Synopsis
- ■
Nerve injuries are often devastating, with associated pain and impaired function.
- ■
Motor nerve injuries must be managed expeditiously, because regenerating axons must reach target muscle prior to degeneration and fibrosis – “time is muscle”.
- ■
Nerve transfers offer an advantageous method of reconstruction by delivering regenerating nerve fibers to the target end organ more quickly, thus converting a proximal injury to a more distal injury.
- ■
Nerve transfers allow for dissection outside the original zone of injury, providing a safer and more technically straightforward procedure.
- ■
Unlike tendon transfers, the muscle–tendon biomechanical structure is preserved; thus, excursion, origin, insertion, and length–tension relationships are undisturbed.
- ■
Nerve transfers require time for the nerve to regenerate and extensive physical therapy for retraining.
- ■
Intraneural dissection is technically demanding, and nerve transfers require intimate knowledge of nerve topography.
Keywords
nerve, nerve injury, nerve transfer, nerve reconstruction, nerve palsy
Synopsis
- ■
Nerve injuries are often devastating, with associated pain and impaired function.
- ■
Motor nerve injuries must be managed expeditiously, because regenerating axons must reach target muscle prior to degeneration and fibrosis – “time is muscle”.
- ■
Nerve transfers offer an advantageous method of reconstruction by delivering regenerating nerve fibers to the target end organ more quickly, thus converting a proximal injury to a more distal injury.
- ■
Nerve transfers allow for dissection outside the original zone of injury, providing a safer and more technically straightforward procedure.
- ■
Unlike tendon transfers, the muscle–tendon biomechanical structure is preserved; thus, excursion, origin, insertion, and length–tension relationships are undisturbed.
- ■
Nerve transfers require time for the nerve to regenerate and extensive physical therapy for retraining.
- ■
Intraneural dissection is technically demanding, and nerve transfers require intimate knowledge of nerve topography.
Brief introduction
- ■
Nerve transfers can be performed to restore sensory or motor deficits and essentially convert a proximal injury to a distal injury, providing a source of regenerating axons in close proximity to the end target.
- ■
Advantages of nerve transfers:
- •
Bring regenerating motor fibers closer to the target end organ more rapidly, essentially converting a more proximal-level injury to a more distal-level injury.
- •
Enable surgical reconstruction outside the zone of the original injury, avoiding complex dissections and limiting injury to critical neurovascular structures.
- •
Allow for a very targeted intervention in cases of partial nerve.
- •
Unlike tendon transfers, nerve transfers require only minimal immobilization (7–10 days), which is especially valuable in patients presenting with significant baseline stiffness.
- •
Preserve the biomechanical properties of the musculotendinous unit.
- •
Can restore unique function such as pronation, which is incredibly difficult to restore by traditional surgical techniques.
- •
- ■
Indications for nerve transfers ( Table 25.1 ).
Table 25.1
Indications for nerve transfer
- •
Proximal brachial plexus injuries where grafting is not possible
- •
Proximal peripheral nerve injuries requiring long distance for reinnervation of distal targets
- •
Severely scarred areas with risk of damage to critical structures
- •
Segmental nerve loss
- •
Major upper extremity trauma
- •
Partial nerve injuries with functional loss
- •
Delayed presentation with inadequate time for reinnervation of distal targets with grafting
- •
Sensory nerve deficits in critical regions
- •
- ■
Absolute contraindications:
- •
End organ unresponsiveness.
- •
Muscle that is in complete discontinuity with the nerve for greater than 1 year will not be reinnervated no matter the elaborate reinnervation strategy employed.
- •
- ■
Relative contraindications:
- •
Extensive time required for regeneration
- •
Surgeon inexperience: challenges of the surgery, the anatomic knowledge required, and problems of postoperative retraining and therapy.
- •
Patients who may prefer the more rapid recovery associated with tendon transfer at the expense of the independent fine motor control that could be achieved through the use of nerve transfers.
- •
- ■
The most relevant recent basic science advances pertaining to nerve transfers relate to end-to-side transfers ( Fig. 25.1 ) .
- •
End-to-side neurorrhaphy involves the coaptation of the distal end of an injured recipient nerve into the lateral aspect of an intact nerve, which serves as a proximal source of axons to regenerate into the injured nerve.
