Synopsis
- ▪
Age-related changes occur in all layers of the face, including skin, superficial fat, SMAS, deep fat, and bone.
- ▪
Patients presenting for facial rejuvenation surgery are usually middle-aged or older, thus increasing the chance of co-morbidities. Risk factors such as hypertension and smoking should be dealt with prior to facelift surgery.
- ▪
Careful preoperative assessment will provide the surgeon with an aesthetic diagnosis regarding the underlying facial shape, the age-related issues that predominate, and the appropriate surgical procedures for every individual patient.
- ▪
Almost all facelift techniques begin with a subcutaneous facelift flap. Careful incision placement, tissue handling, and flap repositioning are important in order to avoid the obvious stigmata of facelift surgery.
- ▪
In its pure form, the subcutaneous, skin-only facelift has a limited effect on the position of heavier deep tissue.
- ▪
In SMAS plication, a skin flap is created with suture manipulation of the superficial fat and the underlying SMAS/platysma.
- ▪
In loop suture techniques (MACS-lift), a skin flap is created with long suture loops taking multiple bites of superficial fat and platysma – fixed to a single point on the deep temporal fascia.
- ▪
The supraplatysma plane creates a single flap of skin and superficial fat mobilized and advanced along the same vector.
- ▪
SMASectomy involves a skin flap plus excision of superficial fat and SMAS from the angle of the mandible to the malar prominence, with direct suture closure of the resulting defect.
- ▪
A SMAS flap raised with skin attached (deep plane) creates a flap of SMAS/platysma, superficial fat, and skin, all mobilized and advanced along the same vector.
- ▪
A separate SMAS flap (dual plane) creates two flaps, the skin flap and the superficial fat/SMAS/platysma, which are advanced along two different vectors.
- ▪
The subperiosteal lift involves dissection against bone, with mobilization and advancement of all soft tissue elements.
- ▪
Additional volume augmentation and, in some locations, volume reduction, should be considered in all cases of facelift surgery.
- ▪
Facial aging is usually a panfacial phenomenon. Therefore, in order to obtain a harmonious result, patients will often benefit from surgery to other components of their face.
- ▪
The most common complication of facelift surgery is hematoma. This problem should be dealt with promptly.
Keywords
Facelift, Rhitydes, Sagging, Jowls, Ageing, SMAS
Synopsis
- ▪
Age-related changes occur in all layers of the face, including skin, superficial fat, SMAS, deep fat, and bone.
- ▪
Patients presenting for facial rejuvenation surgery are usually middle-aged or older, thus increasing the chance of co-morbidities. Risk factors such as hypertension and smoking should be dealt with prior to facelift surgery.
- ▪
Careful preoperative assessment will provide the surgeon with an aesthetic diagnosis regarding the underlying facial shape, the age-related issues that predominate, and the appropriate surgical procedures for every individual patient.
- ▪
Almost all facelift techniques begin with a subcutaneous facelift flap. Careful incision placement, tissue handling, and flap repositioning are important in order to avoid the obvious stigmata of facelift surgery.
- ▪
In its pure form, the subcutaneous, skin-only facelift has a limited effect on the position of heavier deep tissue.
- ▪
In SMAS plication, a skin flap is created with suture manipulation of the superficial fat and the underlying SMAS/platysma.
- ▪
In loop suture techniques (MACS-lift), a skin flap is created with long suture loops taking multiple bites of superficial fat and platysma – fixed to a single point on the deep temporal fascia.
- ▪
The supraplatysma plane creates a single flap of skin and superficial fat mobilized and advanced along the same vector.
- ▪
SMASectomy involves a skin flap plus excision of superficial fat and SMAS from the angle of the mandible to the malar prominence, with direct suture closure of the resulting defect.
- ▪
A SMAS flap raised with skin attached (deep plane) creates a flap of SMAS/platysma, superficial fat, and skin, all mobilized and advanced along the same vector.
