compensate, resulting in hypertrophy of the overused muscle. If the muscle becomes hypertrophied, it can result in a lid or brow ptosis.
Physical examination of lower eyelid (see )
Similar to the upper eyelid and brow, the lower eyelid examination should begin first with the patient seated in a 90-degree upright position. The exam should assess for asymmetry, abnormal anatomy, fat prolapse, excessive skin, rhytids, ectropion, festooning, tear trough deformity, orbital vector, and dermatochalasis. If dermatochalasis is found, the amount of skin that can be safely removed needs to be determined. In order for the surgeon to accurately make this decision, the patient should be instructed to gaze upward with his/her mouth open in order to stretch the skin.
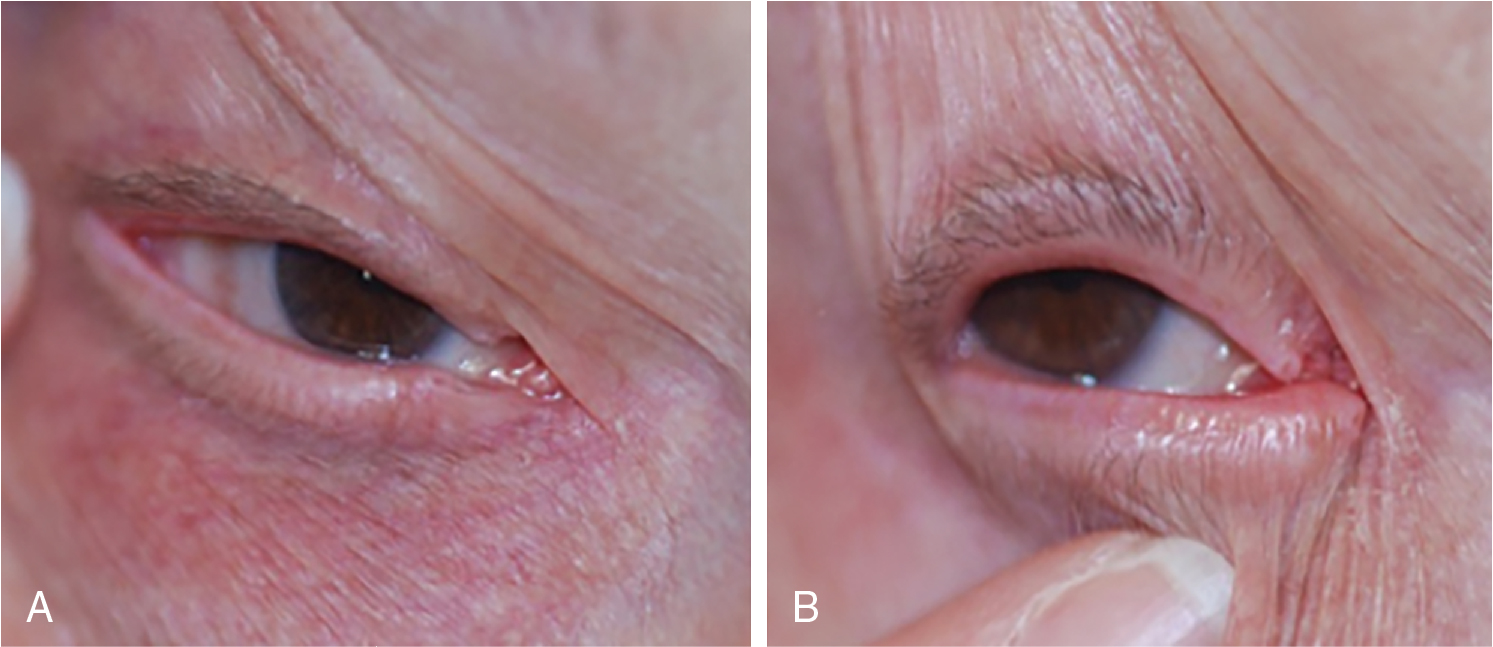
The exam proceeds with the evaluation of eyelid malpositioning (i.e., eyelid tone and tarsal laxity) using the snap-back test and distraction test ( Fig. 2.7 ) discussed in more detail in the upcoming section. Next is the assessment of the medial and lateral canthal tendon laxity ( Fig. 2.8 ) . Medial canthal tendon laxity is evaluated by measuring the excursion of the punctum in relation to the cornea while the lower lid is pulled laterally. Lateral canthal tendon laxity is evaluated by pulling the lower lid medially and measuring the distraction of the lateral commissure. Movement greater than 2 mm in either test is considered abnormal. Canthal tilt can then be measured by marking the angle between a line extending from the lateral canthus to the medial canthus and a horizontal line extending from the lateral canthal crease across the nasal bridge ( Fig. 2.5 D). Its measurements are reported as being positive (when the lateral canthus is located 5 to 8 degrees higher than the medial canthus), negative (reverse of positive), or neutral (no angle between). ( Fig. 2.5 ). 12 The canthal tilt can be influenced by various factors such as anatomy, ethnicity and aging. A positive medial canthal tilt is considered a hallmark of facial female attractiveness 13 and should be paid attention to during lower eyelid blepharoplasty.
