Synopsis
Open rhino
- ■
Accurate preoperative analysis and clinical diagnosis set the foundation for successful primary open rhinoplasty.
- ■
Open rhinoplasty allows anatomic exposure, identification, and correction of nasal deformities.
- ■
Component dorsal hump reduction allows accurate and incremental reduction of the nasal dorsum while preventing problems with internal valve collapse or dorsal irregularities.
- ■
Nasal tip suturing techniques allow control of definition without damaging the osseocartilaginous framework and compromising support.
- ■
Knowledge of the normal course of recovery and potential complications is key to managing patient expectations in the postoperative period.
Closed rhino
- ■
Nature is predictable – therefore, nasal phenomenology can be understood.
- ■
Rhinoplasty has consistent “behavioral” rules, like all surgery – therefore, the surgeon can control the result.
- ■
Nasal deformities are not limitless or lawless but follow patterns – therefore, their solutions follow patterns.
- ■
Sequential intraoperative photography teaches nasal behavior and structural interactions.
- ■
Follow the technical rules that apply to all other surgery: limit dissection, morbidity, and tension on closure.
- ■
Reconstruct anatomically.
- ■
Never forget function.
- ■
Never forget the patient’s own aesthetic.
- ■
Remember that most problems are under the surgeon’s control.
- ■
Always follow your patients closely.
Keywords
Rhinoplasty, Nose job, Dorsal Hump, Cartilages, Deformity, Open, Closed
Synopsis
Open rhino
- ■
Accurate preoperative analysis and clinical diagnosis set the foundation for successful primary open rhinoplasty.
- ■
Open rhinoplasty allows anatomic exposure, identification, and correction of nasal deformities.
- ■
Component dorsal hump reduction allows accurate and incremental reduction of the nasal dorsum while preventing problems with internal valve collapse or dorsal irregularities.
- ■
Nasal tip suturing techniques allow control of definition without damaging the osseocartilaginous framework and compromising support.
- ■
Knowledge of the normal course of recovery and potential complications is key to managing patient expectations in the postoperative period.
Closed rhino
- ■
Nature is predictable – therefore, nasal phenomenology can be understood.
- ■
Rhinoplasty has consistent “behavioral” rules, like all surgery – therefore, the surgeon can control the result.
- ■
Nasal deformities are not limitless or lawless but follow patterns – therefore, their solutions follow patterns.
- ■
Sequential intraoperative photography teaches nasal behavior and structural interactions.
- ■
Follow the technical rules that apply to all other surgery: limit dissection, morbidity, and tension on closure.
- ■
Reconstruct anatomically.
- ■
Never forget function.
- ■
Never forget the patient’s own aesthetic.
- ■
Remember that most problems are under the surgeon’s control.
- ■
Always follow your patients closely.
Synopsis
Open rhino
- ■
Accurate preoperative analysis and clinical diagnosis set the foundation for successful primary open rhinoplasty.
- ■
Open rhinoplasty allows anatomic exposure, identification, and correction of nasal deformities.
- ■
Component dorsal hump reduction allows accurate and incremental reduction of the nasal dorsum while preventing problems with internal valve collapse or dorsal irregularities.
- ■
Nasal tip suturing techniques allow control of definition without damaging the osseocartilaginous framework and compromising support.
- ■
Knowledge of the normal course of recovery and potential complications is key to managing patient expectations in the postoperative period.
Closed rhino
- ■
Nature is predictable – therefore, nasal phenomenology can be understood.
- ■
Rhinoplasty has consistent “behavioral” rules, like all surgery – therefore, the surgeon can control the result.
- ■
Nasal deformities are not limitless or lawless but follow patterns – therefore, their solutions follow patterns.
- ■
Sequential intraoperative photography teaches nasal behavior and structural interactions.
- ■
Follow the technical rules that apply to all other surgery: limit dissection, morbidity, and tension on closure.
- ■
Reconstruct anatomically.
- ■
Never forget function.
- ■
Never forget the patient’s own aesthetic.
- ■
Remember that most problems are under the surgeon’s control.
- ■
Always follow your patients closely.
Brief introduction
- ■
Regardless of your preferred technique, a thorough knowledge of nasal anatomy and understanding of nasal airflow and physiology are the foundations for successful aesthetic and functional rhinoplasty.
