Synopsis
- ▪
The teachings of John Converse, Nicholas Georgiade, and Reed Dingman provided the benchmark for an entire generation of surgeons in facial injury repair.
- ▪
The treatment concepts discussed in this chapter were developed at the University of Maryland Shock Trauma Unit and ultimately employed at the International Center for Facial Injury Reconstruction at Johns Hopkins.
- ▪
The proportion of severe injuries seen at these centers is high.
- ▪
The treatment concepts, however, may be modified for common fractures and less significant injuries.
- ▪
Greater emphasis has been placed on minimizing operative techniques and limited exposures, whereas the decade of the 1980s witnessed craniofacial principles of broad exposure and fixation at all buttresses for a particular fracture across all degrees of severity.
- ▪
Presently, the treatment of injuries is organized both by severity and anatomic area to permit the smallest exposure possible to achieve a good result [computerized tomographic (CT)–based facial fracture treatment].
Keywords
Face, Injury, Fracture, Laceration, Frontal, Sinus
Synopsis
- ▪
The teachings of John Converse, Nicholas Georgiade, and Reed Dingman provided the benchmark for an entire generation of surgeons in facial injury repair.
- ▪
The treatment concepts discussed in this chapter were developed at the University of Maryland Shock Trauma Unit and ultimately employed at the International Center for Facial Injury Reconstruction at Johns Hopkins.
- ▪
The proportion of severe injuries seen at these centers is high.
- ▪
The treatment concepts, however, may be modified for common fractures and less significant injuries.
- ▪
Greater emphasis has been placed on minimizing operative techniques and limited exposures, whereas the decade of the 1980s witnessed craniofacial principles of broad exposure and fixation at all buttresses for a particular fracture across all degrees of severity.
- ▪
Presently, the treatment of injuries is organized both by severity and anatomic area to permit the smallest exposure possible to achieve a good result [computerized tomographic (CT)–based facial fracture treatment].
Brief introduction
- ▪
Bone and soft tissue injuries in the facial area should be managed as soon as the patient’s general condition permits.
- ▪
Classically, facial soft tissue and bone injuries are not acute surgical emergencies, but both the ease of obtaining a good result and the quality of the result are better with early or immediate management.
- ▪
Less soft tissue stripping is required, bones are often easily replaced into their anatomic position, and easier fracture repairs are performed.
- ▪
The definitive radiographic evaluation is the craniofacial CT scan with axial, coronal, and sagittal sections of bone and soft tissue windows. However, the clinical examination remains the most sensitive detection of the character and functional implications of the facial injury.
- ▪
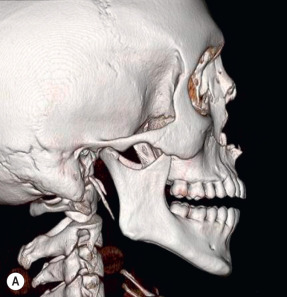
Access to the craniofacial skeleton can be achieved through strategic incision placement ( Fig. 9.1 ) .
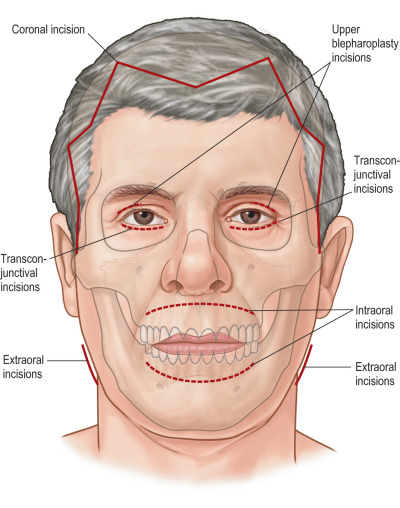
Figure 9.1
Cutaneous incisions (solid line) available for open reduction and internal fixation of facial fractures. The conjunctival approach (dotted line) also gives access to the orbital floor and anterior aspect of the maxilla, and exposure may be extended by a lateral canthotomy. Intraoral incisions (dotted line) are also indicated for the Le Fort 1 level of the maxilla and the anterior mandible. The lateral limb of an upper blepharoplasty incision is preferred for isolated zygomaticofrontal suture exposure if a coronal incision is not used. A horizontal incision directly across the nasal radix is the one case in which a local incision can be tolerated over the nose. In many instances, a coronal incision is preferable unless the hair is short or the patient is balding.