- ▪
A separate SMAS flap (dual plane) creates two flaps, the skin flap and the superficial fat/SMAS/platysma, which are advanced along two different vectors.
- ▪
The subperiosteal lift involves dissection against bone, with mobilization and advancement of all soft tissue elements.
- ▪
Additional volume augmentation and, in some locations, volume reduction, should be considered in all cases of facelift surgery.
- ▪
Facial aging is usually a panfacial phenomenon. Therefore, in order to obtain a harmonious result, patients will often benefit from surgery to other components of their face.
- ▪
The most common complication of facelift surgery is hematoma. This problem should be dealt with promptly.
Brief introduction
- ▪
The classic stigmata of the aging face include:
- •
Visible changes in skin, including folds, wrinkles, dyschromias, dryness, and thinning.
- •
Folds in the skin and subcutaneous tissue created by chronic muscle contraction: glabellar frown lines, transverse forehead lines, and crow’s feet over the lateral orbital rim.
- •
Deepening folds between adjoining anatomic units: the nasojugular fold (tear trough), nasolabial folds, marionette lines, and submental crease.
- •
Ptosis of soft tissue, particularly in the lower cheek, jowls, and neck.
- •
Loss of volume in the upper two-thirds of the face, which creates hollowing of the temple, the lateral cheek, and the central cheek.
- •
Expansion of volume in the neck and lateral jaw line, which leads to the formation of jowls and fullness of the neck ( Fig. 2.1 ) .
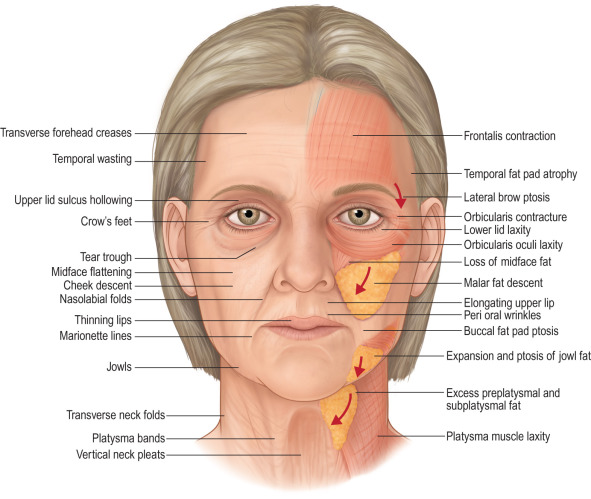
Figure 2.1
The aging face exhibits changes in the skin, superficial wrinkles, deeper folds, soft tissue ptosis, loss of volume in the upper third and middle third, and increased volume in the lower third.
- •
- ▪
Aging of the face occurs in all its layers, from skin down to bone; no tissue is spared. The surgical significance of this concentric layer arrangement is:
- •
Dissection can be done in the planes between the layers.
- •
Anatomical changes in each of the layers can be addressed independently, as required to treat the presenting problem.
- •
- ▪
Skin aging over time is both intrinsic and extrinsic. The net result is that facial skin loses its ability to recoil, a condition called elastosis.
- ▪
Intrinsic aging is the result of genetically determined apoptosis. The skin becomes thinner; there is a decrease in melanocytes, a reduced number of fibroblasts, and a loss of skin appendages. In the dermal matrix, there is fragmentation of the dermal collagen and impairment of fibroblast function.
- ▪
Extrinsic forces include sun exposure, cigarette smoke, extreme temperatures, and weight fluctuations.
- ▪
Important anatomic figures have been included ( Figs. 2.2–2.8 ) .
