Introduction
Forehead and brow lifting procedures are performed by cosmetic surgeons to correct changes from aging to the upper face. They afford long-term improvement of brow positioning and, depending on the technique, improvement in forehead and glabellar rhytids. They can be performed with local and tumescent anesthesia or done under general anesthesia at the surgeon’s preference. Compared to repeated neuromodulator injections, cosmetic outcomes are considered permanent.
There are many valid techniques for forehead and brow lifting ( Fig. 3.1 ). Each technique has its own advantages and disadvantages, and appropriate patient selection is crucial. In general, approaches to forehead and brow lifting may be “open,” meaning that there is direct visualization during dissection. The incision can be coronal or trichophytic, which is sometimes called pretrichial or transfollicular. A “minimally invasive” approach requires the use of an endoscope to visualize dissection around sensitive structures and the incisions are usually placed in the frontal scalp. Alternatively, approaches for brow lifting alone can be “direct,” where the incision is made in the suprabrow or transblepharoplasty, where the incision from a concomitant blepharoplasty in the lid crease is used. Mid-forehead, where the incision is made in a deep forehead furrow is a technique that often results in unacceptable scarring and will not be discussed further in this chapter.

Steps involved in brow lifting are access incision, dissection plane, mobilization of the brow and/or forehead (which may include depressor muscle manipulation), and finally, brow elevation with skin excision and/or fixation of the brow in its desired position.
It is important for cosmetic surgeons to be familiar with this procedure and understand when a brow lift is indicated. As opposed to repeated blepharoplasties, which may cause the brow to descend and can leave the patient with a “brow cripple,” a combination procedure may yield better outcomes. Repeated blepharoplasties can also prohibit brow lifting as there would not be enough upper lid skin available to close the eyes.
Indication
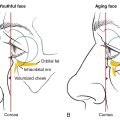
Brow position and forehead appearance are determined by the underlying bony anatomy, contraction of antagonistic muscles, gravity, and natural aging. Optimal brow positioning varies between men and women. In men, the brow should be relatively flat and sit at or slightly below the level of the supraorbital rim. In women, the brow should sit above the supraorbital rim, with an arch that peaks at the lateral limbus.
Noninvasive options like neuromodulators, dermal fillers, thread lifting, and heat-based devices provide temporary results that are best used in younger patients and those who desire nonsurgical treatment. Surgical candidates who seek long-term results may be offered an aesthetic brow lifting procedure.
Evaluation
The simplest way to evaluate the patient for brow and forehead lift is to manually elevate the eyebrows while the patient is looking in a mirror to see if they feel that it is a positive change. An additional method of diagnosis and prediction is to have the patient recline while lifting their chin and looking in a handheld mirror. Gravity will usually elevate the brows to the same position that a surgical procedure would. The surgeon can also take a photograph of the patient while reclined with their chin elevated. Although the lower and mid-face will be somewhat distorted the brows would be in the same position as if they were surgically elevated.
Patient selection (preoperative considerations and choosing different options)
When thinking about the various options of brow lifting for a patient, there are a number of factors to consider. For instance, does the patient desire both brow and forehead rejuvenation? Do they have thinning hair or a receding hairline? Is their forehead long or short? Is their skin texture rough and coarse?
Open procedures create brow lifting and rhytid flattening by excising excess skin, which also makes these procedures irreversible. They pose a rare risk of temporary numbness of the scalp if the supra-frontalis branches of the supraorbital and supratrochlear nerves are transected with the skin excision. Trichophytic incisions shorten the forehead whereas coronal incisions lengthen the forehead. Trichophytic incisions are at higher risk of being visible and should be avoided in those with thinning hair or with a short forehead. Coronal incisions may also be visible, but since they are further into the scalp, they are better hidden. Intraoperative visibility with an open procedure is superior to an endoscopic approach. However, a highly curved forehead may limit visibility in an endoscopic approach.
Endoscopic procedures use smaller incisions and do not utilize skin excision. Rather the brow is elevated through fixation. The forehead may be raised and some forehead elevation is gained but not to the same degree as open procedures. Endoscopic instrumentation is necessary, which can be expensive and also carry a steeper learning curve. Furthermore, there is a small risk of fixation failure and extrusion of the fixation material and foreign body granulomas.
Direct brow approach yields the best control over the location and shape of the brow but may leave visible scarring if not hidden in a thick eyebrow. Transblepharoplasty allows for a single well-hidden incision during a concomitant blepharoplasty. Each of these approaches require fixation of the brow to its desired location. There is no forehead elevation with these procedures, but the glabellar complex can be dissected to improve glabellar rhytids.
Risks in all procedures include scarring, sensory loss, alopecia, and loss of elevation over time. Due to their larger incisions, the pretrichial and coronal procedures are more prone to sensory changes. Motor nerve changes are rare but meticulous surgical technique and dissection is required. The most commonly injured motor nerve is the frontal branch of temporal nerve (particularly in thin patients). However, these injured branches are the most distal branches of this nerve and partial or full recovery can be expected by 9 months. As a general rule, transection of a nerve medial to a line drawn vertically by the lateral canthus tends to recover as opposed to a more proximal nerve trunk injury. Alopecia can result if there is undue tension at the incision site or from an underlying fixation device.