Preoperative considerations
- ▪
Management begins with an initial physical examination and is followed by a radiologic evaluation accomplished with CT scanning ( Table 9.1 ).
Table 9.1
Key components of initial evaluation
- I.
ABCs
- II.
History
- 1.
Mechanism of injury (was the patient restrained, mobile, stationary)?
- 2.
Time of injury (i.e., how much time has elapsed since injury)?
- 3.
Penetrating vs. blunt injury?
- 4.
What type of object involved (e.g., fist, bat, windshield, etc.)?
- 5.
Does the patient complain of any symptoms to particular facial area (e.g., numbness, pain)?
- 6.
How does it feel when the patient bites down – pain? Do teeth feel “normal”? Does bite “feel normal”?
- 7.
Does the patient complain of visual problems, nasal problems, hearing problems, or abnormal/painful bite?
- 8.
Any significant PMH, meds, allergies, social history (e.g., diabetes, aspirin, coumadin, steroid use, ETOH, etc.)?
- 1.
- III.
Exam
- 1.
Inspect face/head for asymmetry, lacerations, abrasions, hematomas, ecchymoses (especially periorbital), epistaxis.
- 2.
Document any bony irregularities, enophthalmos, proptosis, telecanthus.
- 3.
Document visual acuity (e.g., Can you read my ID badge from 12 inches away?).
- 4.
Check pupils and ocular muscles.
- a.
Is there a hyphema (blood in the anterior chamber)?
- b.
Are extraocular movements intact, or is there a restriction in gaze?
- c.
Are pupils reactive and equal?
- a.
- 5.
Inspect oral cavity – pay particular attention to dentition, occlusion, lacerations.
- 6.
Palpate the facial bones and soft tissue: document bony step-offs, crepitance, mobile segments, significant pain, and numbness.
- a.
Palpate orbital rims.
- b.
Palpate radix and nasal bridge for instability, crepitance.
- c.
Check for integrity/mobility of medial canthus.
- d.
Palpate zygoma/zygomatic arch.
- e.
Palpate frontal bone, maxilla/maxillary sinus, cranium.
- f.
Palpate temporomandibular joint at rest and through mandible range of motion.
- g.
Palpate mandible along its length.
- h.
Using gloved hand, palpate teeth for instability, fractures, etc.
- i.
Using gloved hand, grab maxilla/alveolus and check for midface instability/pain.
- j.
Inspect nasal passages and external auditory canal to rule out septal hematoma, CSF rhinorrhea, otorrhea.
- a.
- 7.
Perform sensory exam of all branches of trigeminal nerve (supraorbital, infraorbital, marginal mandibular).
- 8.
Perform motor exam of facial nerve – raise eyebrows, smile, grit teeth, close eyes tightly.
- 1.
- IV.
Imaging
- 1.
CT face/orbits (1.5- to 3-mm cuts along facial bones with coronal/sagittal/axial reconstructions)
- 2.
CT C-spine (overall, 2%–4% incidence of C-spine injury with facial fractures)
- 3.
Sometimes a panorex is warranted. (Often study of choice for mandible fracture, can miss symphyseal fractures – requires normal C-spine)
- 1.
- V.
Adjuncts
- 1.
Ophthalmology consult – if any sign/concern for ocular injury/visual disturbance.
- 1.
- I.
- ▪
Bone injuries are suggested by soft tissue symptoms such as contusions, abrasions, ecchymosis, edema, and distortion of the facial proportions.
Frontal bone and sinus injury patterns
Brief introduction
- ▪
The frontal sinuses are paired structures that begin to be detected at 3 years of age. Significant pneumatic expansion does not begin to occur until approximately 7 years, with full sinus development complete by the age of 18–20.
- ▪
The frontal sinuses are lined with respiratory epithelium, which consists of a ciliated membrane with mucus-secreting glands. A blanket of mucin is essential for normal function, and the cilia beat this mucin in the direction of the nasofrontal ducts.
- ▪
When injured, they serve as a focus for infection, especially if duct function is impaired.
- ▪
One-third of fractures involve the anterior table alone, and 60% involve the anterior table and posterior table and/or ducts.
- ▪
Forty percent of frontal sinus fractures have an accompanying dural laceration.
Preoperative considerations
- ▪
Lacerations, bruises, hematomas, and contusions constitute the most frequent signs of frontal bone or sinus fractures.
- ▪
Occasionally, the first presentation of a frontal sinus fracture may be an infection or symptom of frontal sinus obstruction, such as mucocele or abscess formation. Infection in the frontal sinus may produce serious complications because of its location.
- ▪
Frontal sinus fractures should be characterized by describing both the anatomic location of the fracture, including involvement of the anterior table, posterior table, or both, and their degree of displacement.
- ▪
Indications for operative management include:
- ▪
Depression of the anterior table.
- ▪
Radiographic demonstration of involvement of the nasofrontal duct with presumed future non-function.
- ▪
Obstruction of the nasofrontal duct with persistent air fluid levels.
- ▪
Mucocele formation.
- ▪
Fractures of the posterior table that are displaced and presumably have lacerated the dura resulting in a cerebrospinal fluid leak.
- ▪
While some authors recommend exploration of any posterior table fracture or any fracture in which an air fluid level is visible, most explore posterior wall fractures only if their displacement exceeds the width of the posterior table.
Anatomical pearls
- ▪
The nasofrontal duct passes through the anterior ethmoidal air cells to exit adjacent to the ethmoidal infundibulum beneath the middle meatus.
- ▪
Blockage prevents adequate drainage of normal mucous secretions and predisposes to the development of mucoceles.
- ▪
The reported average interval between the primary injury and development of frontal sinus mucocele is 7½ years.
Key technical considerations
- ▪
The best technique of exposure is the coronal incision. Occasionally, a laceration may be used.
- ▪
Any depressed frontal sinus fracture of the anterior wall potentially requires exploration and wall replacement in an anatomic position to prevent contour deformity.
- ▪
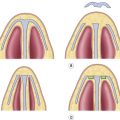
If the nasofrontal duct is compromised, obliteration of the sinus is required and commonly involves stripping of the mucosa, burring of the bone, and occlusion with well-designed “formed-to-fit” calvarial bone plugs or soft tissue ( Fig. 9.2A–C ) .
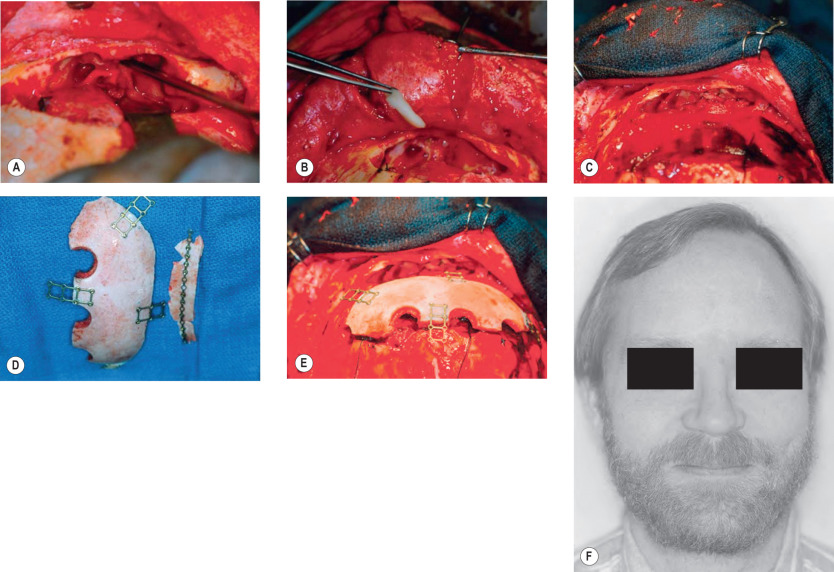
Figure 9.2
(A) Nasofrontal duct. (B) Bone plug for nasofrontal duct and galeal flap. (C) Bone obliteration of frontal sinus. (D) “Back table” surgery for bone replacement. (E) Bone reconstruction and cranialization of the frontal sinus; intracranial neurosurgery. (F) Postoperative result.
- ▪
If most of the posterior bony wall is intact, the entire frontal sinus cavity may be filled either with fat or cancellous bone.
- ▪
If the posterior table is missing, or significantly displaced, the sinus should be “cranialized”. In cranialization, the posterior wall of the frontal sinus is removed, effectively making the frontal sinus a part of the intracranial cavity. The “dead space” may be filled with cancellous bone or left open. Any communication with the nose by the nasofrontal duct or with the ethmoid sinuses should be sealed.