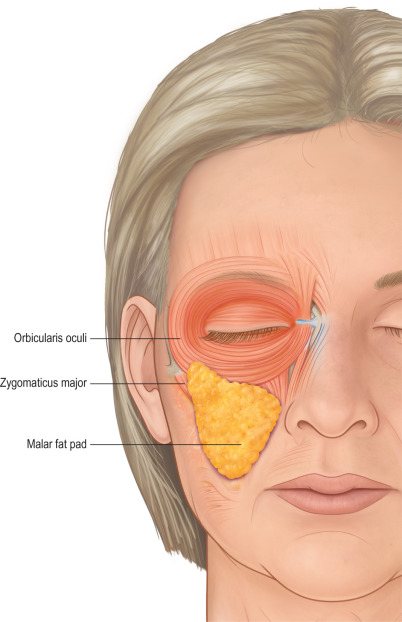
Figure 2.2
The malar fat pad is a triangular area of thickened superficial fat with its base along the nasolabial fold and its apex over the superolateral malar prominence.
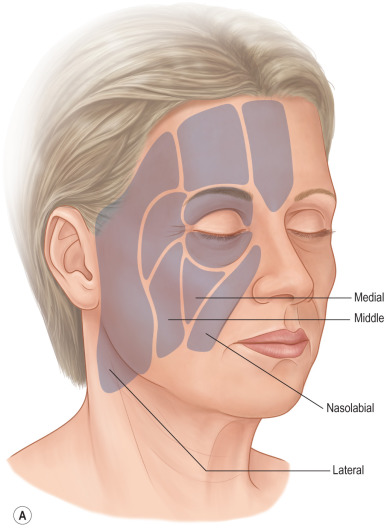
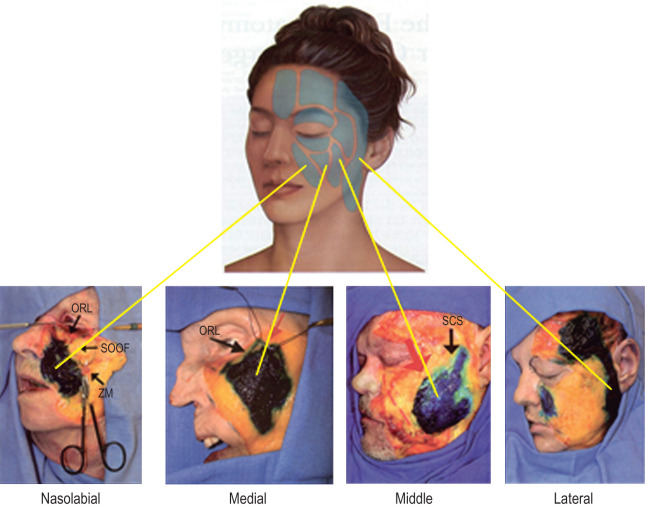
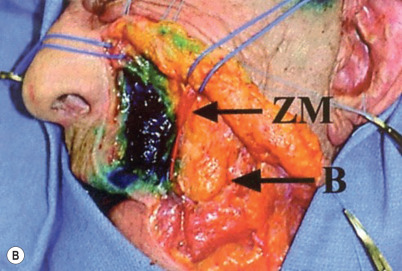
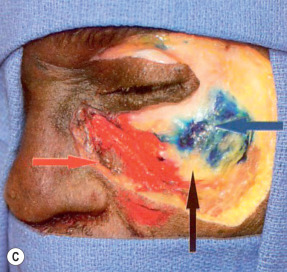
Figure 2.3
(A) Superficial facial fat is compartmentalized by vertically running septae. In the midcheek, from medial to lateral, these compartments are the nasolabial, medial, middle, and lateral compartments. The nasolabial and medial compartments make up the malar fat pad. (B) The deep facial fat is also compartmentalized by septae. The deep medial fat pad (here stained blue) is bounded above by the orbicularis retaining ligament, medially by the pyriform aperture, and laterally by the zygomaticus major (ZM) muscle and the buccal (labeled B) fat pad. (C) Over the body of the zygoma, the suborbicularis oculi fat (SOOF) is deep fat. It is seen here with a medial portion (yellow) and a lateral portion (stained blue). It is bounded medially by deep medial fat pad (stained red).
