Introduction
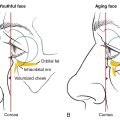
The eyes are arguably the most noticeable feature of the upper third of the human face. Their expressivity accounts for a significant proportion of non-verbal communication between individuals. Periorbital cutaneous aging is bothersome and easily noticeable to patients. It manifests clinically as brow ptosis, drooping of excess upper eyelid skin (dermatochalasis) and periorbital fat herniation of both the upper and lower eyelids leading to visible periocular fullness ( Fig. 4.1 ). These features are compounded by periorbital rhytid formation and often result in a prematurely aged facial appearance.

Given the increased incidence of skin cancers presenting in the periocular region, eyelid surgery has become a mainstay of practice for most dermatological surgeons worldwide. Dermatologic surgeons have acquired an in-depth knowledge of both ocular and periocular anatomy and special techniques which enhance periocular health and cosmesis. As such, many dermatologic surgeons now also perform eyelid surgery for a variety of indications, including cancer removal, reconstruction, and aesthetic periorbital rejuvenation. The following chapter is based on the experiences and insights gained from over 1,000 blepharoplasty cases performed at the Cosmetic Dermatologic Surgery Center at Mount Sinai & at Dr. Levit’s private practice.
Periorbital skin enhancement is an increasingly popular procedure and has been reported to be the third most commonly requested cosmetic surgery procedure. Periorbital skin enhancement may require the removal of skin, fat, muscle, or a mixture of these three elements and can be done using surgical or laser approaches. In trained hands, these procedures can safely produce excellent aesthetic results while preserving optimal eye function. The procedure, however, requires a robust knowledge of relevant periocular anatomy and precise surgical and/or laser technique. In addition, these procedures require careful consideration of the individual’s anatomy, medical history, and aesthetic goals. In this chapter, we will discuss our methods for performing upper eyelid blepharoplasty on Caucasian eyes. In the following chapter, lower eyelid blepharoplasty will be discussed. In Chapter 6 , we will discuss upper eyelid blepharoplasty in Asians, which requires a unique technique and additional knowledge of Asian eyelid anatomy. Some surgeons perform a brow lift in combination with blepharoplasty, the indications and applications of this procedure were discussed in Chapter 3 .
Blepharoplasty
The blepharoplasty procedure may be performed on either the upper eyelids, lower eyelids, or both. Upper eyelid blepharoplasty is the removal of redundant eyelid skin with or without the removal or repositioning of periorbital fat and muscle for the purposes of enhancing ocular function or, more commonly, for periorbital rejuvenation. The decision for skin-only removal versus additional removal or repositioning of fat and muscle is determined on a case-by-case basis. Traditionally, blepharoplasty is done using a scalpel. More recently, however, laser or electrosurgical devices are being successfully used as they have the additional advantage of hemostasis with improved intraoperative visibility and reduced postoperative bruising. The techniques for upper eyelid blepharoplasty in comparison to lower eyelid blepharoplasty are different, and their requirements are assessed by incorporating some basic principles, which we will discuss below.
Anatomical structures pertinent to blepharoplasty
In this section, we will summarize the basic anatomical concepts of upper eyelid blepharoplasty. For a more in-depth anatomical discussion, the reader should refer to Chapter 1 .