In terms of dissection, subcutaneous dissection offers the most significant rhytid improvement and very accurate brow placement, but limitations include decreased flap vascularity, which may lead to alopecia, dehiscence, and paresthesia. Subgaleal plane may provide less flap tension than all the other dissection planes and easier release of muscles at their insertion. Subperiosteal dissection better preserves the subgaleal vascular plexus and sensory nerves, limiting alopecia and paresthesia. The subcutaneous approach allows dissection to be superior to the various sensory nerve branches traversing the forehead. Deeper approaches may transect these nerves.
Like any procedure, the best technique is often the one that the surgeon feels most comfortable with in planning and execution, which is of course surgeon specific. However, there are advantages and disadvantages to specific techniques that may be more appropriate for certain patients. A skilled surgeon with experience in multiple techniques will best be able to serve a diverse patient population.
Fixation
Fixation techniques are essential for providing brow lift in non-open procedures, but can also be used in conjunction with skin excision in open procedures.
The goal of fixation is to maintain brow position until wound healing is complete, about 6 to 8 weeks postoperatively. The ideal device should be effective, reproducible, minimize complications, training, and cost. It should be noted that for any fixation technique to be effective, there must be complete brow release because fixation under tension will lead to relapse.
With the introduction of the endoscopic approach, there have been multiple fixation products, devices, and techniques that have been introduced and described. These include fibrin glue, external bolsters, suspension sutures, bolster sutures, screws, miniplates, K-wires, bone tunnels and Endotine. Each technique carries its own risks and benefits including loss of elevation, alopecia, scarring, palpability, infection and potential for dural injury. Dural injury from drilling techniques has been published in case reports but may be underreported.
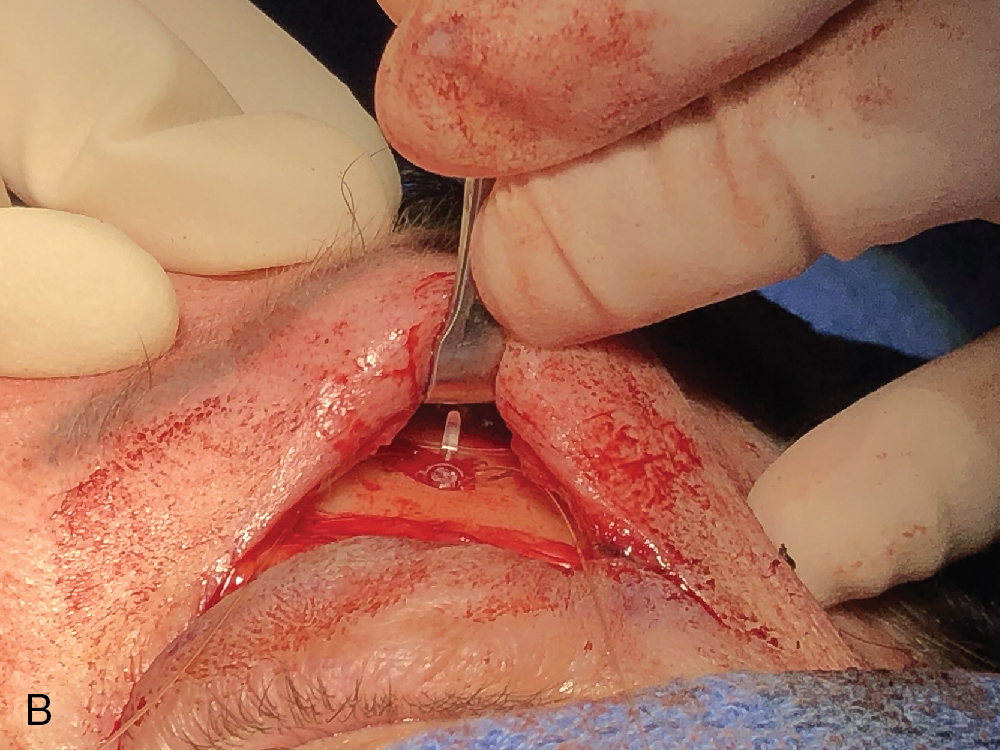
The MicroAire Endotine fixation device (Coapt Systems, Palo Alto, CA) is a sutureless bioabsorbable device made of polylactic acid ( Fig. 3.2 A and B). It has a bore that is drilled into the frontal bone for direct and endoscopic procedures or into the superior orbital rim during a direct or transblepharoplasty procedure. It has multiple tines for fixation which spreads out the tension over a larger area of the overlying skin, giving it a more secure hold. It also has two holes ( Fig. 3.2 A) which the surgeon can utilize to pass a suture through and fixate it to periosteum for additional security. The Endotine fixation device comes with three tine sizes, 3.0, 3.5, and 4.0 mm, based on the surgeon’s assessment of skin thickness. It may be visible and slightly palpable at first but this declines over time. It provides support and fixation for approximately 3 months postoperatively.