(A: Courtesy of Rohrich RJ, Pessa JE. The fat compartments of the face: anatomy and clinical implications for cosmetic surgery. Plast Reconstr Surg. 2007;119:2219–2227; B,C: Courtesy of Rohrich RJ, Pessa JE, Ristow B. The youthful cheek and the deep medial fat compartment. Plast Reconstr Surg. 2008;121(6):2107–2112).
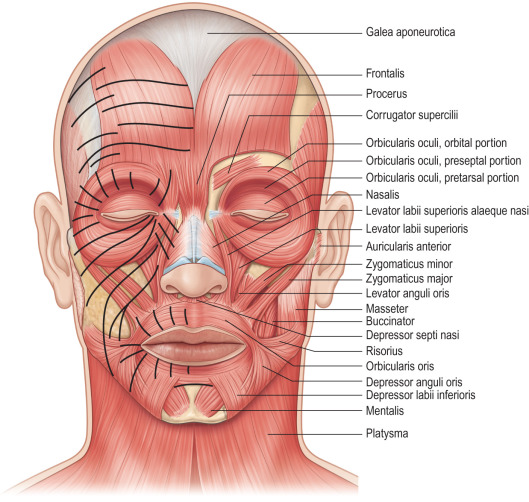
Figure 2.4
Muscles of facial expression. The solid lines demonstrate overlying skin creases caused by repeated contraction of the underlying muscles.
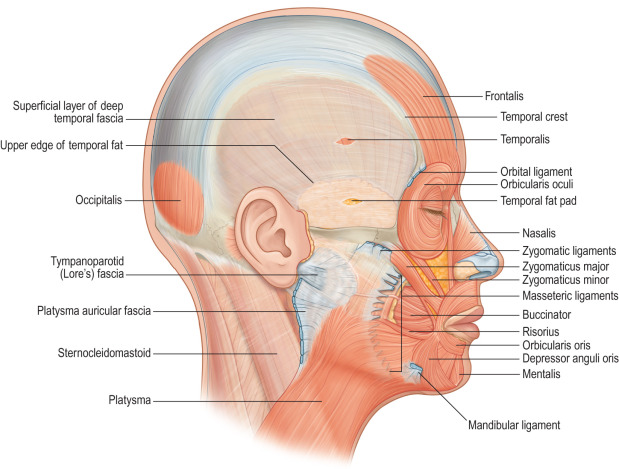
Figure 2.5
Facial soft tissue is tethered to underlying bone by the orbital, zygomatic, and mandibular ligaments. Soft tissue is tethered to underlying deep fascia by the masseteric cutaneous ligaments and by an area of attachment anterior and inferior to the earlobe, known by a number of different terms: platysma auricular ligament (Furnas), platysma auricular ligament (Mendelson), parotid cutaneous ligament (Stuzin), and a distinct area anterior to the earlobe known as Lore’s fascia.
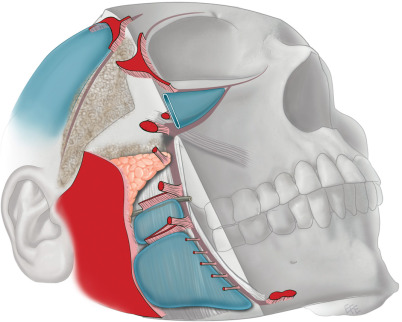
Figure 2.6
Mendelson’s interpretation of soft tissue attachments. The fixed posterior soft tissue is held in place by the platysma auricular fascia (large red area). The anterior face is fixed by a vertical column of attachments: orbital ligament, lateral orbital thickening (superficial canthal tendon), zygomatic ligaments, masseteric ligaments, and mandibular ligament. The so-called “fixed SMAS” is that portion attached to the parotid and the posterior border of the platysma. Anterior to this is the “mobile SMAS.”