- ▪
A galeal flap with a pedicle of the superficial temporal artery can be a useful method for vascularized soft tissue obliteration of frontal bone problems.
Outcomes and complications
- ▪
Complications of frontal bone and sinus fractures include:
- •
Cerebrospinal fluid (CSF) fluid rhinorrhea.
- •
Pneumocephalus and orbital emphysema.
- •
Absence of orbital roof and pulsating exophthalmos.
- •
Carotid–cavernous sinus fistula.
- •
Orbital fractures
Brief introduction
- ▪
Orbital fractures may occur as isolated fractures of the internal orbit or may involve both the internal orbit and the orbital rim.
- ▪
An orbital blow-out fracture is caused by the application of a traumatic force to the rim, globe, or soft tissues of the orbit accompanied by sudden increase in intraorbital pressure and subsequent fracture through the orbital floor ( Fig. 9.3 ) .
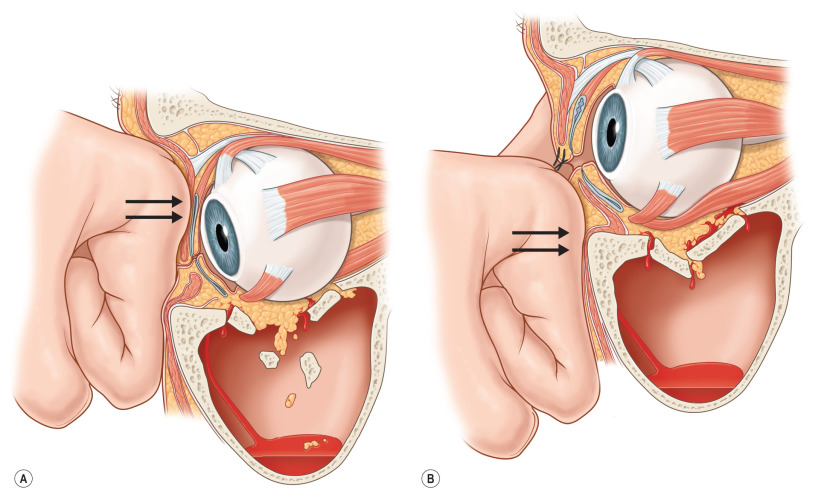
Figure 9.3
(A) Mechanism of blow-out fracture from displacement of the globe itself into the orbital walls. The globe is displaced posteriorly, striking the orbital walls and forcing them outward, causing a “punched out” fracture the size of the globe. (B) “Force transmission” fracture of orbital floor.
- ▪
In children, the mechanism is more frequently like that of a trapdoor, rather than the “blow-out” fracture seen in adults ( Fig. 9.4 ) .

Figure 9.4
Blow-out fracture in a child produced by a snowball. Note the nearly complete immobility of the ocular globe and the enophthalmos. Such severe loss of motion implies actual muscle incarceration, an injury that is more frequent in children than in adults. This fracture deserves immediate operation with release of the incarcerated extraocular muscle system. It is often accompanied by pain on attempted rotation of the globe and sometimes nausea and vomiting. These symptoms are unusual in orbital floor fractures without true muscle incarceration.
- ▪
As opposed to incarceration of fat adjacent to the inferior rectus muscle, children more frequently “scissor” or capture the muscle directly in the fracture site.
- ▪
Muscle incarceration is an urgent situation that demands immediate release of the incarcerated muscle.
- ▪
The patient with true muscle entrapment may experience pain on attempted eye motion as well as nausea, vomiting, and an oculocardiac reflex (nausea, bradycardia, and hypotension).
- ▪
The purpose of orbital floor reconstruction/replacement in this scenario, whether a bone graft or an inorganic implant, is to re-establish the size and the shape of the orbital cavity. This replaces the orbital soft tissue contents and allows scar tissue to form in an anatomic position.
- ▪
A forced duction test is performed by grasping the orbital conjunctiva with forceps and testing the range of motion of the globe ( Fig. 9.5 ) .
- •
Limitation of forced rotation or motion is a positive test for entrapment of extraocular muscles. This test should be performed:
- •
Before dissection.
- •
After dissection.
- •
After the insertion of each material used to reconstruct the orbital wall.
- •
Just prior to closure of the incisions.

Figure 9.5
The forced duction test. Clinical photograph. A drop of local anesthetic instilled into the conjunctival sac precedes the procedure.