- •
Sensory recovery has typically been more impressive than motor recovery.
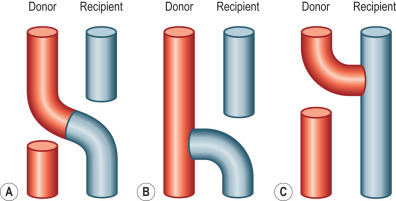
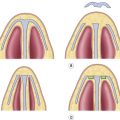
Figure 25.1
The various options for coaptation in nerve transfer. (A) End-to-end coaptation between the donor nerve (red) and the recipient nerve (blue). (B) End-to-side coaptation, where the distal end of the divided recipient nerve (blue) is transferred to the side of the intact donor nerve (red). In this transfer, fascicles from the donor will “sprout” into the distal donor nerve. The recipient nerve essentially “pulls” the donor fascicles into the distal nerve. (C) Reverse end-to-side coaptation. In this transfer, the donor nerve (red) has been divided and transferred to the side of the intact recipient nerve (blue). The donor essentially “pushes” regenerating fascicles into the distal donor nerve.
- •
- ■
Reverse end-to-side nerve transfers involve the complete transection of the donor nerve, which is then coapted into the side of the intact recipient nerve.
- •
This maximizes the potential number of available motor axons from the donor nerve.
- •
This procedure does not interrupt any recovery in the injured recipient nerve because the nerve remains in continuity; however, the additional axons recruited from the donor nerve improve distal target reinnervation, a concept known as “supercharging”.
- •
In a proximal nerve injury, with a long distance required for reinnervation, this technique can protect target muscles from denervation atrophy and fibrosis.
Hints and tips
The end-to-side transfer can be considered as the recipient nerve “pulling” regenerating axons out of the intact donor, whereas the reverse end-to-side transfer can be considered as the donor nerve “pushing” regenerating axons out into the intact recipient.
- •
- ■
The biggest challenge facing peripheral nerve surgeons is that with increasing time since injury, the ability to achieve good motor function becomes increasingly limited.
- •
For any nerve injury where there is complete discontinuity with the motor end organ, no reinnervation procedure will be able to restore muscle once denervation and fibrosis have occurred, a process which occurs as early as 1 year.
- •
- ■
Direct nerve repair and nerve grafting also remain valuable tools for the peripheral nerve surgeon and should continue to be the treatment of choice in a variety of scenarios, including:
- •
Multiple nerve injuries where there is a paucity of nerve donor material for nerve transfer.
- •
Distal single-function nerve injuries where direct or graft repair is preferable to nerve transfer because one-to-one function is preserved, no retraining is necessary, no donor function is sacrificed, and the distance to the end target is short.
- •
- ■
In the event of a failed nerve transfer and the necessity of further secondary procedures, there are several important considerations.
- •
When planning nerve transfers, one must consider the possible salvage procedures required should the transfer fail.
- •
Thus, when deciding on donor nerve, it is prudent to ensure that options are left for later.
- •
A donor for tendon transfer requires Medical Research Council grade 5 of 5 strength because following transfer it will be downgraded by a minimum of one grade.
Hints and tips
Avoid using a donor nerve that may be required for a secondary procedure such as a tendon transfer down the road. Prior to cutting a donor nerve, make sure the rest of the nerve performs all essential functions with fastidious intraoperative nerve stimulation.
- •
- ■
Tendon transfers have the benefit of not being restricted by time, given that distal motor denervation and fibrosis do not affect the outcome. For this reason, there is no harm in attempting a nerve transfer as a primary procedure and reserving the tendon transfer for a secondary procedure if the functional outcome is less than desired.
- ■
Nerve transfers should not be attempted if there are not suitable, redundant, available donors, as in the setting of a multinerve injury. In this setting, nerve grafting combined with tendon transfer, or even arthrodesis, may be warranted.
Preoperative considerations
- ■
On history, details of the mechanism and timing of injury are crucial. The mechanism of injury will determine timing of intervention, with prompt exploration of penetrating sharp trauma and more expectant management of closed injuries and gunshot wounds.
- ■
Specific patient symptoms such as loss of function, both sensory and motor, and pain should be precisely elicited, as this will help focus the subsequent physical examination.