- ■
Proponents of open rhinoplasty argue that closed rhinoplasty is difficult because the surgeon does not have good binocular vision through small incisions, the dissection is blind, the anatomy is complex, and the operation is technically difficult.
- ■
Proponents of endonasal or closed rhinoplasty techniques point to two common considerations:
- •
First, by separating columellar skin from the medial crura, the surgeon loses an important component of tip stability and projection, which therefore requires some method (suture fixation or columellar strut) to support the medial crura so that a new nasal tip can be made. The strut can impart rigidity to the columella and increases graft requirements.
- •
In primary patients, this consideration may be unimportant, but in secondary patients whose donor sites are already depleted, every bit of graft material counts.
- •
Though incisions are limited, endonasal rhinoplasty is not a blind operation. Most procedures are performed under direct vision with greater access than endoscopic surgery permits.
- •
The operative strategy, making skeletal changes through limited incisions and judging progress by feeling the surface, is precisely the same discipline required by suction-assisted lipectomy.
- •
Limited pocket dissection minimizes the need for graft fixation and simplifies some procedures.
- •
Solid or crushed grafts can be used in ways that would be tedious or impossible by the open approach, although some solutions have been described.
- •
- ■
In rhinoplasty, there are four common anatomic variants that predispose to unfavorable results:
- ■
Low radix or low dorsum:
- •
Low radix or low dorsum begins caudal to the level of the upper lash margin with the patient’s eyes in primary gaze.
- •
The low radix is one of several primary causes of nasal imbalance: an upper nose that seems too small for its lower nasal component.
- •
When the radix begins lower than the upper lash margin, dorsal length is therefore shorter, and so nasal base size appears larger.
- •
If the surgeon reduces the nasal dorsum, the patient’s preoperative skeletal and skin sleeve maldistribution will worsen, and the lower nose will appear even larger.
- •
The surgeon should instead either limit tip reduction or raise the dorsum segmentally or entirely to balance the nasal base.
- •
- ■
A narrow middle vault:
- •
Arbitrarily defined as any upper cartilaginous vault that is at least 25% narrower than the upper or lower nasal third. This variant is a trait that places the patient at special risk for internal valvular obstruction, which can exist preoperatively or may be produced by dorsal resection.
- •
Inadequate tip projection is defined as any tip that does not project to the level of the anterior septal angle.
- •
Alar cartilages sufficiently strong to support the tip to the level of the septal angle are “adequately projecting”; alar cartilages too weak to do so are “inadequately projecting”.
- •
The practical value of this definition lies in its ability to define treatment: adequately projecting tips do not need increased support, whereas inadequately projecting tips do.
- •
“Alar cartilage malposition” describes cephalically rotated lateral crura whose long axes run on an axis toward the medial canthi instead of toward the lateral canthi, the position of orthotopic lateral crura.
- •
This anatomic variation was first recognized by Sheen as an aesthetic deformity that produced a round or boxy tip lobule with characteristic “parentheses” on frontal view.
- •
Malposition also has two additional ramifications that are not aesthetic:
- •
First, the abnormal cephalic position of the lateral crura places them at special risk if an intercartilaginous incision is made at its normal intranasal location.
- •
Second, most malpositioned lateral crura do not provide adequate external valvular support, and so malposition is not only associated with boxy or ball tips but also the leading cause of external valvular incompetence.
- •
None of these four anatomical variants (low radix or low dorsum, narrow middle vault, inadequate tip projection, and alar cartilage malposition) always require treatment, but they do supply cautionary notes.
- •
The most common grouping in both primary and secondary patients was the triad of low radix, narrow middle vault, and inadequate tip projection.
- •
The second most common grouping was the association of all four anatomic traits.
- •
- ■
For many years, the following concepts provided the basis for analysis of the obstructed nose:
- •
The bony and cartilaginous septal partition, deformed by congenital or traumatic causes, may obstruct the nasal airway.
- •
Compensatory hypertrophy of the contralateral inferior turbinate frequently occurs so that both airways eventually become obstructed.
- •
- ■
These concepts are more understandable if the reader considers airway size to be the product of at least four factors: (1) mucosal sensitivity to the environment or hereditary factors, (2) inferior turbinate hypertrophy from many causes, (3) septal deviation, and (4) position and stability of the lateral nasal wall during the dynamic process of ventilation.