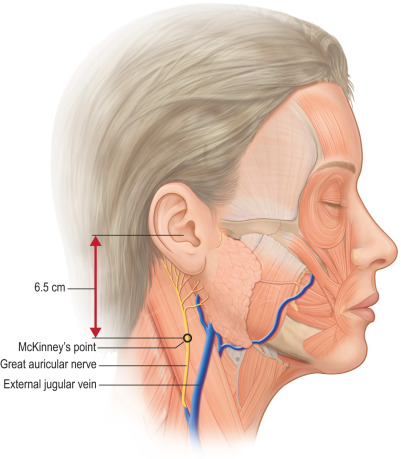
Figure 2.7
The great auricular nerve crosses the midportion of the sternocleidomastoid at McKinney’s point, which is 6.5 cm inferior to the external auditory canal. It usually travels about 1 cm posterior to the external jugular vein. Anterior to McKinney’s point, the nerve is covered by the superficial cervical fascia (SMAS), but at the posterior border of the sternocleidomastoid, the nerve is subcutaneous. The most common point of injury is at the posterior border of the sternocleidomastoid muscle.
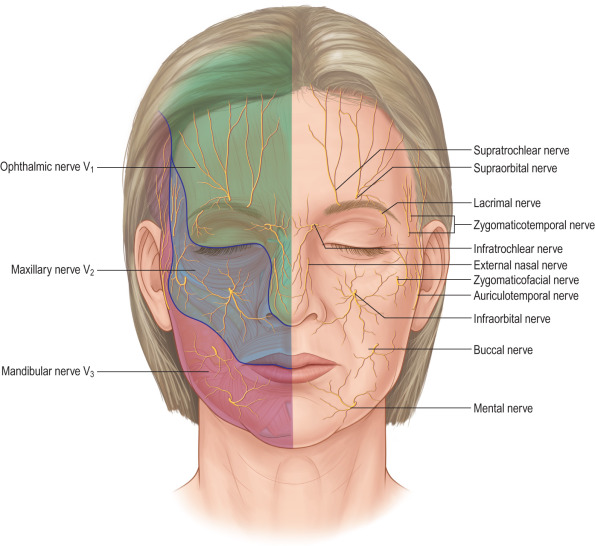
Figure 2.8
Major sensory nerves of the face.
Preoperative considerations
- ▪
The quality of surgical result will be affected by many patient-related factors, including the facial skeleton, the weight of facial soft tissue, the depth and location of folds, and the quality of the skin.
- ▪
Some issues can be reversed, others attenuated, and some may not be correctable at all.
- ▪
Incipient hypertension is common in the general population and can promote postoperative hematomas if it is not identified prior to surgery.
- ▪
Uncontrolled hypertension is a contraindication for surgery, while controlled hypertension is not a contraindication.
- ▪
Smokers have been shown to exhibit delayed wound healing due to microvasoconstriction and abnormal cell function.
- ▪
Nevertheless, there are significant short-term effects, which can be reversed by abstaining from tobacco use for 2–3 weeks prior to surgery.
- ▪
Prior to surgery, the entire face should be properly assessed.
- ▪
The face should be assessed as a whole – looking for the equality of facial thirds, the degree of symmetry, and the overall shape (round, thin, wide).
- ▪
Surgeons should develop an organized way to examine all the zones of the face: forehead, eyelids, cheeks, the perioral area, and the neck.
- ▪
With the diversity of surgical techniques available, a surgeon should think like a sculptor – considering the face in three dimensions with a view to adding tissue in some areas, removing tissue in other areas, and repositioning tissue where indicated.
- ▪
The ear should be examined with a thought to the potential placement of incisions.
- ▪
Important factors: the size and orientation of the earlobe, the angle of attachment of the tragus, the difference in character of the cheek skin and tragal skin, the size of the tragus, the density of the hair surrounding the ear, and the location of the hairline in the temple, the sideburn, and posterior to the ear.