Anesthesia
Anesthesia is usually provided by a combination of nerve blocks, tumescent anesthesia, and anxiolytics. General anesthesia may be used, especially with endoscopic procedures.
Each procedure
The trichophytic, or transfollicular brow and forehead lift, which is author JN’s preferred method, will be discussed in detail. Only the salient points of other techniques will be reviewed.
Trichophytic (transfollicular brow and forehead lift)
An incision is made 5 mm posterior to the frontal hairline, at the beginning of thicker terminal hair ( Fig. 3.3 ,  ). It is best performed with a random, undulating z-plasty pattern. The author recommends using an #11 blade to incise with a severe bevel of 10 to 15 degrees, which will allow transected hairs to penetrate and grow through the scar ( Figs. 3.4–3.6 ). Dissection can be performed in the subcutaneous, subgaleal or subperiosteal space but the author recommends a subcutaneous dissection to preserve sensory branches around the frontal hairline and for optimal rhytid improvement. Pretunneling may be performed with a dedicated spatula or a non-suctioning liposuction cannula. Dissection is then performed with facelift scissors, in a cut-and-spread fashion, up until 2 cm superior to the supraorbital rim ( Fig. 3.7 ). Further dissection is done cautiously and under direct vision with the use of a lighted retractor to preserve neurovascular structures. Dissection around the supraorbital and supratrochlear neurovascular bundles to release the entire brow is critical and is easier with the scissors in the vertical direction ( Fig. 3.8 ). It should be carried out to a level below the supraorbital rim, laterally to the brow. In older patients this may extend to the temporal crests, but not beyond and care must be taken to not injure the frontal nerve (a branch of the ophthalmic nerve (V1) of the trigeminal nerve). Once the brow is completely mobilized from the retaining ligaments of the orbit, a midline cutback and lateral cutbacks at the maximum desired brow peak are performed ( Fig. 3.9 ). An assistant should push the proximal scalp forward to help neutralize the scalp position to accurately predict the amount of cutback, which averages 15 mm centrally and 20 mm laterally, but varies depending on the amount of skin excess ( Fig. 3.10 ). Cutbacks are secured with 4-0 or 5-0 absorbable gut sutures. Excess skin is then trimmed with special attention placed so that the same exact angle of bevel and zigzag pattern is matched to the initial incision ( Fig. 3.11 ). One may find it easier to excise smaller 3- to 4-cm strips of skin as opposed to one long strip. Subcutaneous sutures are optional. Closure is with buried 5-0 absorbable gut suture along the incision line and running or interrupted 5-0 gut, nylon or prolene suture superficially ( Fig. 3.12 ). Lasers or chemical peels should be performed only by those with experience on lipocutaneous flaps. Compression is not needed and is actually avoided by the author due to worsening eyelid edema.
). It is best performed with a random, undulating z-plasty pattern. The author recommends using an #11 blade to incise with a severe bevel of 10 to 15 degrees, which will allow transected hairs to penetrate and grow through the scar ( Figs. 3.4–3.6 ). Dissection can be performed in the subcutaneous, subgaleal or subperiosteal space but the author recommends a subcutaneous dissection to preserve sensory branches around the frontal hairline and for optimal rhytid improvement. Pretunneling may be performed with a dedicated spatula or a non-suctioning liposuction cannula. Dissection is then performed with facelift scissors, in a cut-and-spread fashion, up until 2 cm superior to the supraorbital rim ( Fig. 3.7 ). Further dissection is done cautiously and under direct vision with the use of a lighted retractor to preserve neurovascular structures. Dissection around the supraorbital and supratrochlear neurovascular bundles to release the entire brow is critical and is easier with the scissors in the vertical direction ( Fig. 3.8 ). It should be carried out to a level below the supraorbital rim, laterally to the brow. In older patients this may extend to the temporal crests, but not beyond and care must be taken to not injure the frontal nerve (a branch of the ophthalmic nerve (V1) of the trigeminal nerve). Once the brow is completely mobilized from the retaining ligaments of the orbit, a midline cutback and lateral cutbacks at the maximum desired brow peak are performed ( Fig. 3.9 ). An assistant should push the proximal scalp forward to help neutralize the scalp position to accurately predict the amount of cutback, which averages 15 mm centrally and 20 mm laterally, but varies depending on the amount of skin excess ( Fig. 3.10 ). Cutbacks are secured with 4-0 or 5-0 absorbable gut sutures. Excess skin is then trimmed with special attention placed so that the same exact angle of bevel and zigzag pattern is matched to the initial incision ( Fig. 3.11 ). One may find it easier to excise smaller 3- to 4-cm strips of skin as opposed to one long strip. Subcutaneous sutures are optional. Closure is with buried 5-0 absorbable gut suture along the incision line and running or interrupted 5-0 gut, nylon or prolene suture superficially ( Fig. 3.12 ). Lasers or chemical peels should be performed only by those with experience on lipocutaneous flaps. Compression is not needed and is actually avoided by the author due to worsening eyelid edema.