Preoperative considerations
- ■
Obtain information on the patient’s medical and emotional suitability to undergo rhinoplasty.
- ■
Feelings of inadequacy, immaturity, family conflicts, divorce, and other major life changes may be unhealthy motivating factors behind the patient seeking aesthetic surgery.
- ■
Poor postoperative patient satisfaction is often based on emotional dissatisfaction as opposed to technical failure, and this can be avoided by the preoperative identification of these unhealthy motivating factors.
- ■
Review past medical history and specifically note a history of allergic disorders, including hay fever, asthma, and other problems, including vasomotor rhinitis and sinusitis. These conditions should be controlled prior to rhinoplasty; however, patients should be informed that they may be exacerbated in the postoperative period and can persist for weeks to months.
- ■
Nasal obstruction is usually found in patients with a long history of allergic rhinitis secondary to inferior turbinate hypertrophy. Engorgement of the inferior turbinates causes these symptoms to be worse at night. Patients may also complain of headache because of the inadequacy of the inferior turbinate to warm inspired air.
- ■
Prior nasal trauma and surgeries, including rhinoplasty, septal reconstruction/septoplasty, and sinus surgery, should be noted.
- ■
Smoking, alcohol consumption, and use of illicit drugs, in particular cocaine, can compromise outcomes. Medications including acetylsalicylic acid, nonsteroidal anti-inflammatory drugs, fish oil, and certain herbal supplements may cause increased risk of bleeding and postoperative ecchymosis.
- ■
Anatomic examination includes both external nasal analysis ( Table 4.1 ) and internal nasal examination ( Table 4.2 ). In addition, facial analysis plays a key role in achieving facial harmony after rhinoplasty.
Table 4.1
External nasal analysis
Frontal view
Facial proportions
Skin type/quality
Fitzpatrick type, thin or thick, sebaceous
Symmetry and nasal deviation
Midline, C-, reverse C-, S- or S-shaped deviation
Bony vault
Narrow or wide, asymmetrical, short or long nasal bones
Midvault
Narrow or wide, collapse, inverted-V deformity
Dorsal aesthetic lines
Straight, symmetrical or asymmetrical, well- or ill-defined, narrow or wide
Nasal tip
Ideal/bulbous/boxy/pinched, supratip, tip-defining points, infratip lobule
Alar rims
Gull-shaped, facets, notching, retraction
Alar base
Width
Upper lip
Long or short, dynamic depressor septi muscles, upper lip crease
Lateral view
Nasofrontal angle
Acute or obtuse, high or low radix
Nasal length
Long or short
Dorsum
Smooth, hump, scooped out
Supratip
Break, fullness, poly beak
Tip projection
Over- or underprojected
Tip rotation
Over- or underrotated
Alar–columellar relationship
Hanging or retracted alae, hanging or retracted columella
Periapical hypoplasia
Maxillary or soft tissue deficiency
Lip–chin relationship
Normal, deficient
Basal view
Nasal projection
Over- or underprojected, columellar–lobular ratio
Nostril
Symmetrical or asymmetrical, long or short
Columella
Septal tilt, flaring of medial crura
Alar base
Width
Alar flaring
Table 4.2
Internal nasal exam
External valve
Collapse
Internal valve
Narrowing, collapse
Mucosa
Edema, irritation
Inferior turbinates
Hypertrophy
Septum
Deviation, tilt, spurs, perforation, cartilage
Masses
Polyps, tumors
- ■
Standardized photography is obtained for every patient presenting for rhinoplasty and includes frontal, lateral, oblique, and basal views of the patient.
- ■
It is useful to review photographs with the patient to identify areas of concern that can be addressed with surgery and deformities that may persist after surgery, including notches, grooves, and irregularities. Facial disproportions and asymmetries should be pointed out to the patient as these may require orthognathic surgery to address.
- ■
Identifying the patient’s expectations preoperatively is a key component to postoperative patient satisfaction and successful rhinoplasty.
- ■
Common concerns include asymmetry, tip deformities, dorsum irregularities, and nasal airway obstruction.
- ■
The patient should attempt to rank these concerns in order of importance.