- ▪
A careful assessment of the overlying skin is also important to determine if anything of a non-surgical nature is indicated before, during, or after facelift surgery.
- ▪
Excellent photographic documentation of the preoperative face is very important and should include frontal, oblique, and profile views. Other optional views include the smile and close-up views of the neck in repose and with platysma contracture.
Operative techniques
Subcutaneous facelift
- ▪
Classic procedure that tightens excess skin and relies completely on skin tension to shift underlying facial soft tissue against the force of gravity.
- ▪
Advantages: relatively safe, relatively easy to do, and patient recovery is rapid.
- ▪
Effective for the thin patient with excess skin and minimal ptosis of deep soft tissue.
- ▪
Disadvantage: skin placed under tension to support heavy underlying soft tissue will stretch, leading to a loss of surgical effect.
- ▪
Attempts to overcome this problem with excess skin tension may lead to distortion of facial shape, abnormal reorientation of wrinkles, and local problems at the incision line, including stretched scars and distorted earlobes.
Facelift incisions ( ; )
- ▪
In the temple area, the incision can be placed in the hair, at the anterior hairline, or a hybrid of the two, with an incision in the hair plus a transverse extension at the base of the sideburn ( Figs. 2.9A–B ) .
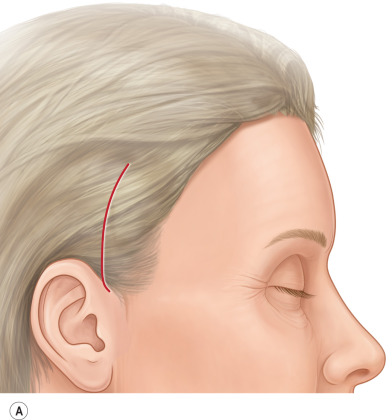
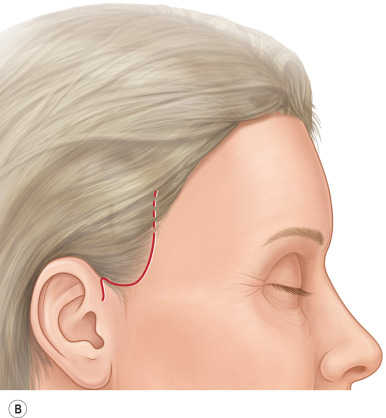
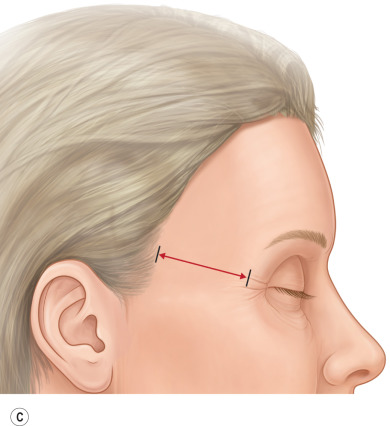
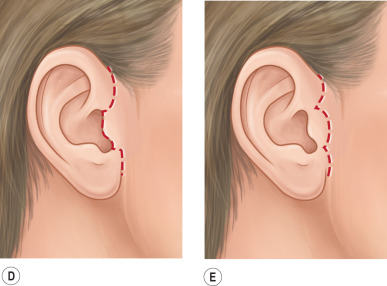
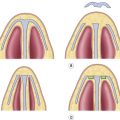
Figure 2.9
(A) The traditional hidden incision in the temple hair is appropriate when the temporal hairline will not be shifted adversely. (B) A temple incision along the hairline is used if a hidden incision will adversely shift the hairline. (C) The distance from the lateral orbital rim to the temporal hairline should not exceed 5 cm. (D) The retrotragal incision follows the edge of the tragus. (E) The pretragal incision is placed in the pretragal sulcus.
- ▪
The advantage of the incision in the hair is that it is hidden, but when the flap is drawn up, the anterior hairline and sideburn will shift; the degree of this depends on skin laxity.