- ■
A complete physical examination of the upper extremity includes assessment of sensory and motor function, deep tendon reflexes, joint suppleness, and range of motion.
- ■
Particularly in patients with late presentation, the presence of fixed joint contractures may preclude functional recovery.
- ■
Sensation should be examined by both dermatome and peripheral nerve distribution, and can be helpful in distinguishing these injuries. The authors advocate the use of both two-point discrimination and the ten-test to evaluate sensory loss in the hand.
- ■
A Tinel’s sign, the tingling sensation elicited with percussion over a regenerating nerve, will help to localize the level of nerve injury and may also be followed on serial clinical examination to check for signs of advancement, indicating spontaneous recovery.
- ■
An advancing Tinel’s sign quite often precedes actual motor recovery, which might be quite distal to the site of the initial injury.
- ■
The scratch collapse test is useful primarily for patients with nerve compression pathology, but also has a role in evaluating the patient for potential nerve transfer procedures, as it can provide additional confirmation of the level of nerve injury (
 ).
).
- ■
The test is performed by having the patient sit facing the examiner with their shoulders adducted, elbows held in 90° of flexion, neutral pronosupination, and wrist and fingers extended. The examiner will then lightly scratch the area of the presumed nerve injury and exert force to the patient’s arms in the direction of internal shoulder rotation as the patient resists. Nerve injury at the test site is indicated by the inward collapse of the arm on the side ipsilateral to the injury.
- ■
One of the most important components of the physical examination is the simple determination of what is functioning and what function has been lost.
- ■
In the presence of an injury requiring surgical intervention, it is important to examine the patient for putative nerve donors, both intraplexal and extraplexal (spinal accessory, medial pectoral, and thoracodorsal).
Hints and tips
Remember to check not only for what muscles have lost function, but also for potential nerve transfer donors.
- ■
Electrodiagnostic testing, performed by an experienced person, can be a useful adjunct to physical examination for serial assessment of reinnervation in closed nerve injuries.
- ■
Initial electrodiagnostic testing should be deferred until a minimum of 6–8 weeks postinjury to assess for signs of both axonal injury and root-level avulsion.
- ■
In patients with no evidence of recovery 3 months after a closed nerve injury, the balance should tilt towards consideration of surgical intervention.
Hints and tips
Order baseline electrodiagnostic studies at 6–8 weeks and subsequent testing as indicated by the injury. Fibrillations and positive sharp waves suggest denervation. Motor unit potentials and nascent units suggest reinnervation.
Patient selection
Anatomical/technical pearls for specific injury patterns
- •
Avoid or use short-term paralytics with anesthesia induction to allow for nerve stimulation.
- •
Minimize or avoid tourniquet time to avoid interference with nerve stimulation.
- •
Use plain epinephrine in proximal incisions to minimize blood loss without lidocaine paralysis.
- •
Obtain wide surgical exposure to identify nerves and appropriate branches.
- •
Choice of optimal nerve donor is based on quantity of motor axons, proximity to target muscles, synergy of muscle function, and donor expendability.
- •
Conduct neurolysis with your “eyes” except at the site of actual transfer to avoid prolonged dissection and increased trauma to nerve branches.
- •
Confirm no intraoperative stimulation in putative recipient before dividing donor.
- •
Divide donor nerve distally and recipient nerve proximally.
- •
Use 9–0 nylon and the operating microscope to perform tension-free epineurial repair.
- •
Use bupivacaine block at end of case for postoperative pain control.
Upper plexus injury
Specific patient exam findings
- ■
Upper plexus injuries involve injuries at the C5, C6, and/or C7 root or upper trunk level.
- ■
Commonly include deficits of:
- •
The dorsal scapular nerve innervates the rhomboid muscles and the levator scapulae muscles, which contribute to scapular adduction, retraction, and elevation.
- •
The long thoracic nerve innervates the serratus anterior muscle, which abducts the scapula, permitting the full range of shoulder flexion past 90°.
- •
The suprascapular nerve innervates the supraspinatus and infraspinatus muscles. These muscles are rotator cuff muscles. The supraspinatus contributes to shoulder abduction with the deltoid muscle. The infraspinatus contributes to shoulder external rotation with the teres minor.