- ■
A patient who focuses on minor or uncorrectable problems or who has unrealistic expectations despite extensive discussion will likely be disappointed following surgery regardless of the aesthetic improvement; it is better to avoid operating on these patients.
- ■
In general, the ideal candidate for surgery has legitimate concerns and realistic expectations and is secure and well-informed and understands the limitations of surgery.
- ■
The acronym SYLVIA has been used to describe the ideal patient: secure, young, listens, verbal, intelligent, and attractive.
- ■
The poor candidate for surgery has excessive concerns about minimal deformities and unrealistic expectations, and is insecure, poorly informed, and fails to recognize the limitations of surgery. These patients are likely to be unsatisfied following surgery regardless of the aesthetic improvement. They should be approached with caution and, in most cases, should not be operated on.
- ■
The acronym SIMON has been used to describe this patient: single, immature, male, overly expectant, and has narcissistic traits.
- ■
Proper identification of causative factors of nasal airway obstruction is key to successful treatment. Nasal airway obstruction can have both medically and surgically correctable causes.
- ■
Common surgically correctable causes include nasoseptal deviation, internal or external valve dysfunction, and inferior turbinate hypertrophy.
- ■
Primary and secondary rhinoplasty patients differ in three characteristic ways.
- •
First, the secondary patient’s scarred, contracted soft tissues will not tolerate aggressive dissection, multiple incisions, or tight dressings.
- •
Second, graft donor sites may have already been harvested, necessitating the use of more difficult (distorted septum or concha), painful (costal), or frightening (calvarial) donor sources.
- •
Third, the secondary rhinoplasty patient’s morale is often more fragile. Having already invested money, time, discomfort, and emotion in one or more unsuccessful procedures, what secondary rhinoplasty patients fear most and need least are additional disappointments.
- •
- ■
For secondary rhinoplasty patients, the surgeon should be careful to construct a plan that is based on a clear understanding of what is possible and founded on sound surgical and biologic principles that maximize the airway and respect the patient’s aesthetic goals.
- ■
Before agreeing to operate on a patient, the surgeon must be able to answer each of the following questions affirmatively:
- •
Can I see the deformity? This question eliminates delusional patients or those with minimal defects that may not be surgically correctable.
- •
Can I personally fix it? This criterion will vary from surgeon to surgeon and must be based on operative experience and ease in correcting specific problems.
- •
Can I manage the patient? A patient who is unacceptably nervous, impossible to examine, or unwilling to comply with preoperative and postoperative instructions is a poor candidate, even if all other conditions are met.
- •
If there is a complication, will the patient remain controlled and cooperate with treatment? No patient enjoys a complication, but there are those who, although disappointed, quietly understand and will await the proper time for revision. There are others who become hysterical, angry, disruptive, or accusatory and want an immediate correction.
- •
Does the patient accept the margin of error inherent in surgery? This is the most important criterion. The patient’s willingness to accept the imperfection that is inherent in surgery is a willingness to accept the imperfection that is inherent in being human.
- •
Anatomical pearls
- ■
It is helpful to conceptualize the nose as a system of two interrelated layers ( Fig. 4.1 ) .
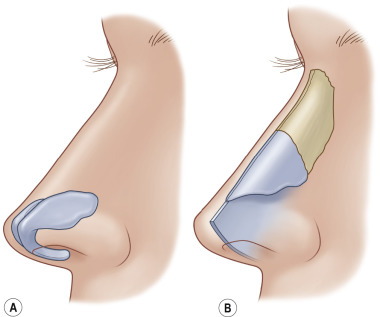
Figure 4.1
The structural layers of the nose, which separate those anatomical units that move together. The investing soft tissues and alar cartilages (A) glide over the inner, fixed, semirigid layer, which contains the bony vault, the upper cartilaginous vault, and the nasal septum (B) .
- ■
The outer layer, like a soft, elastic sleeve, slides over the inner semirigid layer and contains the entire investing nasal soft tissues plus the alar cartilages and their associated lining.
- ■
The inner layer contains everything else (the bony and upper cartilaginous vaults, the nasal septum, and their associated linings).
- ■
This two-layer concept associates those structures that behave together anatomically and functionally, and provides an explanation for the “global” manifestations of some surgical changes (e.g., the effect of dorsal reduction or augmentation on nasal length).