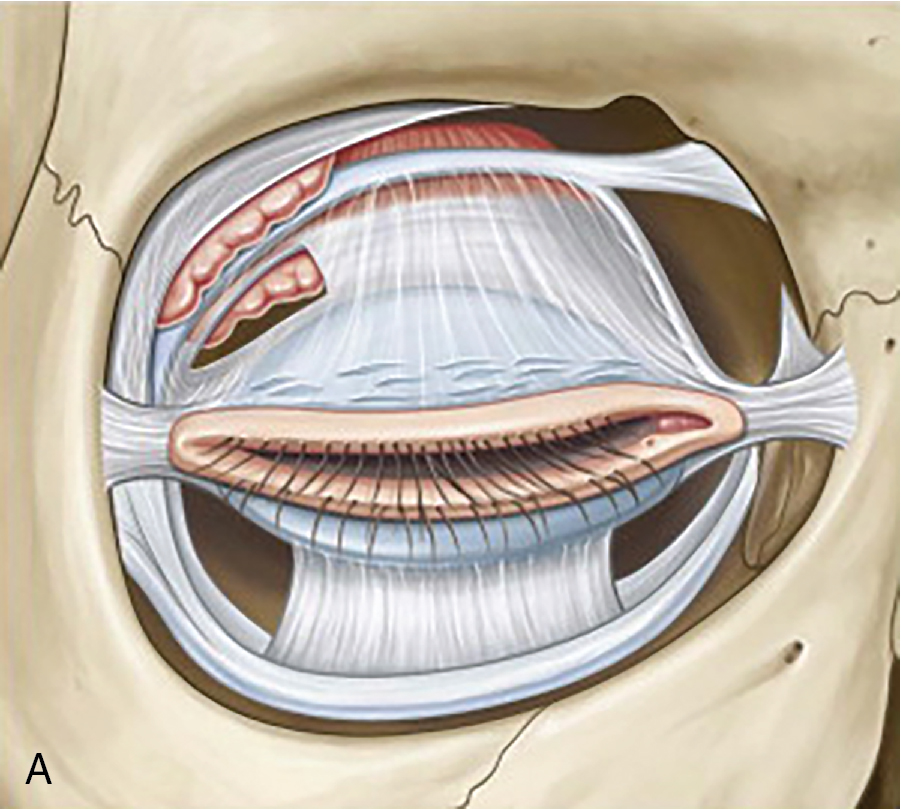
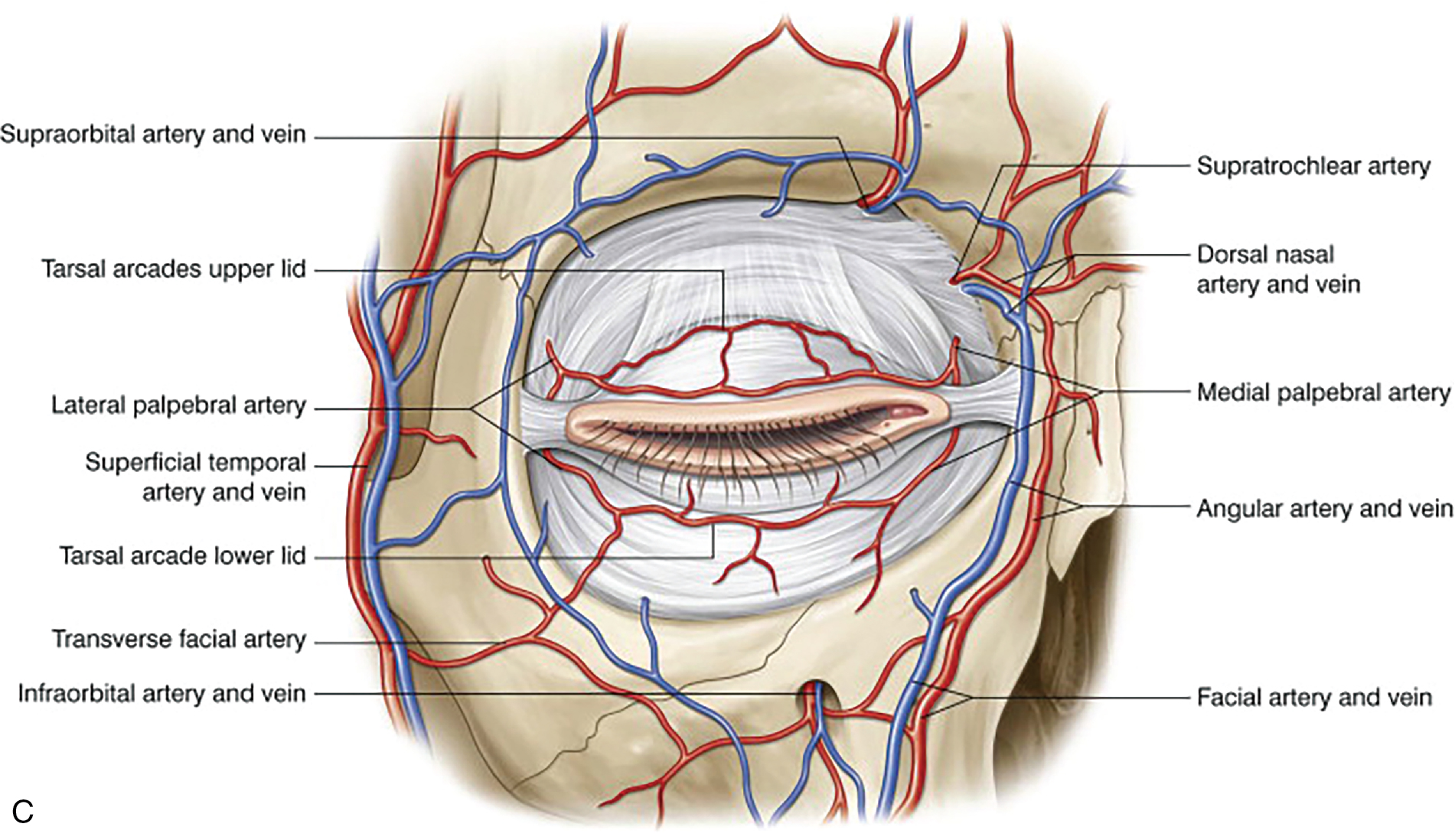
Starting from the skin, it is important to note that eyelid skin has a very thin dermis; thus, there is typically no need for a layered closure involving dermal sutures. Immediately below the dermis is the pinkish orbicularis oculi muscle. Note that there is a lack of subcutaneous fat. A strip of orbicularis is often removed to recreate the orbital crease, or a larger muscle sheet is removed in cases where a patient may have a very heavy upper lid. After the muscle strip is removed, one can visualize the glistering white orbital septum, which is covering the fat compartments ( Fig. 4.2 A). It is important to be able to identify the color, size, and shape of various fat compartments in the upper orbit (see Fig. 4.2 B). For instance, the nasal fat pad is cone shaped and whitish in color as compared to the more tubular, bright yellow central fat pad. A ptotic lacrimal gland can occasionally be visualized in the lateral compartment, which is pinkish in color. The lacrimal gland must not be removed but can be plicated to the periosteum of the lateral orbital rim. The vascular arcade of the upper eyelid is sandwiched between the orbicularis oculi muscle and orbital septum (see Fig. 4.2 C). These vessels are under low pressure, which is of greater importance in lower eyelid surgery and less so in upper eyelid surgery. Although major bleeding complications are not a big concern, micro-hematomas are occasionally encountered in cases where a patient has received local anesthesia with a needle (see Fig. 4.2D ). Therefore, the author HK prefers to use a cannula for numbing.


Patient selection
Proper patient selection is key to performing safe and successful blepharoplasties. Particular emphasis should be placed on counseling patients, setting realistic goals, and managing expectations. For more details regarding preoperative assessment, the reader should refer to Chapter 2 . Refer to appendix to see HK’s pre and post-op instructions for upper and lower blepharoplasty.
 VIDEO 2.1)
VIDEO 2.1)- 1.
Identification of the reason for performing a blepharoplasty, that is, functional loss with visual field decline secondary to dermatochalasis, skin cancer of the upper eyelid or aesthetic enhancement.
- 2.
Assessment of the patients’ current facial anatomy, including any pre-existing asymmetry or structural anomalies, should be discussed and accurately photographically documented. Attention should also be given to the texture and quality of the periorbital skin, and the presence or absence of fat herniation versus festooning (including lid lag and lid laxity which are tested using the snap test).
- 3.