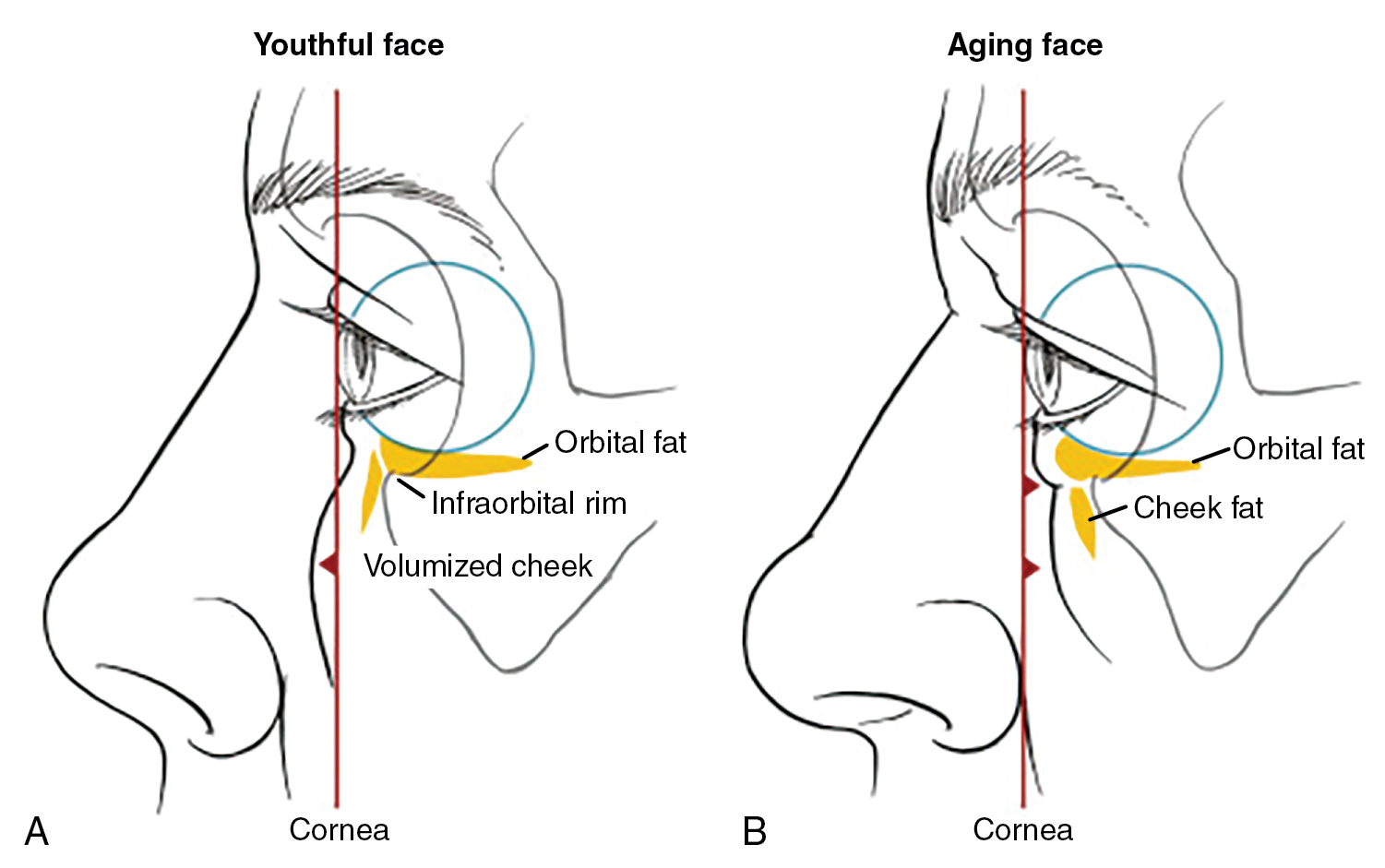
The examination concludes with notation of the lower lid fat pads. These are best observed when the patient is instructed to look upward. A negative vector is noted if there is a bulging globe relative to the malar prominence. A more conservative skin excision should be planned by the surgeon in this setting ( Fig. 2.9 ) . Particular attention should be paid to the presence of periorbital hollows (as they could represent bony deformities) and any signs of muscle displacement. While lower lid fat pads are generally easy to identify, they too can be made more prominent with an upward gaze and can also be more thoroughly assessed by gently pressing the globe while the patient’s eyes are closed, and then observing the change in the fat pad protrusion.
Snap back test
The Snap Back Test is conducted by pulling the lower eyelid inferiorly and away from the globe, holding 2 to 3 seconds, and then releasing (see Fig. 2.7 ). The physician should then note whether or not the lid returns to its original position (OP) and record the time it takes for the eyelid to return to that OP, or the “new” position. The test should be completed without the patient blinking. The patient receives a grade, 0 to 4, with 0 being an immediate snap back to OP where one can actually hear a snapping sound as it returns to its position, 1 taking 2 to 3 seconds to OP, 2 taking 4 to 5 seconds to OP, 3 taking more than 5 seconds to OP, and 4 if it does not return to the OP.
Distraction test
The Distraction Test is conducted by pulling the lower lid in an inferior direction from the globe and then measuring the distance. Distraction greater than 6 mm is abnormal and therefore considered a positive test (see Fig. 2.7 ).
In conjunction with a lower blepharoplasty, many patients will benefit from a chemical peel or ablative laser resurfacing since there may be fine periorbital rhytides. In addition, partial removal of the fat pads can cause skin laxity. The patients need to be the appropriate skin type, Fitzpatrick I-III, in order to avoid potential postinflammatory hyperpigmentation. For darker skin types, the authors (HBG, DMS) will perform multiple nonablative fractional treatments postoperatively. Newer technologies such as microneedling (using semi-insulated microneedles) with radiofrequency may also be used in patients with darker skin types.
Facelift
Patient selection
For the appropriate patient, a rhytidectomy can be a profoundly rejuvenating procedure. Despite its overall decline in popularity among cosmetic procedures, the facelift remains the cornerstone and gold standard of facial and neck rejuvenation. Relatively speaking, facelifts have split into two camps, one touting a less invasive approach, albeit more than the first one performed by Suzanne Noel, which was described as a skin-only procedure in the early 20th century. In reality, the methods used and their overall success depends on several factors, including the surgeon’s surgical technique, patient selection which encompasses patient’s skin, muscle, and bone conditions, among other factors.
Because of the tabloids and social media, many patients are misinformed about what a rhytidectomy is and is not. Given innovations over the past several decades, facelifts can be increasingly customized to each patient’s needs. Proper patient selection depends on the physical characteristics of their aging face as well as their emotional and mental readiness for this type of invasive procedure. Educating the patient and setting expectations including the recovery time and results is critically important. Optimally, the patient should have some form of emotional support structure since the recovery process can be a prolonged journey. This can be a spouse, a family member, or even a close friend.