- ■
The internal nasal valve is formed by the articulation of the caudal and anterior (or dorsal) edges of the upper lateral cartilages with the anterior septal edge ( Fig. 4.2 ) .
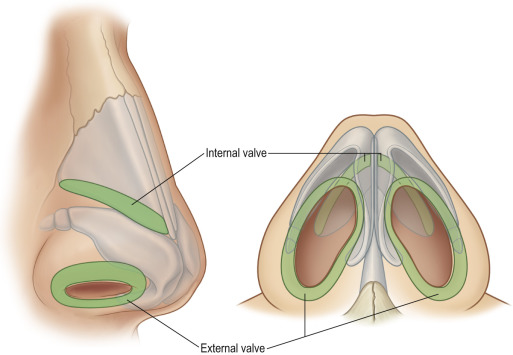
Figure 4.2
The nasal valves. The internal valves are formed by the articulation of the upper lateral cartilages with the anterior (dorsal) septal edge; the external valves are formed by the alar cartilage lateral crura and their associated investing soft tissue cover.
- ■
The external nasal valve is composed of the cutaneous and skeletal support of the mobile alar wall (the alar cartilage lateral crura with their associated external and vestibular skin coverings).
Upper cartilaginous vaults
- ■
The width and stability of the upper cartilaginous vault (formed by the upper lateral cartilages and the anterior septal edge), the critical area of the internal nasal valves, depend not only on the width of the bony vault but also on the height and width of the middle vault roof.
- ■
Resection of the middle vault roof during hump reduction removes this most critical anterior stabilizing force on the upper lateral cartilages, which will fall medially and produce a characteristic “inverted-V” deformity and consequent narrowing at the internal valves.
- ■
Middle vault collapse virtually always occurs when the cartilaginous roof has been resected, whether or not osteotomy has been performed, but may not be visible if the overlying soft tissues are sufficiently thick.
- ■
To avoid middle vault collapse and internal valvular incompetence, the surgeon should plan to reconstruct the normal distracting forces by a substantial dorsal graft or by spreader grafts, which provide the same degree of functional mean nasal airflow improvement (see below).
Middle and lower cartilaginous vaults
- ■
The upper lateral cartilages are supported caudally by their relationship to the cephalic margins of the lateral crura in the region of the so-called “scroll”.
- ■
Radical alar cartilage resection can compromise middle vault support and may leave an external deformity typified by deepening and lengthening of the alar creases.
- ■
Resect the upper lateral cartilages submucosally only when failure to do so would allow them to prolapse into the airway or when necessary to shorten the nose.
- ■
The point of intersection of the upper and lower lateral cartilages creates the “watershed” area between the internal and external nasal valves, and aggressive surgery in this area also affects external valvular competence, particularly in patients whose alar cartilage lateral crura are cephalically rotated.
Dorsum and tip
- ■
Tip projection, that is, the intrinsic ability of the alar cartilages to support the tip lobule independent of dorsal height, depends on alar cartilage middle crural size, shape, and substance.
- ■
Septal deviation can involve deviation of the septal cartilage, perpendicular plate of the ethmoid bone, or vomer away from the midline and can cause obstruction of one or both of the nasal airways, along with external deviation of the nose.
- ■
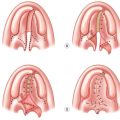
Nasal deviations can generally be classified into three basic types: (1) caudal septal deviations, (2) concave dorsal deformities, and (3) concave/convex dorsal deformities ( Table 4.3 ).
Table 4.3
Classification of nasal deviations
- I.
Caudal septal deviation
- a.
Straight septal tilt
- b.
Concave deformity (C-shaped)
- c.
S-shaped deformity
- a.
- II.
Concave dorsal deformity
- a.
C-shaped dorsal deformity
- b.
Reverse C-shaped dorsal deformity
- a.
- III.
Concave/convex dorsal deformity (S-shaped)
- I.
- ■
Septal tilt is the most common type where the quadrangular cartilage and perpendicular plate of the ethmoid are straight, but the quadrangular cartilage is tilted to one side internally and to the opposite side externally. Hypertrophy of the inferior turbinate contralateral to the side of internal deviation is usually present.
- ■
The turbinates exist as three or four bilateral extensions from the lateral nasal cavity.