- •
Preoperative considerations
- ▪
Indications for surgical treatment of orbital fractures:
- ▪
Diplopia caused by incarceration of muscle or the fine ligament system, documented by forced duction examination and suggested by CT scans.
- ▪
Radiographic evidence of extensive fracture, such that enophthalmos would occur.
- ▪
Enophthalmos or exophthalmos produced by an orbital volume change.
- ▪
Visual acuity deficit, increasing and not responsive to medical dose steroids, implying that optic canal decompression would be indicated.
- ▪
“Blow-in” orbital fractures that involve the medial or lateral walls of the orbit, and severely constrict orbital volume, creating increased intraorbital pressure.
- ▪
Goals of surgical management:
- ▪
Disengage entrapped structures and restore ocular rotatory function.
- ▪
Replace orbital contents into the usual confines of the normal bony orbital cavity, including restoration of both orbital volume and shape.
- ▪
Restore orbital cavity walls, which, in effect, replaces the tissues into their proper position and dictates the shape into which the soft tissue can scar.
Anatomical pearls
- ▪
The orbits are conceptualized in thirds progressing from anterior to posterior.
- ▪
Anteriorly, the orbital rims consist of thick bone.
- ▪
The middle third of the orbit consists of thin bone, while the bone structure thickens again in the posterior third.
- ▪
The orbital bone structure is thus analogous to a “shock-absorbing” device in which the middle portion of the orbit breaks first, followed by the rim.
- ▪
The optic foramen is situated at the junction of the lateral and medial walls of the orbit posteriorly and is well above the horizontal plane of the orbital floor. The foramen is located 40–45 mm behind the inferior orbital rim.
Key technical considerations
- ▪
Exposure considerations:
- •
Endoscopic approaches through the maxillary sinus permit direct visualization and repair of the orbital floor and manipulation of the soft tissues without an eyelid incision ( Fig. 9.6 ) .
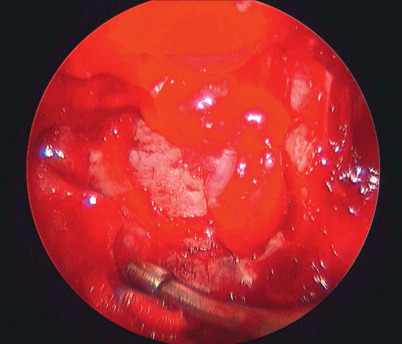
Figure 9.6
Endoscopic approach through the maxillary sinus permits direct visualization of the orbital floor and manipulation of the soft tissue and floor repair.
- •
Lower eyelid incisions have the least incidence of ectropion of any lid incision location but tend to be the most noticeable.
- •
Subciliary incisions near the upper margin of the lid leave the least conspicuous cutaneous scar, although they have the highest incidence of lid retraction.
- •
Transconjunctival incisions can be performed in the preseptal or retroseptal plane and avoid external scars. Occasionally, a lateral canthotomy or caruncular extension is necessary to widen exposure to the lateral and medial orbit, respectively.
- •
Complications and outcomes
- ▪
Diplopia: usually the result of muscle contusion, but can be the result of incarceration of muscle, soft tissue adjacent to the muscles, or nerve damage to cranial nerve III, IV, and VI.
- ▪
Enophthalmos: second major complication of blow-out fractures, usually due to enlargement of the orbital volume.
- ▪
Retrobulbar hematoma: signaled by globe proptosis, congestion, and prolapse of the edematous conjunctiva. Diagnosis is confirmed by a CT scan imaged with soft tissue windows. It is usually not possible to drain retrobulbar hematomas.
- ▪
Ocular (globe) injuries and blindness.
- ▪
Implant migration, late hemorrhage around implants, and implant fixation.
- ▪
Ptosis of the upper lid: true ptosis of the upper lid should be differentiated from “pseudoptosis” resulting from the downward displacement of the eyeball in enophthalmos.
- ▪
Scleral show, ectropion and entropion – vertical shortening of the lower eyelid.
- ▪
Infraorbital nerve anesthesia.
- ▪
The “superior orbital fissure” syndrome: when a roof fracture extends posteriorly to involve the superior orbital fissure and its contents (CN III, IV, V, VI). Signaled by: restricted gaze and numbness of the forehead, brow, medial portion of upper lid, and medial upper nose.
- ▪
The “orbital apex” syndrome: when a roof fracture extends posteriorly to involve the superior orbital fissure and optic foramen and their contents (CN II, III, IV, V, VI). Signaled by: all symptoms of the superior orbital fissure syndrome with visual acuity change or blindness.
Nasal fractures
Brief introduction
- ▪
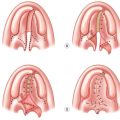
Most nasal fractures are initially reduced by closed reduction ( Fig. 9.7 ) .
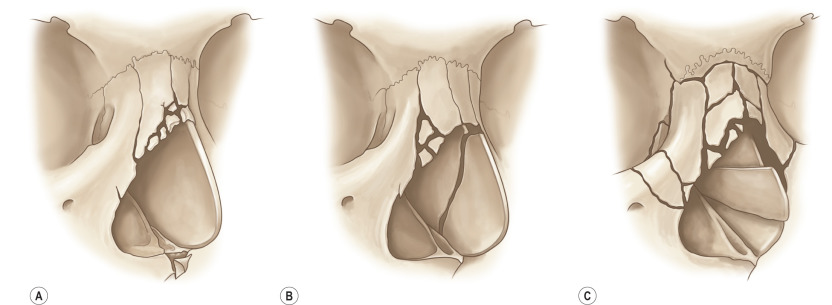
Figure 9.7
Frontal impact nasal fractures are classified by degrees of displacement, as are lateral fractures. (A) Plane I frontal impact nasal fracture. Only the distal ends of the nasal bones and the septum are injured. (B) Plane II frontal impact nasal fracture. The injury is more extensive, involving the entire distal portion of the nasal bones and the frontal process of the maxilla at the piriform aperture. The septum is comminuted and begins to lose height. (C) Plane III frontal impact nasal fractures involve one or both frontal processes of the maxilla, and the fracture extends to the frontal bone. These fractures are in reality nasoethmoidal–orbital fractures because they involve the lower two-thirds of the medial orbital rim (central fragment of the nasoethmoidal–orbital fracture) as well as the bones of the nose.
- ▪
In practice, closed reduction is frequently deferred until the edema has partially subsided, and the accuracy of the reduction may be confirmed by visual inspection and palpation.
- ▪
In more severe frontal impacts where loss of nasal height and length occurs, or in nasoethmoidal orbital fractures, the use of open reduction and primary bone or cartilage grafting is beneficial to restore the support of the nose to its original volume ( Fig. 9.8 ) .


Figure 9.8
Palpation of the (A) columella and (B) dorsum detects superior rotation of the septum and lack of dorsal support. There is an absence of columellar support and dorsal septal support.
- ▪
Naso-orbital ethmoid (NOE) fractures are severe fractures of the central one-third of the upper midfacial skeleton. They comminute the nose, the medial orbital rims, and the piriform aperture. NOE fractures are isolated in one-third of cases and, in two-thirds of cases, extend to involve the frontal bone, zygoma, or maxilla. One-third is unilateral, and two-thirds are bilateral injuries. The central feature is the displacement of the section of the medial orbital rim carrying the attachment of the medial canthal ligament.
Preoperative considerations
- ▪
The appearance of NOE fractures is typical:
- •
The nose is flattened.
- •
There is a loss of dorsal nasal prominence.
- •
An obtuse angle is noted between the lip and columella.
- •
The medial canthal areas are swollen and distorted with palpebral and subconjunctival hematoma.
- •
Directly over the medial canthal ligaments, crepitus or movement may be palpated with external pressure.
- •
Traumatic telecanthus (increase in distance between medial canthal ligaments) and/or traumatic orbital hypertelorism (increase in distance between the orbits and globe) is present.
- •
Anatomical pearls
- ▪
The diagnosis of a NOE fracture requires, at a minimum, four fractures that isolate the frontal process of the maxilla from adjacent bones:
- •
Fracture of the nose.
- •
Fracture of the junction of the frontal process of the maxilla with the frontal bone.
- •
Fracture of the medial orbit (ethmoidal area).
- •
Fracture of the inferior orbital rim extending to involve the piriform aperture and orbital floor.
- •
- ▪
NOE fractures can be classified into one of three types:
- •
Type I: an incomplete fracture, which is displaced only inferiorly at the infraorbital rim and piriform margin ( Fig. 9.9 ) .
- •