- •
The axillary nerve arises from the posterior cord, receiving innervation from C5 and C6. Supplies the deltoid and teres minor muscles, which provide shoulder abduction and external rotation, respectively. Provides cutaneous innervation over the lateral shoulder.
- •
The musculocutaneous nerve arises from the lateral cord and is primarily innervated by C5, C6, and occasionally C7. Innervates coracobrachialis, biceps brachii, and brachialis, which power elbow flexion. The biceps is also the primary forearm supinator. The lateral antebrachial cutaneous (LABC) nerve is a terminal branch and provides cutaneous innervation to the lateral forearm.
- •
- ■
Patients with upper plexus injuries present with glenohumeral joint subluxation, loss of shoulder abduction and external rotation, and absent or weakened elbow flexion, depending on the involvement of C7. Numbness over the lateral shoulder and forearm is noted.
Specific operative techniques
Priorities for upper plexus injuries include restoration of shoulder external rotation and abduction, as well as elbow flexion. Standard transfers include: (1) spinal accessory to suprascapular nerve; (2) medial triceps to axillary nerve; and (3) double fascicular nerve transfer.
Use of spinal accessory nerve (cranial nerve XI) to suprascapular nerve transfer (motor)
- ■
Restoration of shoulder stability and external rotation are facilitated by transferring the spinal accessory nerve (cranial nerve XI) to the suprascapular nerve. This transfer can be conducted by either an anterior or a posterior approach ( Fig. 25.2 ) .
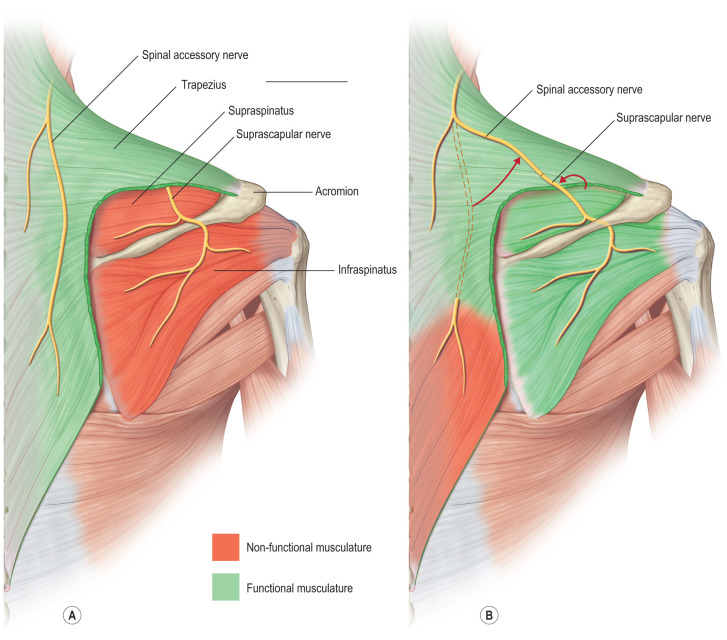
Figure 25.2
The posterior approach for spinal accessory to suprascapular nerve transfers. (A) The nerves can be seen in their original orientation. (B) The end-to-end transfer has been completed. The transfer includes the functional spinal accessory nerve (donor) being transposed and coapted to the non-functional suprascapular nerve (recipient).
- ■
Posterior approach:
- •
The spinal accessory nerve runs parallel to the border of trapezius and is localized 40% of the way along a line connecting the acromion to the dorsal midline at the level of the superior border of the scapula ( Fig. 25.3 ) .

Figure 25.3
Surface markings for posterior approach to spinal accessory to suprascapular. The spinal accessory nerve is located 44% of the way along a line connecting the dorsal midline to the acromion. The suprascapular nerve is located at the halfway point between the medial border of the scapula and the acromion on an obliquely oriented line at the superior aspect of the scapular spine. It runs in the suprascapular notch.
- •
The suprascapular nerve is located midway between the medial border of the scapula and the acromion as it runs through the suprascapular notch.
- •
The nerves are accessed through an incision located slightly obliquely just above the superior border of the spine of the scapula. Dissection is carried through the trapezius in a muscle-splitting fashion, and an end-to-end coaptation, sparing the upper trapezius nerve branches, is performed.