- ■
The inferior turbinate consists of highly vascular mucoperiosteum covering a thin semicircular conchal bone and is involved in regulation of filtration and humidification of inspired air.
- ■
In combination with the internal nasal valve, the anterior extent of the inferior turbinate can be responsible for up to two-thirds of the upper-airway resistance.
- ■
Inferior turbinoplasty is performed in patients with nasal airway obstruction secondary to inferior turbinate hypertrophy refractory to medical management.
- ■
Overly aggressive surgical management may be complicated by bleeding, mucosal crusting and desiccation, ciliary dysfunction, chronic infection, malodorous nasal drainage, or atrophic rhinitis.
- ■
In most cases, inferior turbinoplasty with outfracture of the inferior turbinate or submucous resection is adequate to achieve significant improvement ( Fig. 4.3 ) .
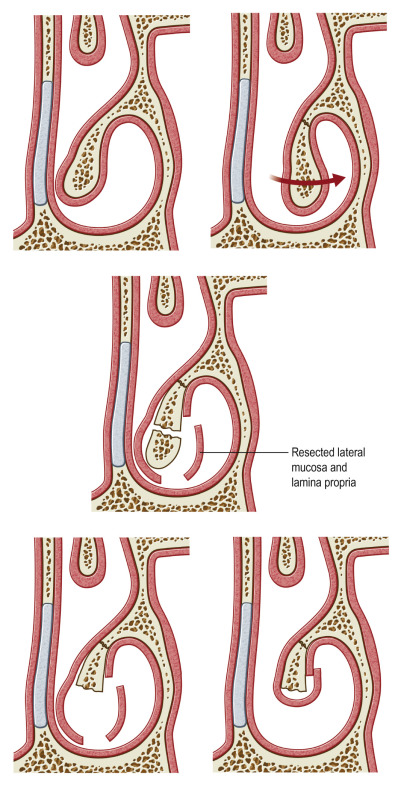
Figure 4.3
Inferior turbinate outfracture and submucous resection.
- ■
In cases of severe inferior turbinate hypertrophy, submucous resection of the inferior turbinate is indicated.
- ■
Autologous grafts are preferential to homografts and alloplastic implants because of their high biocompatibility and low risk of infection and extrusion.
- ■
Disadvantages include donor site morbidity, graft resorption, and unavailability of sufficient quantities of graft material.
- ■
Grafts are most commonly obtained from septal, ear, and costal cartilage. Other sites include calvarial, nasal bone, and the olecranon process of the ulna.
- ■
Concerns regarding donor site morbidity, graft availability, and graft resorption will necessitate the use of homologous or alloplastic implants.
- ■
Septal cartilage is the primary choice for autogenous grafts in rhinoplasty. It can be used in all areas including tip grafts, dorsal onlay grafts, columellar strut grafts, and nasal spreader grafts. It is easily harvested, leaves minimal donor site morbidity, and is available in the operative field.
- ■
The ear can provide a significant amount of cartilage for rhinoplasty when septal cartilage has been depleted. It can be used for tip grafts, dorsal onlay grafts, alar contour grafts, and reconstruction of the lower lateral cartilages. However, its flaccidity does not allow it to be used where structural support is necessary. Donor site morbidity and scarring are minimal.
- ■
Costal cartilage provides abundant autogenous graft material. It can be used for tip grafts, columellar strut grafts, nasal spreader grafts, alar cartilage grafts, and dorsal onlay grafts. Given the size, amount, and intrinsic qualities, costal cartilage lends itself well to use as a dorsal onlay graft and where structural support is required.
- ■
It can be carved into any shape. However, allowing at least 30 min to pass prior to carving allows initial warping to occur, minimizing late deformity.
- ■
The straightest, smoothest cartilage graft is used for the nasal dorsum to reconstruct this dominant area covered by thin soft tissues.
- ■
If septum is available, it is used. Failing that, use rib cartilage for the dorsum.
- ■
Bone that may be unsuitable elsewhere can be used instead for spreader grafts, lateral wall grafts, or alar wall grafts. And primarily in closed techniques, solid or lightly crushed cartilage scraps can fill regional depressions.
- ■
The key principle in all augmentation is to match the graft material to the patient’s soft tissue characteristics and to his or her aesthetic goals.
- ■
Unmodified rib cartilage is stiff, ear cartilage is rubbery, and septal cartilage is the most “plastic”.
- ■
Thicker skin needs more augmentation to provide a given result but will hide more underlying flaws.
- ■
Thinner skin requires softer, well-contoured grafts that will not show excessively.
- ■
A graduated approach to nasal tip surgery requires a combination of techniques including the cephalic trim, the use of a columellar strut graft, nasal tip suturing, and nasal tip grafting.
- ■
Compared with the closed approach, the open approach may cause mild loss of tip projection due to disruption of ligamentous support and increased skin undermining. As such, columellar strut graft and nasal tip suturing techniques are often employed to maintain nasal tip support during open rhinoplasty.
- ■
Nasal tip grafts are used in primary rhinoplasty only if adequate tip projection, definition, or symmetry cannot be obtained by the use of the previously discussed techniques. Visible nasal tip grafts are used infrequently in primary rhinoplasty because of the potential for long-term resorption leading to asymmetries or sharp angulations requiring revision.
- ■
Tip suturing techniques ( Table 4.4 ) are used to refine the tip by controlling the subtle contours of the lower lateral cartilages.
Table 4.4
Tip-suturing techniques
Medial crural suture
Interdomal suture
Transdomal suture
Joined transdomal suture
Intercrural septal suture
Lateral crural mattress suture
- ■
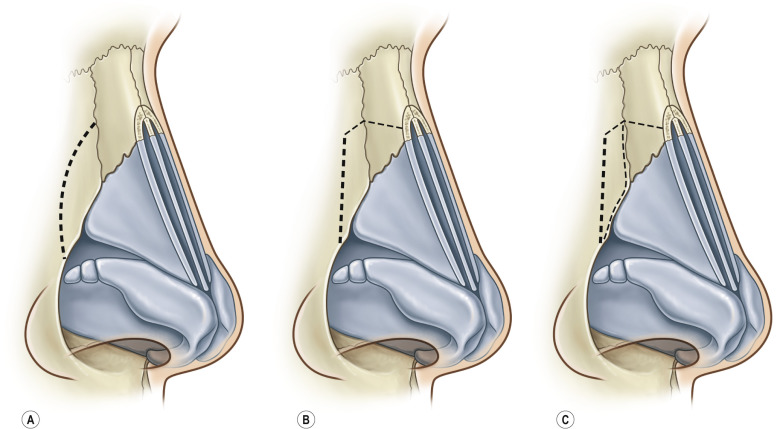
When nasal tip grafts are used, it is important that they have smooth, tapered edges. Nasal tip grafts of all shapes and sizes have been described ( Fig. 4.4 ) .
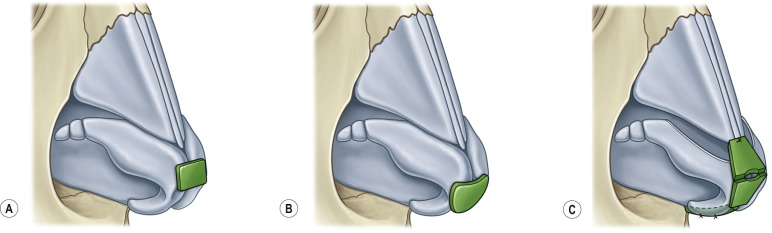
Figure 4.4
Nasal tip cartilage grafts. (A) Supratip; (B) infratip; (C) anatomic.
- ■
The presence of deformities of the alar rims such as alar notching or retraction, facets of the soft tissue triangles, malposition of the lateral crura, or functional problems including external valve collapse may require the use of lateral crural horizontal mattress sutures, lower lateral crural turnover flaps, or alar contour or lateral crural strut grafts to correct.
- ■
Nasal osteotomies are a key component to shape the bony vault in rhinoplasty. They are used to narrow a wide bony vault, close an open-roof deformity, or straighten deviated nasal bones.
- ■
The goals of nasal osteotomies are maintenance or creation of smooth dorsal aesthetic lines and obtaining a desirable width of the bony vault.
- ■
Osteotomies can be classified by approach (external or internal), type (lateral, medial, transverse, or a combination), and level (low to high, low to low, or double level) ( Fig. 4.5 ) .