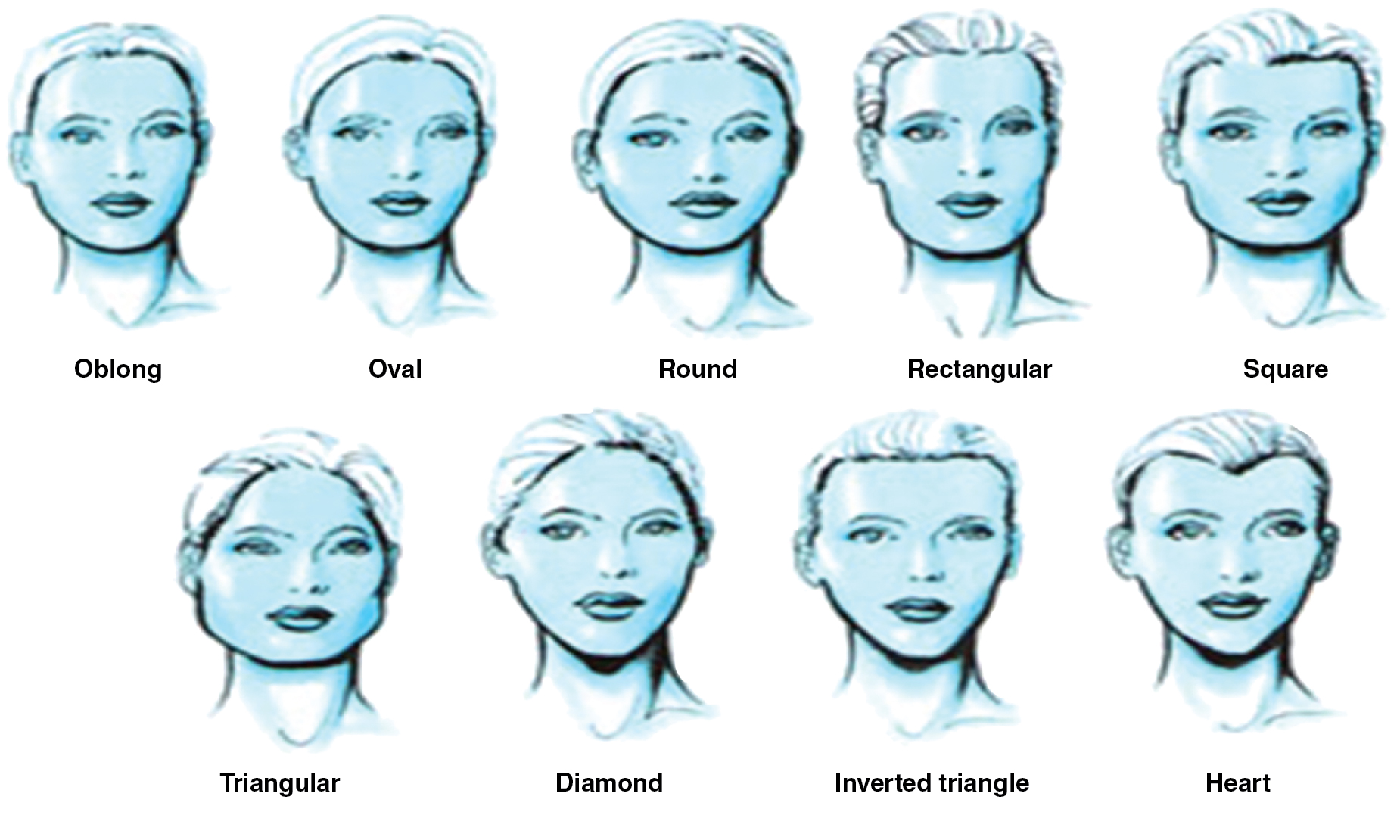
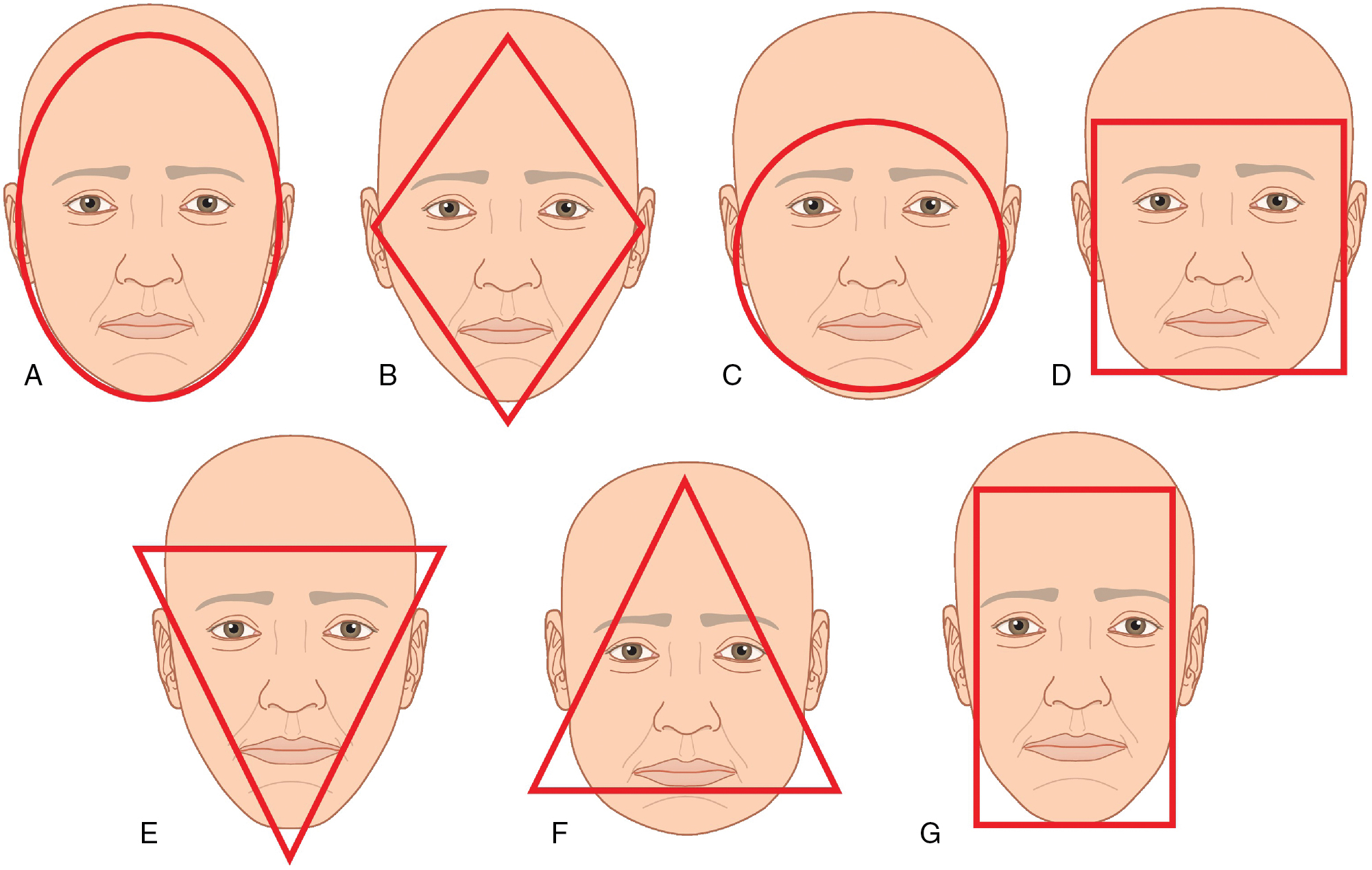
A facelift is a surgical lifting and tightening procedure. It will improve jowls, reduce marionette lines, and provide a stronger more clearly defined jawline. It can also elevate the mid face somewhat, increase volume if the SMAS plication technique is used, and for a lower facelift, the neck and the platysma will be lifted and tightened. It does not appreciably improve prominent nasolabial folds. Because a rhytidectomy lifts and tightens, there can be some improvement in rhytides and acne scars, but it is not the primary treatment for these conditions. Aside from adding, with some deep plain techniques, mild lateral and mid face volume, a facelift does not add significant volume. It is important to educate the patient on the goals and limitations of a facelift. In most patients, a facelift alone will not achieve an overall rejuvenation effect. Ancillary procedures such as laser resurfacing and fat transfer are routinely performed during the facelift procedure, and other fillers can be performed after the recovery period for additional volumization. Depending on the race and culture the ideal youthful face in women may be an oval or heart shape, while in men, a more rectangular shape is considered the aesthetic ideal across cultures ( Figs. 2.10 and 2.11 ).