Particular attention should be given to brow position and symmetry. Is the patient a good candidate for a traditional brow lift? Or is the patient better candidate for a trans-blepharoplasty brow fixation? In both cases, a more conservative skin excision needs to be planned. Conservative skin removal should also be considered for patients with a negative vector (discussed in Chapter 2 ) as the upper eyelid will have to cover more surface area for eyelid closure.
- 4.
Determining whether optimal results can be achieved via removal of skin alone versus a combination of fat and skin. Conservative fat removal is the preferred method by the authors to avoid unnecessary hollowing and skeletalization of the orbit.
- 5.
Assessment of individual patient needs and managing realistic expectations.
- 6.
The identification of existing co-morbidities and risk factors prior to the procedure, such as glaucoma, thyroid ophthalmopathy, anticoagulant usage, pacemaker, or defibrillator placement, among others.
- 7.
A thorough evaluation of pre-existing dry eyes with Schirmer’s test (see Chapter 2 ) is advisable in conjunction with a preoperative ophthalmological examination, including visual acuity.
- 8.
It is good practice to show patients photographs representing realistic outcomes of both pre- and postoperative results, as well as wound healing timelines illustrated with photographs. Best-case and worst-case scenarios should be reviewed from previous patients and discussed in detail; both for patient understanding as well as for legal protection and documentation.
Upper eyelid blepharoplasty technique
Patient marking (see  and )
and )
Preoperative skin marking for upper eyelid blepharoplasty involves identification of the upper eyelid crease (supra-tarsal skin fold) and determining the appropriate amount of tissue for removal to achieve an optimal cosmetic outcome while maintaining proper eyelid function. The patient should be sitting upright in a neutral gaze position during the skin marking process prior to local anesthetic delivery.
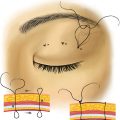
The inferior margin is marked across the mid-pupillary line, approximately 8 to 12mm in female patients and 8 to 10mm in male patients from the ciliary margin (ideally in the natural skin crease). One must take into account variations across ethnic variations and levator dehiscence. The former can lower the crease (particularly in Asian eyelids), while the later can raise it. The punctum is a safe landmark for the medial extension of the incision. Extending the incision past the punctum may result in webbing. The lateral marking can be extended to the lateral canthus or immediately past the orbital rim in cases where lateral hooding might be present (see Fig. 4.1 ). The medial and lateral positions of the lower marking are marked 5mm above the medial and lateral canthus and never less than 3mm from the lash line. The superior margin is marked by using Bishop Harmon forceps and gently pinching the excess skin while marking. For safety, the superior margin should not be less than 10mm from the brow (natural unplucked/untattooed position), allowing at least 20mm of skin to be left behind for proper closure of the eyelid. The distance between the lower and upper margins will determine the amount of skin removal required for a tension free closure ( Fig. 4.3 ). The pinch test using the Bishop Harmon forceps can be used to confirm skin markings, ensure eyelid closure, and allow for conservative skin excision. In younger patients, skin markings are usually lenticular, but the shape at the lateral edge can be modified to a trapezoid to allow for the removal of excess lateral eyelid skin typically required amongst older patients (see Fig. 4.4 ).



Local anesthesia
Upper eyelid blepharoplasty can be an office-based procedure under local anesthesia with or without sedation in the appropriate patient setting. Typically, 1% lidocaine with a 1:100,000 dilution of epinephrine is used. These preparations may be buffered with sodium bicarbonate to decrease patient discomfort secondary to pH mismatch. Alternatively, a 50:50 mixture of lidocaine and ropivacaine may be used following the initial lidocaine injection to provide a prolonged anesthetic effect. Furthermore, ropivacaine has vasoconstrictive properties which can aid in hemostasis. For additional hemostasis in patients who are prone to bleeding, the author HK prefers to add tranexamic acid (TXA) to the mixture. Each eyelid is then anesthetized with 3mL of this mixture. The lidocaine solution should be injected superficially above the orbicularis. The author HK prefers a 27-gauge cannula with a 25-gauge needle used at the lateral brow for entry to avoid bruising and micro-hematomas postoperatively ( Fig. 4.4 ).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