- ▪
If the incision is placed at the anterior hairline, the scar is potentially more visible, but there will be no shift of the hairline.
- ▪
A transverse incision at the base of the sideburn is a compromise solution, which ameliorates much of the hairline shift while preserving a largely hidden scar.
- ▪
Several factors should be assessed before committing to an incision within the temple hair.
- ▪
A preoperative estimate of skin redundancy will give the surgeon some sense of how far the skin flap will move.
- ▪
The distance between the lateral orbital rim and the temporal hairline should be assessed.
- ▪
In youth, this distance is generally <4–5 cm, while in older patients, the distance increases.
- ▪
If the distance is already excessive, or if the expected movement of the temporal hairline will create a distance over 5 cm, then an incision in the hair should be avoided ( Fig. 2.9C ).
- ▪
Anterior to the ear, the incision can be pretragal or along the tragal edge ( Fig. 2.9D,E ).
- ▪
The advantage of the tragal edge incision is that it is hidden, but care must be taken to thin the flap covering the tragus in order to simulate a normal tragal appearance.
- ▪
Before committing to a tragal edge incision, the quality of tragal skin and that of facial skin must be compared; if the difference between the tragal skin and facial skin is too great, a tragal edge incision should be avoided.
- ▪
A pretragal incision is preferred in men, as the hair-bearing portion of the cheek skin will not be drawn up onto the tragus.
- ▪
Around the earlobe, the incision can be placed either in the cleft of earlobe attachment or 1–2 mm distal to the cleft, leaving a cuff of skin along the earlobe. This cuff will ease the process of insetting the earlobe on skin closure.
- ▪
In the retroauricular sulcus, the incision can be placed directly in the conchal groove as it courses superiorly.
- ▪
The incision is often carried as high as the level of the external auditory canal, or slightly higher, at the level of the antihelix.
- ▪
An extension of the retroauricular sulcus incision toward the occipital hair-bearing region should be made when there is a need to remove excess redundant neck skin.
- ▪
A “short scar” facelift is one that avoids the occipital incision, and will suffice for many patients.
- ▪
The principle objectives for the occipital incision are to gain access to the neck in order to take up redundant neck skin while making the incision as invisible as possible with little or no distortion of the occipital hairline ( Figs. 2.10 and 2.11 ).

Figure 2.10
(A) When there is minimal to moderate skin shift expected, an appropriate incision will curve from the retroauricular incision directly into the occipital hair. (B) When a greater amount of skin is to be excised, a “Lazy S” incision, which partly follows the occipital hairline, is an appropriate choice.
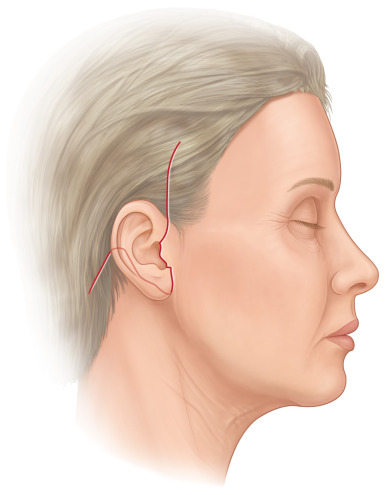
Figure 2.11
The traditional incision for a facelift flap curves vertically or slightly anteriorly in the temple, follows the contours of the ear, both anteriorly and posteriorly, and then angles into the posterior scalp.
- ▪
Either the temple dissection or the postauricular dissection can be done first, depending on surgeon preference.
- ▪
In the postauricular area, the flap is firmly attached to the deep cervical fascia of the sternocleidomastoid and the mastoid.
- ▪
This is the most common location to see skin flap necrosis, so the flap should be raised sharply under direct vision, keeping the dissection against the underlying deep fascia in order to maintain flap thickness.
- ▪
As the dissection continues inferior to the earlobe level, the surgeon must be cognizant of the great auricular nerve, where it is most at risk over the posterior border of the sternocleidomastoid.