While there are no set age limits for a facelift, given their elective yet invasive nature, one should be cautious when considering the geriatric population and their response to anesthesia. There are different types of rhytidectomies and different methods of anesthesia. A short scar or mini facelift using local anesthesia with oral sedation is the least invasive. It may require 90 minutes or less. Full lower facelifts combined with ancillary procedures such as resurfacing or blepharoplasties have been demonstrated by dermatologic surgeons to be safe using tumescent anesthesia and oral or IM sedation. Other more extensive rhytidectomies such as the deep plane technique may be better performed with IV sedation or general anesthesia. Certainly, the patient should be healthy. Senior author, HBG, has performed a full lower facelift on a female patient that was 82 years old and she was still practicing psychotherapy. The other end of the age range depends mostly upon genetics, Fitzpatrick skin type, and photo damage. Patients younger than 40 should be encouraged to consider noninvasive procedures first. Author HBG believes that the best candidates for facelifts are between the ages of 45 to 65 years. While the author DS agrees, he feels that age is less of a factor, gauging his decision solely by the patient’s health and the expected improvement he can deliver with the selected procedure.
For any cosmetic procedure, and specifically for a facelift, which is both a significant financial and emotional investment for the patient, proper patient selection is critical. It can be difficult during a single consultation to determine if the patient understands what a facelift will achieve. A facelift can help the patient appear naturally rested and rejuvenated. It can make them appear as their best self and reflect their internal vigor. Combined with many other factors, it can contribute to improved professional and social wellbeing, but it cannot do this alone. It is paramount that the patient has realistic expectations about the procedure and the outcome. Besides obtaining a medical clearance prior to surgery many surgeons require that the patient be evaluated by a psychologist for body dysmorphic disorder. A body dysmorphic questionnaire may or may not help depending on the patient’s self-awareness ( Appendices 2.1 and 2.2 ). Often having a cosmetic consultant and a second consultation will provide another opinion and a second opportunity for both sides to ask questions. As mentioned, facelifts can be successful in older patients, but expectations need to be tempered due to the loss of skin elasticity. Patients with previous rhytidectomy can certainly have satisfying second facelifts, but it is important to discuss with them that the recovery may take longer, there is a higher chance of complications like bleeding/hematoma, and that the results may not be the same as the previous one. Furthermore, repeat cases may have significant scar tissue and this may increase both the anesthesia time and surgical complexity. Therefore, increased risk and increased cost should be considered.
| Are you very concerned about the appearance of some part of your body, which you consider especially unattractive? | Y | N | ||
| If no, thank you for your time and attention. You are finished with this questionnaire. | ||||
| ********************************************** | ||||
| If yes, do these concerns preoccupy you? That is, you think about them a lot and they are hard to stop thinking about? | Y | N | ||
| What are these concerns? What specifically bothers you about the appearance of these body parts? ___________________________ | ________________________________________ | |||
| _________________________________________________________________________________________________________ | ||||
| _________________________________________________________________________________________________________ | ||||
| _________________________________________________________________________________________________________ | ||||
| What effect has your preoccupation with your appearance had on your life? | ________________________________________ | |||
| _________________________________________________________________________________________________________ | ||||
| _________________________________________________________________________________________________________ | ||||
| Has your defect often caused you a lot of distress, torment or pain? How much? (Circle best answer) | ||||
|
|
|
|
|
| Has your defect caused you impairment in social, occupational or other important areas of functioning? How much? (Circle best answer) | ||||
|
|
|
|
|
| Has your defect often significantly interfered with your social life? | Y | N | ||
| If yes, how? ______________________________________________________________________________________________ | ||||
| _________________________________________________________________________________________________________ | ||||
| Has your defect often significantly interfered with your school work, your job, or your ability to function in your role? | Y | N | ||
| Are there things you avoid because of your defect? | Y | N | ||
| _________________________________________________________________________________________________________ | ||||
| _________________________________________________________________________________________________________ | ||||
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