- •
- ■
Anterior approach:
- •
An incision is designed 2 cm superior to and parallel to the clavicle extending laterally from the posterior border of the sternocleidomastoid ( Fig. 25.4 ) .
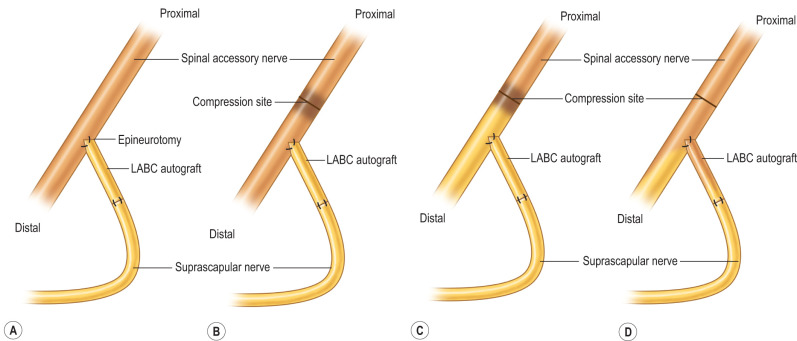
Figure 25.4
In the anterior approach to the spinal accessory to suprascapular nerve transfer, upper trapezius function is preserved by performing the nerve transfer in an end-to-side manner. (A) To inset this transfer with no tension, an interpositional lateral antebrachial cutaneous (LABC) nerve graft is used. (B) To facilitate regenerative sprouting, injury to the donor nerve is required proximally. This is accomplished by “crushing” the nerve with a hemostat to cause a second-degree nerve injury. (C) Wallerian degeneration occurs distal to the site of compression. (D) Axons regenerate from the level of the crush injury, with some axons following the donor nerve and restoring function to the upper trapezius muscle, and some axons diverting into the distal recipient nerve via the LABC graft.
- •
The upper trunk is identified between the anterior and middle scalene muscles.
- •
The suprascapular nerve is a distinct branch of the upper trunk that sits on the superolateral aspect.
- •
The spinal accessory nerve is located in the posterior aspect of the incision on the deep surface of the trapezius muscle.
- •
Although an end-to-end transfer can be performed, the end-to-side approach with a partial neurectomy of the donor accessory nerve is preferred, as this preserves some donor function.
- •
In the end-to-side transfer, a short interpositional graft from the recipient suprascapular nerve to the donor spinal accessory nerve is required to avoid tension.
- •
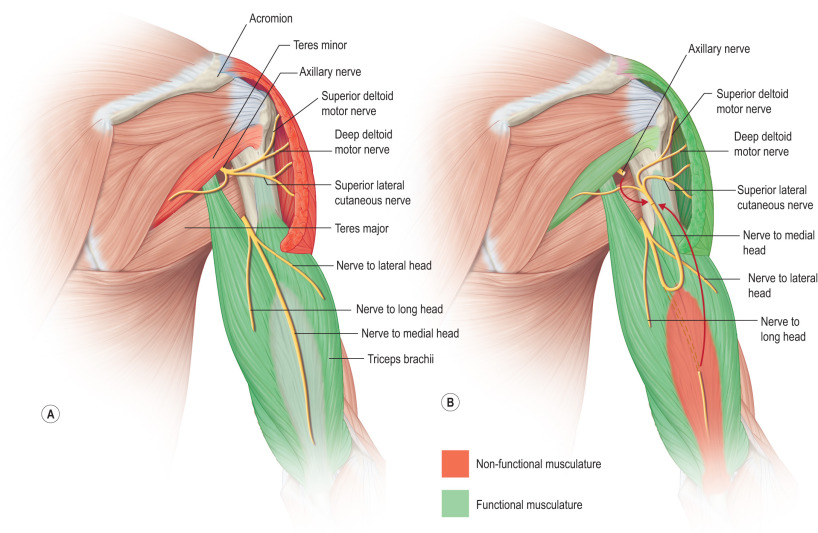
Use of triceps to axillary nerve transfer (motor component)
- ■
Additional reduction of glenohumeral subluxation and abduction of the shoulder are provided by transferring a branch of the triceps, usually from the medial head, to the axillary nerve ( Fig. 25.5 ) .