- ▪
By keeping the dissection in the subcutaneous plane, the great auricular nerve will be protected.
- ▪
In the temple, if the incision has been made along the anterior hairline, dissection is begun directly in the subcutaneous plane. If the incision has been made in the hair-bearing scalp of the temple, dissection can be carried out in one of two planes: superficial to the superficial temporal (temporoparietal fascia), which will continue directly into the subcutaneous facelift plane, or between the superficial temporal fascia and the deep temporal fascia.
- ▪
If the deeper approach is used, the dissection proceeds quickly against deep fascia, but at the anterior hairline, the dissection plane must transition into the subcutaneous facelift plane.
- ▪
This change of plane results in a narrow ribbon of superficial temporal fascia, which will contain the superficial temporal artery and vein and branches of the auriculotemporal nerve, which must be divided ( Fig. 2.12A ) .
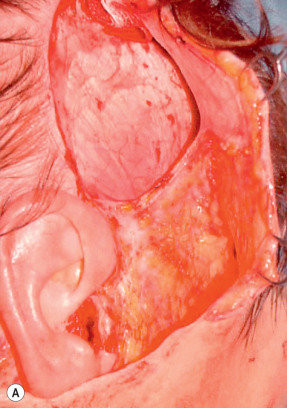

Figure 2.12
(A) Facelift flap has been raised in two different planes, initially deep to the superficial temporal fascia, against the deep temporal fascia (seen as an oval window), with a change of planes near the anterior temporal hairline into the subcutaneous plane. The “mesotemporalis” is a bridge of tissue that develops between these two planes. In order to unify the planes, it has been divided with ligation of the superficial temporal artery. (B) Facelift flap has been raised in a single subcutaneous plane, with dissection directly on the superficial temporal fascia and deep to the hair follicles of the scalp. The purple line outlines the course of the anterior branch of the superficial temporal artery.
- ▪
The superficial plane preserves the superficial temporal fascia and vessels, but can injure the hair follicles during the dissection unless care is taken ( Fig. 2.12B ).
- ▪
Anterior to the anterior hairline, the subcutaneous plane is then developed.
- •
The level of dissection normally leaves 1–2 mm of fat on the dermis.
- •
This results in a large random-pattern skin flap, the survival of which will entirely depend on the subdermal plexus.
- •
- ▪
In the upper face, this dissection continues anteriorly until the orbicularis oculi is encountered, where it encircles the lateral orbital rim. Depending on the type of deep plane surgery planned, the midcheek dissection may stop short of the malar fat pad or, alternatively, carry on over the fat pad, freeing it from the overlying skin in the temple and cheek.
- ▪
Lower in the cheek, immediately anterior to the ear and the earlobe, the skin is tethered to underlying structures by secure fascial attachments, but beyond this area, the subcutaneous dissection proceeds relatively easily.
- ▪
Once the skin flaps anterior and posterior to the ear have been raised, the two dissections are joined.
- ▪
The dissection can then be extended into the neck as far as the technique requires ( Figs. 2.13 , 2.14 ) . ( )
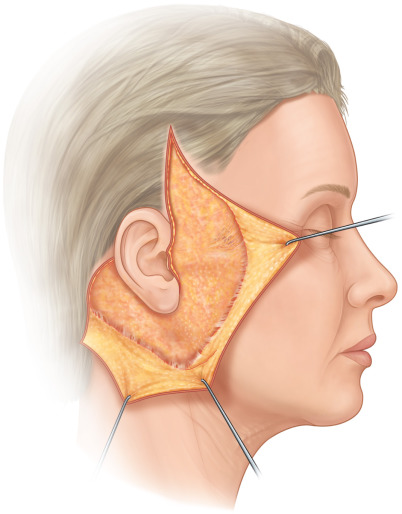
Figure 2.13
Subcutaneous facelift flap has been raised.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree